Minutes:
Technical Advisory Group for COVID-19
Date:
Minutes:
Technical Advisory Group for COVID-19
Date:
Friday 12 June 2020
Time:
10.30am – 11.30am
Location:
Zoom Meeting
Chair:
Dr Ian Town
ACT 1982
Members:
Dr Sally Roberts, Prof Michael Baker, Dr Nigel Raymond, Dr Virginia Hope, Dr Shanika
Perera, Prof David Murdoch, Dr Bryan Betty, Prof Stephen Chambers, Dr Matire
Harwood, Dr Anja Werno, Dr Patricia Priest, Dr Erasmus Smit, Dr Collin Tukuitonga
Ministry of Health staff - Dr Caroline McElnay, Dr Harriette Carr, Dr Tomasz Kiedrzynski,
Dr Juliet Rumball-Smith, Dr Niki Stefanogiannis, Dr Richard Jaine, Andi Shirtcliffe, Asad
Abdul ahi, Margaret Broodkoorn, Louise Chamberlain
Guests
Maria Turley, Cathie McGachie
INFORMATION
Apologies:
-
1.0 Welcome and Previous Minutes
Dr Ian Town welcomed all Members, Attendees and Guests in his capacity as Chair of the Technical
Advisory Group for COVID-19.
Minutes of the last meeting (5 June 2020) were accepted subject to the following correction being
made to item 4.1 Managing respiratory illnesses over winter:
•
Many people do not have sick leave, so will not be able to stay home, regardless of messaging
General y, Subgroups support the current guidance, but acknowledge compliance wil be an issue and that communications
need to be clear
•
Many people do not have sick leave, so will not be able to stay home, regardless of messaging. Financial support should be
provided if necessary, for people to stay home when sick or while awaiting a test result
General y, Subgroups support the current guidance, but acknowledge people’s ability to comply wil vary. Communications
need to be clear
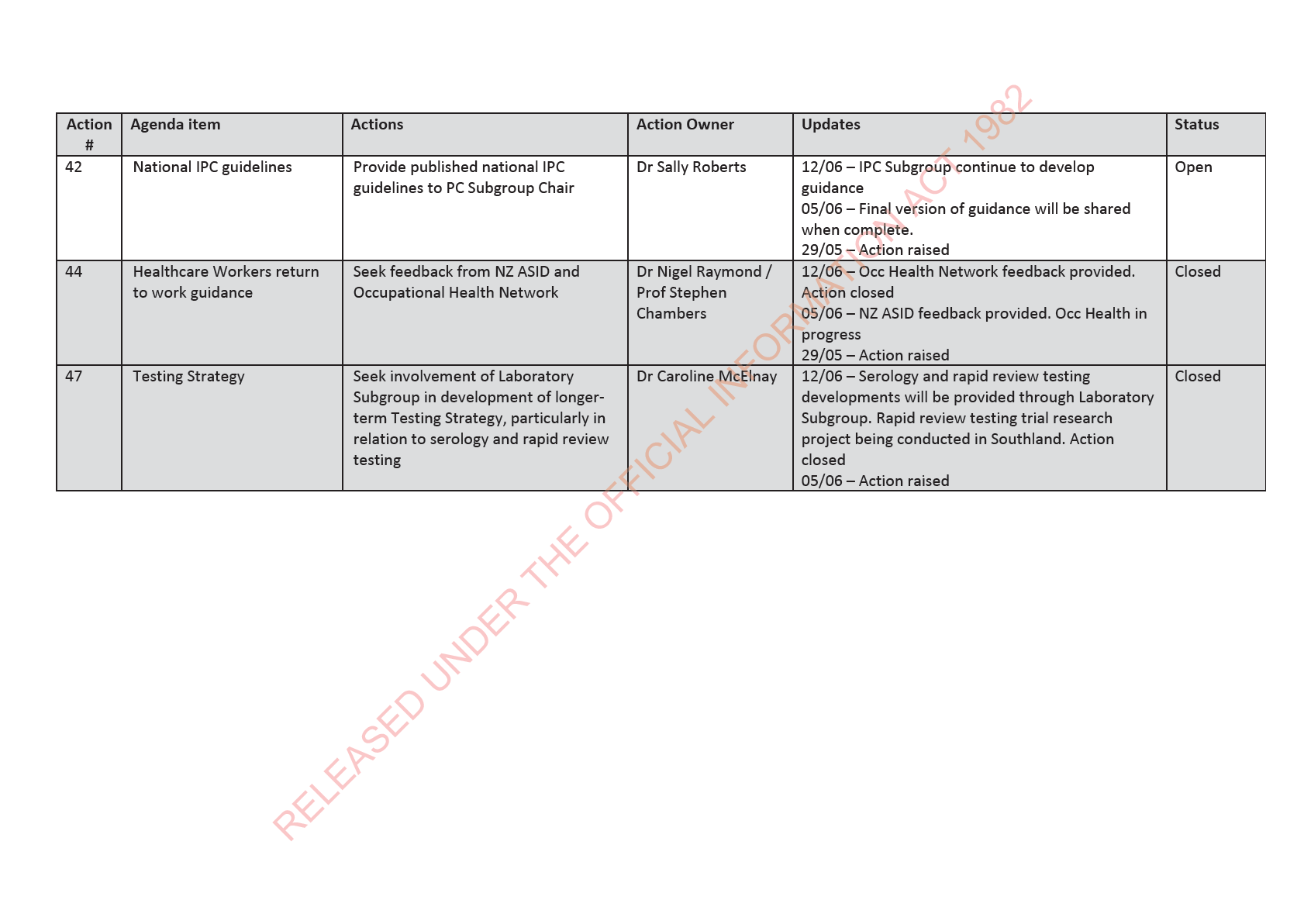
2.0 Update on open actions
Open actions updated. Action 42 remains open. Actions 44 and 47 closed.
3.0
Ministry of Health update on COVID-19 response
On behalf of the Ministry, the Chair thanked and acknowledged TAG and Subgroup members for all
RELEASED UNDER THE OFFICIAL
the expertise, support and encouragement provided to the response to date.
The Chair gave an update on current issues being worked on in Ministry of Health, include:
o Ministry now planning resourcing and the strategy for preparedness phase of the pandemic
the country is now entering. Considering lessons learnt as input into planning.
o All of Government (AOG) Team continue to focus on a range of complex issues including
border management and control
o Once scenarios have been confirmed desktop exercises are being planned to stress test
various elements including contact tracing
o MBIE lead Vaccine Task Force has now formally met. A Science and Technical Advisory Group
is to be established to develop Vaccine Science Strategy across international research and
funding organisations
o A range of internal Ministry reviews are being considered including an Executive Leadership
Team review of roles and responsibilities during the response.
4.0 Healthcare workers return to work guidance
TAG was presented with return to work guidance for Healthcare Workers (HCW) infected with SARS-
CoV-2 or who are close contacts with a person infected with SARS-CoV-2.
Guidance has been developed by the Infection and Prevention Subgroup and contributed to by
Clinical and Public Health Subgroups.
ACT 1982
Noted this is area experiencing rapidly changing advice in other countries. Recent recommendations
from Public Health England and Australian PHLN have removed the need for PCR testing at the end
of the isolation period. The group was asked if we should follow suit.
Feedback sought from TAG on support of the removal of the requirement for 2nd PCR test at day 10
prior to release from isolation, except for HCW returning to work who:
• provide direct patient care;
• were close contacts of a confirmed case of COVID-19 infection and have been in quarantine
for 14 days
INFORMATION
TAG feedback:
• In favour of reducing number of PCR tests required
• Positive PCRs add confusion, even when at high CT value
• HCW and general public advice should be consistent and consider equity
• Advice must be presented with simple easy to understand messaging eg: low prevalence;
why to some people need to be tested and not others?
• Risk of infectiousness becomes lower over time - there can be a gap between isolation
release and returning to work for those with ongoing symptoms eg: do not want HCW
returning to work stil coughing but there would not be a requirement for them to be in
strict isolation
• Often ARC HCW are older women and on low income and cannot afford additional time off
work if long stand down required
• Target groups which may be more risk adverse, for groups where absolute confirmation is
required
TAG supported a further revision to the HCW RTW algorithm which will no longer include PCR
testing at day 10. Updated algorithm to be circulated by email.
4.1 Clinical algorithm
RELEASED UNDER THE OFFICIAL
TAG was presented with a clinical algorithm, developed by the Public Health Subgroup. Has been
developed as a tool to accompany the implementation of the changes in case definition and the
implementation of the Testing Strategy; to demonstrate logic, confirm context, identify gaps and
issues.
Appreciation given to all Subgroups for their feedback and recommendations (taken as read), which
have been incorporated into the algorithm. Any further feedback is invited to the Public Health
Subgroup.
Primary Care:
• Strong primary care sector feedback - If broad based surveillance testing is required, a
statement is required on epidemiologic criteria (not ILI approach)
• Surveillance testing capacity concerns through winter – need practical approach for
general practice. Surveillance testing won’t be done if not practically workable
• People are now refusing tests; do not understand why testing is required as currently low
risk of community transmission – urgent need for public communications
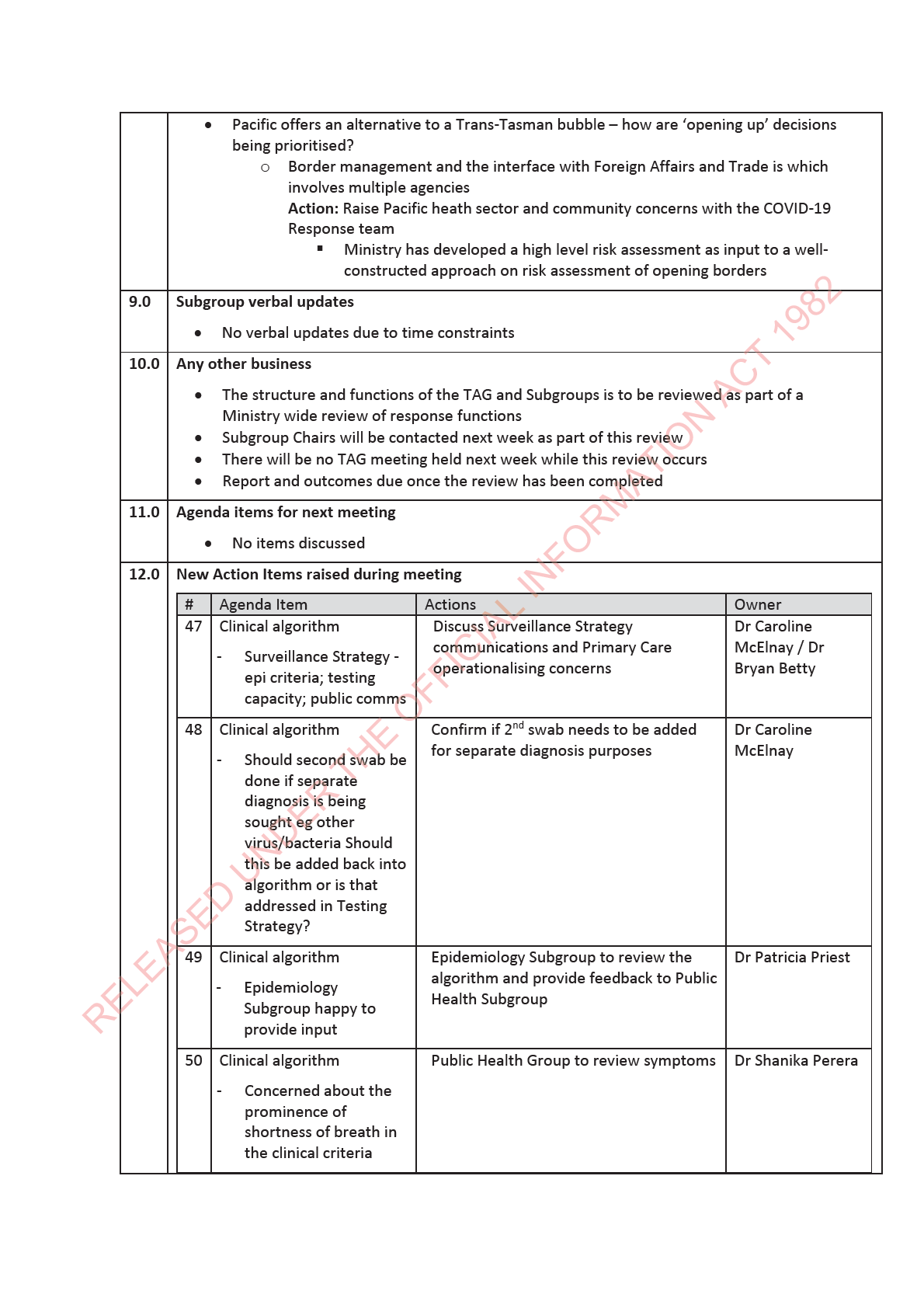
Action: Discuss Surveillance Strategy communications and Primary Care operationalising
concerns
Laboratory:
• Should second swab be done if separate diagnosis is being sought eg other virus/bacteria
Should this be added back into algorithm or is that addressed in Testing Strategy?
ACT 1982
Action: Confirm if 2nd swab needs to be added for separate diagnosis purposes
Epidemiology:
• Subgroup happy to provide input
Action: Epidemiology Subgroup to review the algorithm and provide feedback to Public
Health Subgroup
Clinical • Extensive testing for surveilance is not a usual clinical pathway.
INFORMATION
• Concerned about the prominence of shortness of breath in the clinical criteria
•
Action: Public Health Group to review symptoms
Urutā
• Welcome opportunity to provide feedback
Action: Consider and provide feedback to Public Health Subgroup
Ministry currently working on bringing together communications and operationalisation of changes
to case definition, testing strategy, arrangements and opportunities for testing as a package to take
effect within the next 2 weeks.
Noted - Testing Strategy which has been reviewed by TAG includes asymptomatic testing and ILI
surveillance.
5.0
PPE requirements for COVID-19 Nasopharyngeal or Throat swabs
TAG was presented with PPE requirements for COVID-19 Nasopharyngeal or Throat swabs advice,
developed by the IPC Subgroup.
Advice is based on IPC best practice with staff safety being top priority. Subgroup also considered
impacts of implementing and operationalising any advice.
RELEASED UNDER THE OFFICIAL
Noted Appendix 1: Current advice on Ministry website regarding PPE for staff taking NP/Throat
swabs from people with suspected COVID-19 infection will be replaced with updated Level 1 advice
which IPC Subgroup is currently developing.
TAG feedback:
Primary Care:
• Require evidence base for full PPE requirements; what is the epidemiologic basis?
• Effective PPE use is linked to Surveillance Strategy and how that is operationalised -
strong feedback received from sector particularly within community medicine
• Must consider the practicalities of supply, capacity and efficiencies in a primary care
setting eg:
o Some DHBs have now stopped PPE supply into general practice
o CBACs are now being reduced
o Donning and doffing requirements
o Some DHBs are now publishing their own contrary advice
Action: Primary Care Subgroup review advice and provide feedback to IPC Subgroup
Action: Primary Care Subgroup to provide advice to Ministry on operationalisation and
communication of this advice and the wider Surveillance Strategy
6.0 Infected Healthcare Worker data analysis
ACT 1982
TAG was presented with infected healthcare work data analysis, fol owing feedback given on a
previous version.
Analysis summary:
• Over half HCW infections were likely to be contracted in the workplace
• Most HCW did not transmit infection to others
• The majority of all transmissions between HCW, patient, resident occurred in ARC
• Key finding – as most infections were in ARC facilities there were not many instances of
INFORMATION
transmission via HCW to other health professionals
• Analysis is currently quantitative
TAG feedback:
• Query whether the number of contact exposures had been defined, considering the
closeness of contact in ARC facilities
o This couldn’t be picked up through current quantitative data (EpiSurv) and would
need to be part of further review eg: interviews
• IPC Subgroup interested in reviewing data on HCW who acquired the infection in the
healthcare setting; this will inform system error themes
•
Action: ODPH is planning a more detailed review of the data over the next 3 months with
support from the Clinical Subgroup
7.0 Māori health perspectives
• Many Māori health providers have concerns around PPE and IPC
• Continuing to advocate for swabs for children. Level of testing remains inconsistent
• Continue to monitor the impact of lockdown / deferred care
o Previous feedback provided on this issue has resulted in specific questions being
added to a NZ Health Survey on Deferred Care, commissioned by Director General
of Health
RELEASED UNDER THE OFFICIAL
Pacific health perspectives
• There is some confusion among the Pacific health sector and wider community about
border management ie: borders are closed but many people are returning; managed
isolation breaches are being reported; flights beginning to Japan. Clarification guidance is
required
51 Clinical algorithm
Urutā to review the algorithm and
Dr Matire
provide feedback to Public Health
Harwood
Subgroup
52 PPE requirements for
Primary Care Subgroup review advice and Dr Bryan Betty
COVID-19 Nasopharyngeal provide feedback to IPC Subgroup
or Throat swabs advice
53 PPE requirements for
Primary Care Subgroup to provide advice Dr Bryan Betty /
COVID-19 Nasopharyngeal to Ministry on operationalisation and
Dr Sally Roberts /
or Throat swabs advice
communication of this advice and the
Dr Caroline
wider Surveillance Strategy
McElnay
54 Infected Healthcare
ODPH is planning a more detailed review Dr Niki
Worker data analysis
of the data over the next 3 months with
Stefanogiannis
ACT 1982
support from the Clinical Subgroup
55 Border management
Raise Pacific heath sector and community Chair
concerns with the COVID-19 Response
team
13.0 Summary of TAG Recommendations
• Healthcare workers return to work guidance - TAG supported a further revision to the HCW
RTW algorithm which will no longer include PCR testing at day 10
INFORMATION
14.0 Meeting closed at 11.30am
Next meeting Friday 26 June 10.30am – 11.30am
RELEASED UNDER THE OFFICIAL