
11 November 2019
Karl Bloxham
[FYI request #11463 email]
Tēnā koe Karl
Your Official Information Act request, reference: 002142
Thank you for your email of 16 October 2019, asking for the following information under the Official
Information Act 1982 (the Act):
1.
I would like to request a copy of the following form;
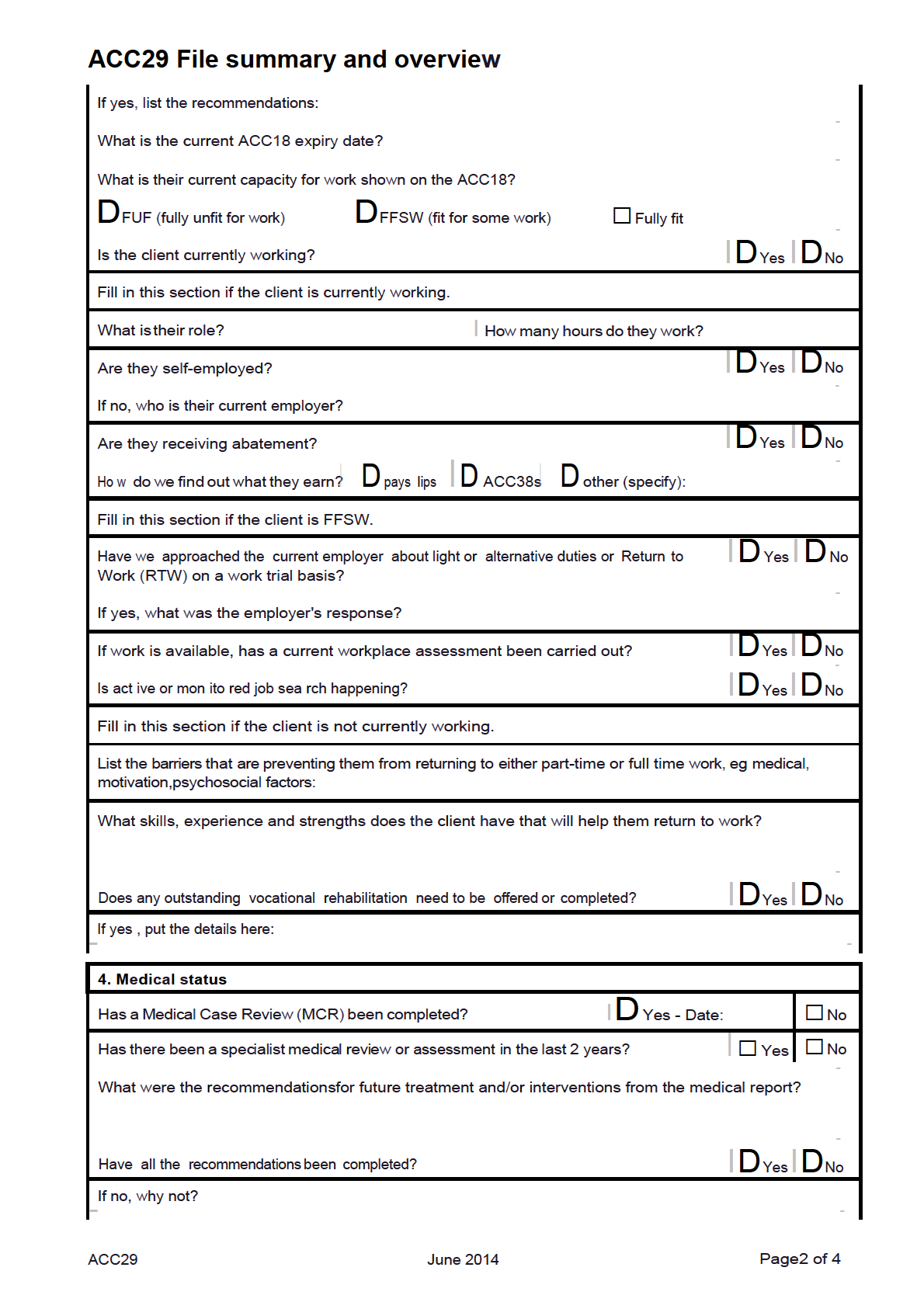
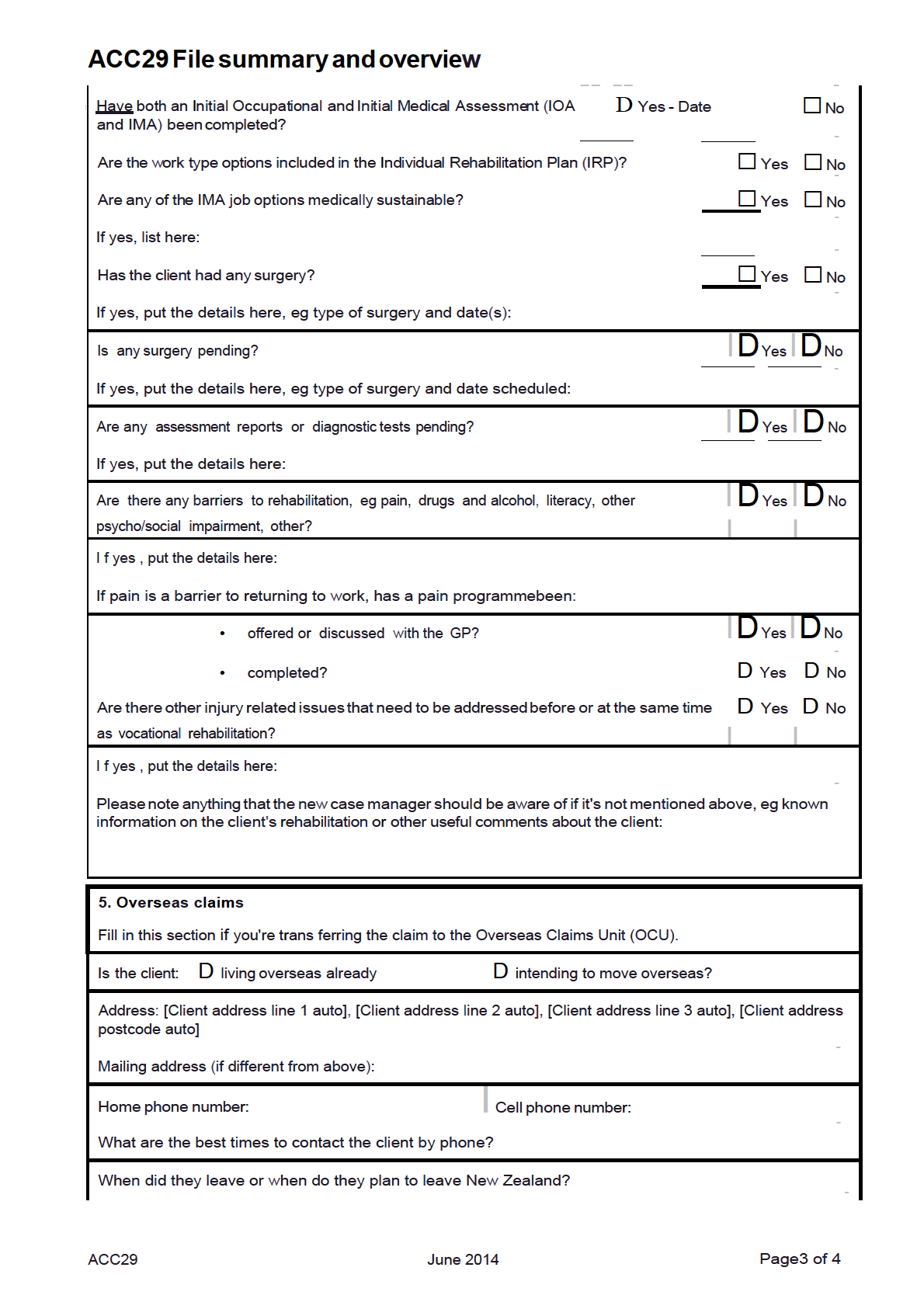
ACC29
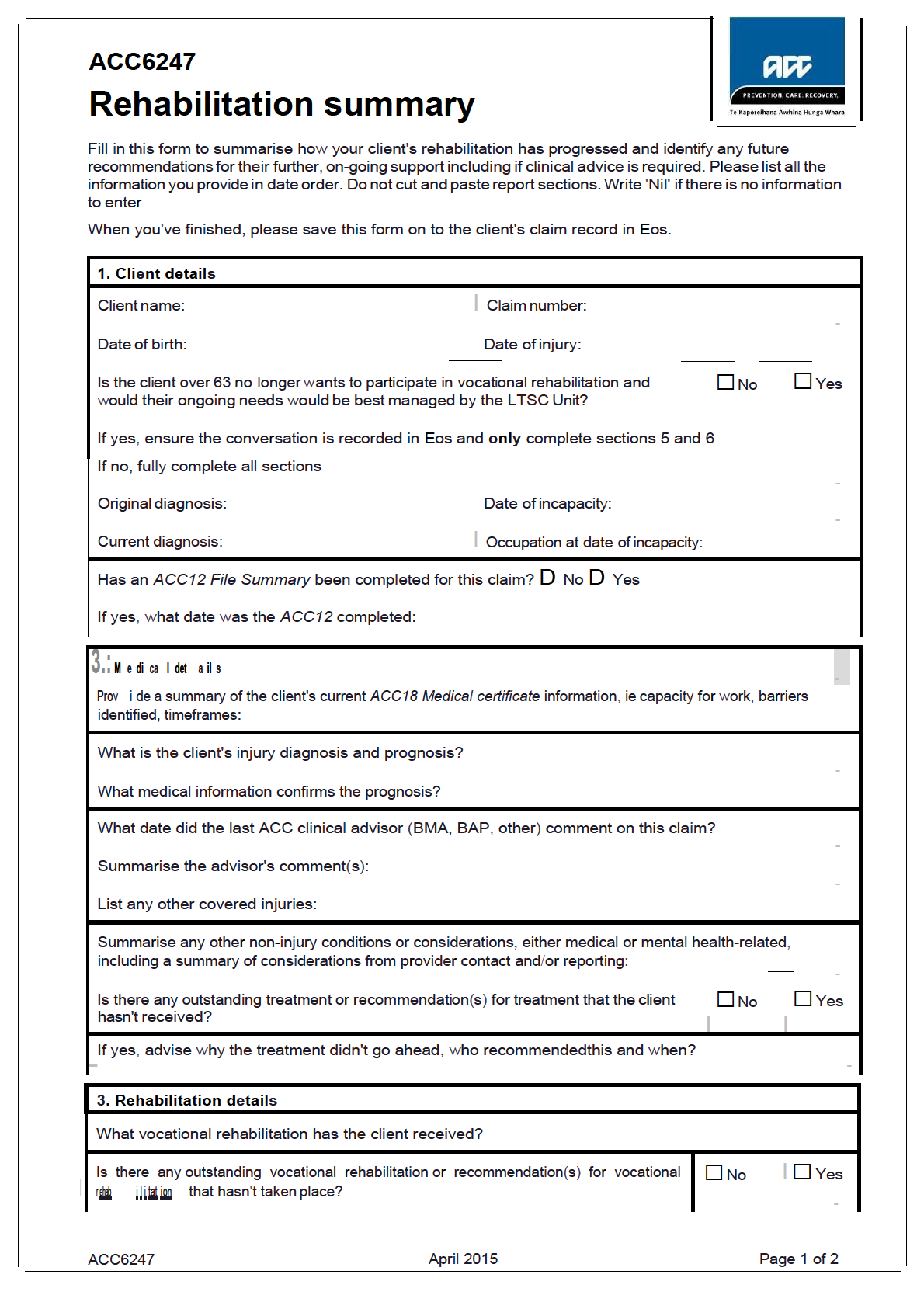
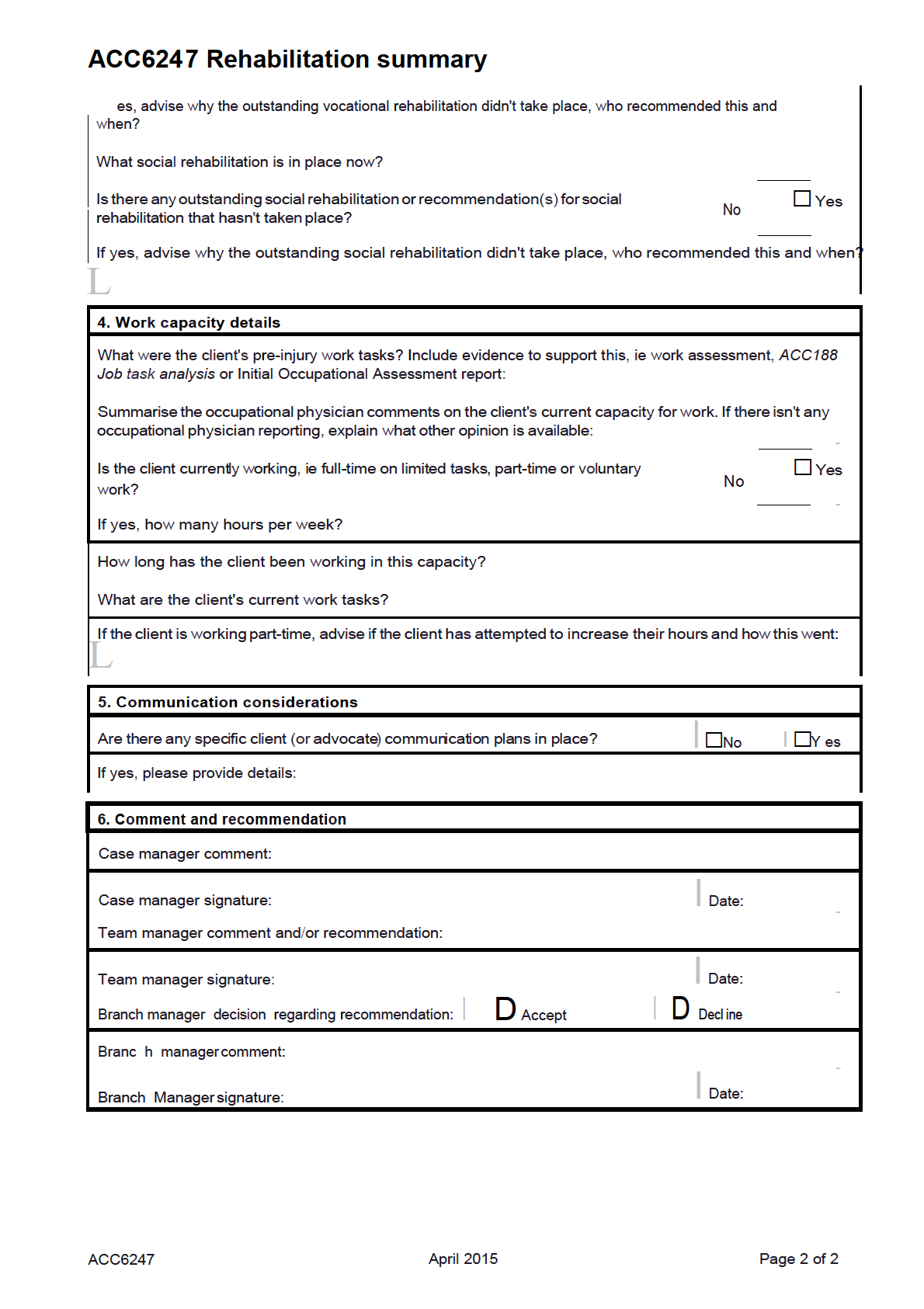
ACC6247
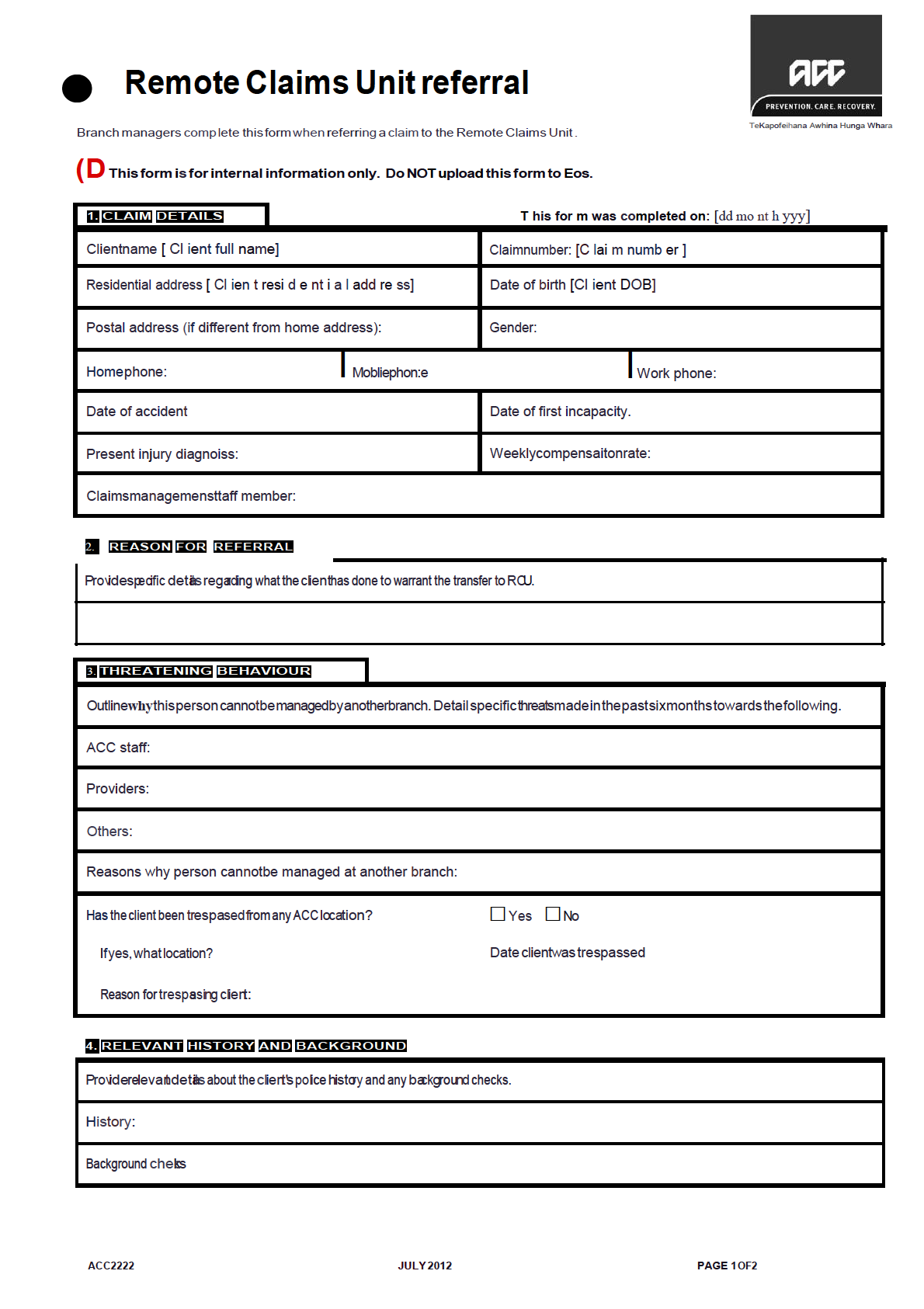
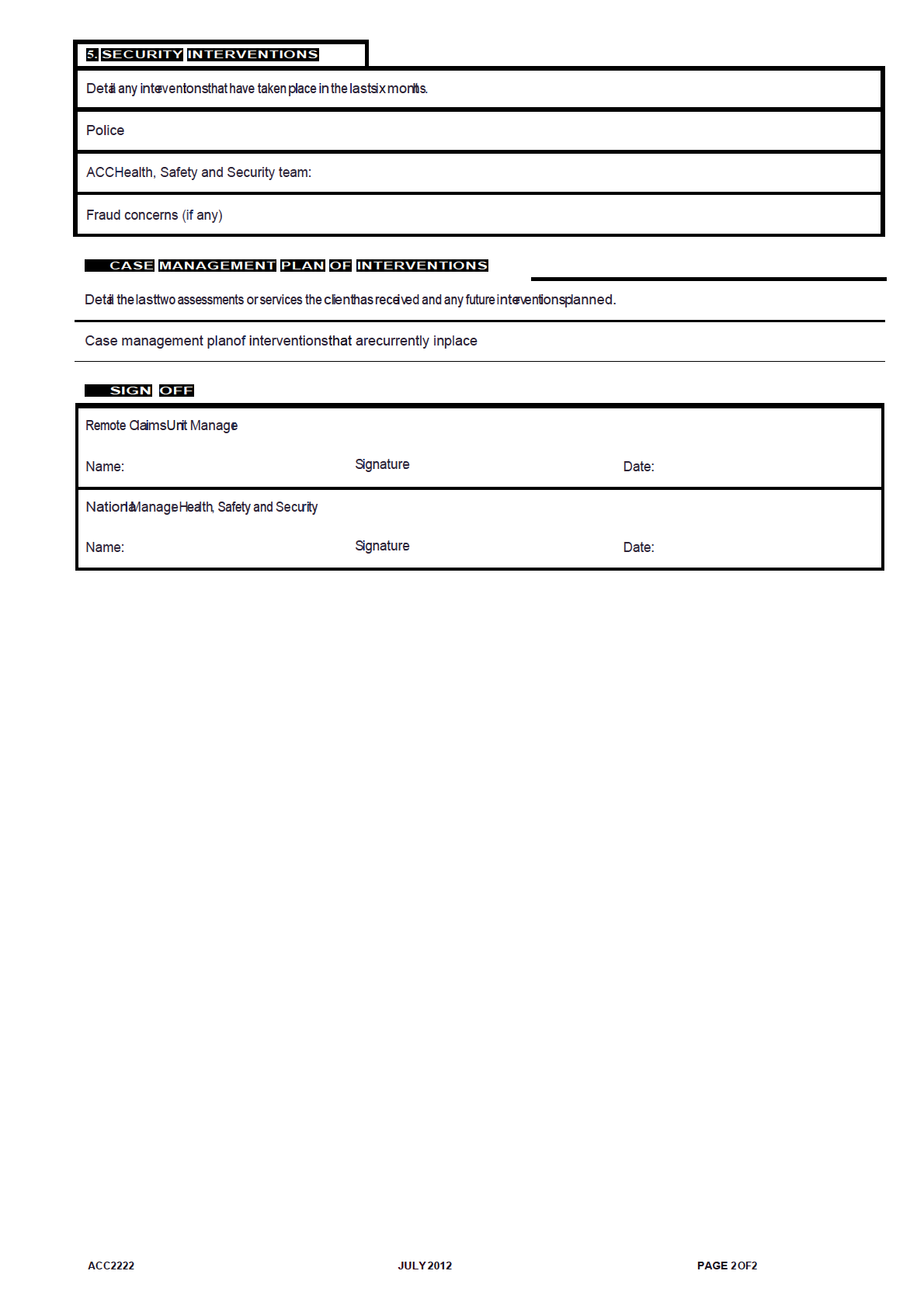
ACC2222
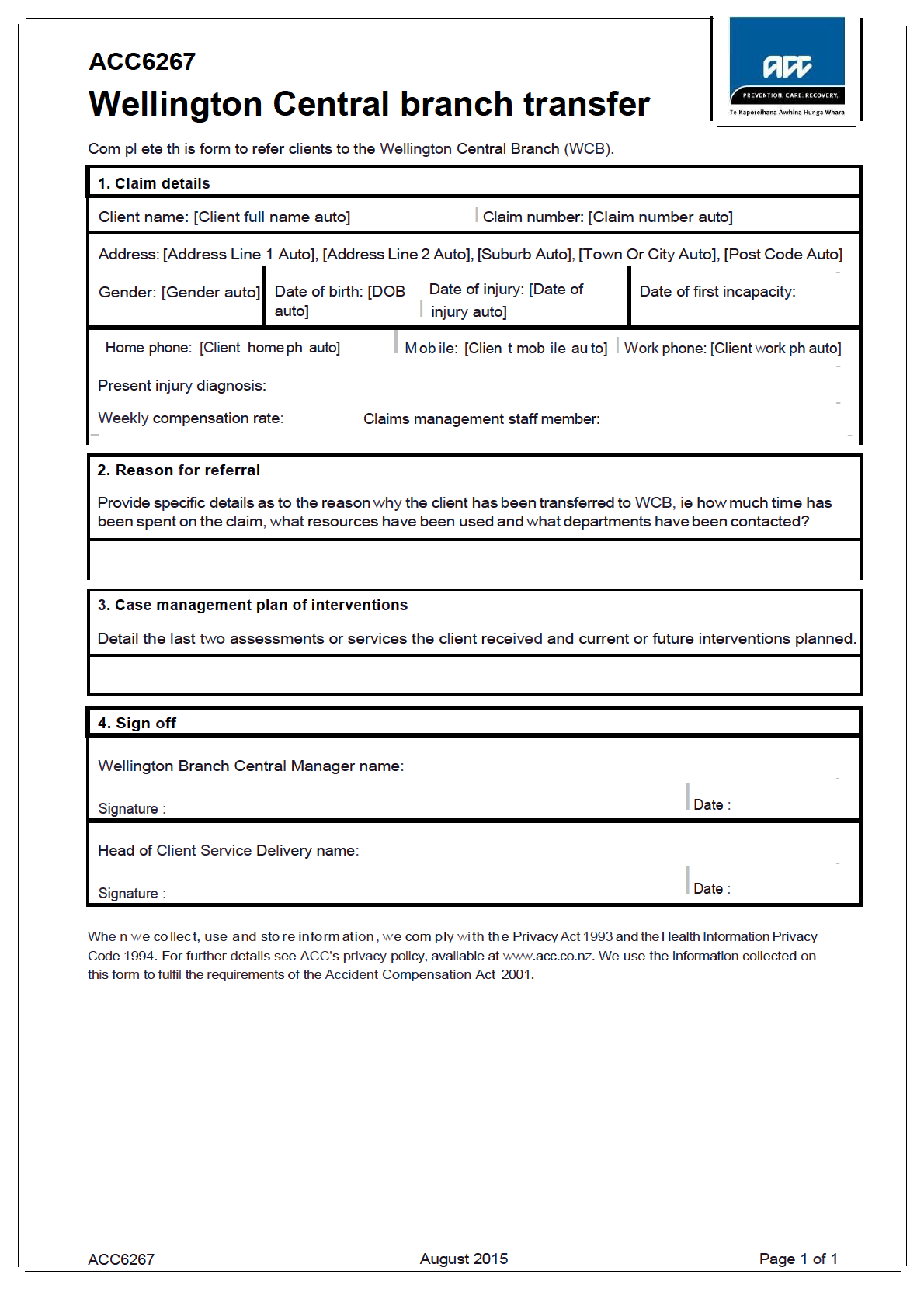
ACC6267
Attached are the forms you requested.
If you have any questions, you can email me at
[email address] Nāku iti noa, nā
Emma Coats
Manager Official Information Act Services
Government Engagement & Support
 ACC29
File summary and overview
ACC29
File summary and overview
Fill in this form if you're a case owner and you need to transfer a claim to another branch or the Overseas
Claims Unit. Upload it to the client's claim in Eos when you've finished.
1. Client details
Client name: [Client full name auto]
I Claim number: [Claim number auto]
Date of birth: [Client date of birth auto]
_ Do they have an advocate?
Yes I D _No
l3.:1njury , reh a bilit a ti o n a nd e ntitl e m e nt s
Injury: [Injury auto]
I Date of injury (DOI): [DOI auto]
Occupation at date of injury: [Occupation at date of injury auto]
-
Diagnosis at time of injury:
Current diagnosis:
List the covered injuries:
Are there any significant non-injury factors that may have an effect on this claim?
Yes I □No
If yes, put the details here:
Are there any other claims that may have an effect on this claim?
□ □
Yes
No
-
If yes, put the details here:
-
Is there a signed Individual Rehabilitation Plan (IRP) on file?
□ □
Yes
No
If yes, does it need updating?
□ □
Yes
No
-
IRP expiry date:
I Outcome date:
I Date of next monitoring step:
Tick the ongoing current entitlements that the client is receiving:
D Abatement
D Attendant care
D Training for independentliving (TIL)
D Child care
D Education support
D Transport for independence
-
D Sleepover
I D Home help
D Vocational rehab, eg work trial etc:
D Weekly compensation at$
pw
D Other (specify):
-
If we're providing any social rehabilitation assistance, eg hours of care, education support etc, put the details
I here:
-
3. Work capacity
Date of incapacity:
I Date of subsequent incapacity:
Has the client worked at all since the injury?
I D Yes I D No
If yes, what type of work have they been doing?
-
Has capacity to return to their pre-injury employment been assessed?
D
□
Yes - Date:
No
ACC29
June 2014
Page1 of 4
ACC29 File summary and overview
6. Summary
What are the next steps needed for the client's rehabilitation?
1:
-
2:
3:
-
4:
5:
-
6:
7. Your name and signature
Case manager/team manager name: [Staff member auto]
Signature:
I Date:
When we collect, use and store information, we comply with the Privacy Act 1993 and the Health Information Privacy
Code 1994. For further details see ACC's privacy policy, available at www.acc.co.nz. We use the information collected on
this form to fulfil the requirements of the Accident Compensation Act 2001.
ACC29
June 2014
Page4 of 4
Document Outline