



133 Molesworth Street
PO Box 5013
Wellington 6140
New Zealand
T+64 4 496 2000
8 July 2021
NZ Health Justice
By email:
[FYI request #15556 email]
Ref: H202106408
Tēnā koe NZ Health Justice
Response to your request for official information
Thank you for your request under the Official Information Act 1982 (the Act) on 25 May 2021 for
information pertaining to audits, certification and surveil ance of HealthCare NZ Limited.
On 22 June 2021, the due date for responding to your request was extended under section 15A
of the Act as further consultation was required.
Information in response to each part of your request is as follows. The table in Appendix 1 also
outlines the documents for release.
“A timetable of certification, surveil ance and verification audits of HealthCare NZ Limited
under NZS 8158:2012 since 2017”
The Ministry of Health (the Ministry) does not formally receive the audit schedule timetables
from the conformity assessment bodies (CABs) for Home and community providers. However,
we note the following audits have occurred and are pending for Healthcare of New Zealand
Holdings Limited:
• June 2017 certification audit
• 2017 verification audit
• March 2019 surveil ance audit
• 2020 certification audit is pending (deferred due to COVID-19 pandemic).
“A copy of the most recent certification, surveil ance or verification audit undertaken of
HealthCare NZ Limited under NZS 8158:2012;” and “An explanation of how these audits
are completed and the Ministry's role”
Please refer to Document 1 attached to this letter for a copy of the ‘
Home and Community
Support Services Audit Report’.
It is important to note that HealthCERT does not regulate or certify Home and Community
Support Services (HCSS) providers under the Health and Disability Services (Safety) Act 2001.

HealthCERT’s role is to provide an administrative function in terms of maintaining a central
repository for home and community provider audit reports (where they are funded) and to help
facilitate review of certification audit reports between the Independent Assessment Commit ee
and the CAB.
Further information regarding the requirements for CABs that are auditing and certifying
providers of HCSS against the HCSS Standard (NZS 8158:2012) is publicly available on the
Ministry website:
www.health.govt.nz/publication/auditing-requirements-home-and-community-
support-sector-standard-nzs-81582012.
The Ministry also contracts service providers to provide HCSS through a Needs Assessment
Service Coordination (NASC) service. Ministry-funded HCSS help disabled people to live at
home and include household management and personal care. Further information about this is
available at the following address:
www.health.govt.nz/your-health/services-and-
support/disability-services/types-disability-support/home-and-community-support-services.
“A copy of any formal correspondence addressed to the Ministry under section 59 of the
Health & Disability Commissioner, or other relevant provisions of the Act, in respect of
HealthCare NZ Limited in the past 12 months. Where any such referrals have been made,
please disclose what follow-up action the Ministry has taken. If no action has been taken
then please provide an explanation.”
Please refer to Documents 2 to 8 for information within scope of this part of your request. These
documents are listed in Appendix 1 with copies enclosed. The table in Appendix 1 also lists the
specific grounds under which information has been withheld.
I trust this information fulfils your request. Please accept my apologies for the delay in providing
this information.
Under section 28(3) of the Act you have the right to ask the Ombudsman to review any
decisions made under this request. The Ombudsman may be contacted by email at:
[email address] or by cal ing 0800 802 602.
Please note that this response, with your personal details removed, may be published on the
Ministry website at:
www.health.govt.nz/about-ministry/information-releases/responses-official-
information-act-requests.
Nāku noa, nā
Emma Prestidge
Group Manager, Quality Assurance and Safety
Health System Improvement and Innovation
Page 2 of 3
Appendix 1: List of documents for release
# Date
Title
Decision on release
1 March 2019
Home and Community Support
Services Audit Report
2 September 2020 Letter from the Health and
Disability Commissioner to the
Director General of Health
3 November 2020
Letter from the Health and
Released with some information
Disability Commissioner to the withheld under section 9(2)(a) of the
Chief Executive Officer of
Act, to protect the privacy of natural
HealthCare NZ
persons
4 November 2020
Letter from the Health and
Disability Commissioner to the
Director General of Health
5 2020
Summary table of complaints
raised against HealthCare NZ
6 2020
Updated table of complaints
raised against HealthCare NZ
7 February 2021
Memorandum: Update to
Deputy-Director General about
actions taken in response to
HDC complaint dated 23
September
Released in full
8 2021
Excerpt of quality record
minutes about actions taken in
response to the HDC complaint
Page 3 of 3

Document 1
Home and Community Support Services Audit Report
Home and Community Support Services Audit Report (version 1.0)
Introduction
This audit was conducted against the Home and Community Support Sector Standard 8158:2012. Instructions:
•
Refer to the Conformity Assessment Body document for Home and Community Support Services audits.
•
When completing this template standard level reporting is used i.e. criteria only have evidence reported where there is a non-conformity or
1982
continuous improvement (fully attained ratings do not have evidence reported at criterion level).
•
For a surveillance audit: refer to paged 6-7 of the Conformity Assessment Body document for Home and Community Services audits.
THE
•
A recommendation is an opportunity for improvement for a fully attained criterion.
•
ACT
Sample totals: these represent staff employed, total FTE and number of consumers receiving services across the total organisation (not just
the audited sites).
•
Submit the final report together to the Ministry of Health (refer separate instructions).
It is important that auditors restrict their editing to the content controls in the document and do not delete any content controls or any text outside
UNDER
the content controls.
Audit Report
Supplier name:
Healthcare of New Zealand Holdings Limited
Contract name(s):
Healthcare of New Zealand Holdings Limited (HCSS)
Contracts held with:
ACC; Ministry of Health; Auckland; Counties Manukau; Lakes; Bay of Plenty; MidCentral; Canterbury
INFORMATION
RELEASED
Designated Auditing Agency: The DAA Group Limited
Types of audit:
Surveillance Audit
Premises audited:
Healthcare of NZ Christchurch; Healthcare of NZ Hamilton; Healthcare of NZ New Plymouth; Healthcare of
NZ Auckland; Healthcare of NZ Tauranga; Healthcare of NZ Palmerston North
OFFICIAL
Dates of audit:
Start date:
18 March 2019
End date:
18 April 2019
Page 1 of 83
Page 1 of 107
Document 1
Home and Community Support Services Audit Report
Home and Community Support ServiceAudit Team
Lead Auditor
Karen Davis
Hours on
72
Hours off
24
site
site
Other Auditors
Joy Hickling
Total hours
72
Total hours
24
on site
off site
Technical Experts
Click here to enter text
Total hours
0
Total hours
0
on site
off site
1982
Consumer Auditors
Click here to enter text
Total hours
0
Total hours
0
on site
off site
THE
Peer Reviewer
Joanna Harper
Hours
3
ACT
Sample Totals
Total audit hours on site
144
Total audit hours off site
51
Total audit hours
195
UNDER
Number of consumers interviewed
41
Number of field based staff
59
Total FTE equivalent staff
0
(face to face)
interviewed
employed
Number of consumers interviewed
8
Number of office based staff
19
Number of managers interviewed
22
(telephone)
interviewed
Number of consumer records
97
Number of staff records reviewed
106
Number of relatives interviewed
5
reviewed
Total number of consumers receiving
41212
Total number of staff employed
3550
Number of health professionals
19
services
interviewed
INFORMATION
RELEASED
OFFICIAL
Page 2 of 83
Page 2 of 107
Document 1
Home and Community Support Services Audit Report
Executive Summary of Audit
General Overview
HealthcareNZ Limited (previously called Healthcare Holding Ltd) provides home and community services throughout New Zealand via
HealthCare of New Zealand Limited (previously known as Healthcare of New Zealand Ltd and Healthcare Rehabilitation Ltd). Community
mental health services have been provided in in five location under the name Mental Health NZ.
Since the last audit, there has been a formal merger of Healthcare New Zealand Ltd and Healthcare Rehabilitation Ltd and renaming of the
1982
organisation. This has resulted in significant change with two out of a three-stage restructuring programme completed. A divisional chief
executive officer has been appointed to HealthCare of New Zealand. The first stages of the restructure included restructuring of the area
THE
manager and national operation roles and the next tier of management. There are now six regional operations managers (ROMs) that are
responsible for all services provided within their geographical location. Six regional clinical managers have been appointed aligned
ACT
geographically with each regional operations manager to assist with clinical governance. New roles have been developed, including national
service development manager, and a service improvement manager role (currently vacant). Thirteen locality managers have been appointed
(previously called branch managers). Clinical service managers or service managers are responsible for services provided to rehabilitation
clients in each location. The title is different between some locations based on size of the service. There are designated service managers for
the mental health services. All of the locality managers of the localities audited were appointed to the role in September 2018 although most
UNDER
held branch manager roles previously with one of the previous service entities. The regional operations managers all held senior management
roles prior to the restructure and have now expanded responsibilities. A new company called ‘My Skills’ is responsible for overseeing the staff
learning and development framework for the three services included in this audit.
This is the first occasion all home and community services have been incorporated into one certification programme for HealthCare New
Zealand. Six localities (Albany, Penrose, Palmerston North, Hamilton, Tauranga and Christchurch) were included in this audit along with the
mental health services provided in Hamilton, Tauranga and Christchurch.
All mental health services now use ‘recordbase’ as the electronic client management system. Work has commenced and is ongoing to merge all
INFORMATION
other community and rehabilitation services to one client management system (Care Call). Along with this, electronic time and attendance
records (replacing timesheets) for staff are being slowly introduced.
RELEASED
Work has been ongoing to standardise and align policies, procedures and quality and risk systems across all the home and community services.
The home and community services provided are funded by Accident Compensation Corporation (ACC), District Health Boards (DHBs), the
Ministry of Health (MOH), Veterans Affairs and by privately paying consumers. In some locations, a restorative model of care is being
implemented where this is contractually required by individual DHBs.
There are 2,073.38 staff employed in the community services, 1, 447.60 staff employed in the rehabilitation services, and 30 recovery facilitators
OFFICIAL
in mental health. All consumers and family members interviewed were satisfied with the services received.
Page 3 of 83
Page 3 of 107
Document 1
Home and Community Support Services Audit Report
During the previous three audits (Mental Health New Zealand in 2016), Healthcare New Zealand (June 2017) and the Healthcare Rehabilitation
verification audit (November 2017), there were 28 areas identified as requiring improvement with some only related to one service. The areas
for improvement raised related to managing client finances, policies and processes related to entering consumers’ homes, monitoring
organisation performance, consulting with mental health consumers and family /whanau, incident management, developing access/entry criteria
for mental health clients along with a sufficiently detailed admission agreement, and exit/discharge processes for mental health clients have
been addressed. One client management system is now used in mental health, ensuring community staff maintain client information in a
confidential manner, monitoring of non-signing clients, the afterhours service/client and staff/client rostering, aspects of medicine management,
developing and implementing a policy for self-administering of medicines by clients, infection control policies and procedures, and staff training
on challenging behaviour have also been addressed.
1982
At this audit, eight areas continue to require improvement. These relate to complaints management, undertaking internal self-
assessments/snapshot audits, corrective action planning, identifying priority clients in an emergency, staff training, staff competency
THE
assessments/performance appraisals, review of clients’ progress towards achieving their goals, and ensuring service plans are reviewed at least
ACT
annually.
Outcome 1: Consumer Rights
Systems and processes are in place to ensure that clients’ rights are maintained. A copy of the Code of Health and Disability Services
UNDER
Consumers’ Rights (the Code), together with information about the Nationwide Health and Disability Advocacy Service is provided to the client on
entry to the service. There are opportunities for discussion if the client so wishes. Education relating to clients’ rights is included in staff
orientation.
The individual preferences, values and beliefs of clients along with specific cultural/spiritual requirements are identified and incorporated into the
service delivery plan. A copy of the plan is provided to the client and is available to guide support workers during service delivery.
Systems and processes are in place to ensure that clients and staff are informed of the complaints process. Clients confirmed any complaints
have been addressed. Policies and procedures are available to guide staff practices related to concerns clients may be at risk of abuse or
INFORMATION
neglect.
Open disclosure principles are followed.
RELEASED
Outcome 2: Organisational Management
The service is governed by a board of directors and is managed by an experienced divisional chief executive with the support of regional
operations managers, regional clinical mangers, and locality/service managers. Processes are in place to monitor the organisation’s progress to
achieving their goals and objectives.
OFFICIAL
The organisation’s quality and risk management system includes quality improvement projects, complaints, compliments, client experience
surveys, identification and monitoring of risk and adverse event reporting. Open disclosure is documented as occurring. Complaints, incident and
Page 4 of 83
Page 4 of 107
Document 1
Home and Community Support Services Audit Report
health and safety data are monitored by locality and service as well as nationally with themes and trends identified and communicated. The
organisation is an accredited employer by Accident Compensation Corporation (ACC) at tertiary level.
Organisation policies and procedures have been reviewed and standardised for the community services. Document control processes are
implemented.
Support workers are aware of the need to maintain any client information in a secure and confidential manner. One client records management
system is now in use in mental health services. Clients and their family/whanau where applicable are consulted about services delivered.
Outcome 3: Human Resources
1982
A comprehensive induction/orientation programme is available for new staff relevant to their roles and responsibilities.
THE
An on-going training programme is in place, including support to complete level two and three of an industry approved qualification. The support
worker competency framework has been reviewed.
ACT
All registered health professionals have current annual practising certificates and access to relevant ongoing education. Support workers and
recovery facilitators have access to advice and support where required both during business hours and afterhours.
Outcome 4: Service Delivery
UNDER
Service agreements include all the requirements of the standard. Service plans are focused on maintaining and supporting independence and
recovery. The service plans for the three service streams are in different formats. Clients and families interviewed expressed their satisfaction
with their involvement in the development of their or their relatives’ service plans and the review process whenever it occurs. They also
expressed their satisfaction with the standard of services provided to them and the reliability of the service.
Staff reported they receive good support from managers, coordinators and RNs. There are systems in place for contingency planning in the
event of an emergency.
INFORMATION
The medicine management policies and procedures have been reviewed and ratified. The services at the branches visited have developed close
links with a range of support agencies including district health boards (DHBs), primary health organisations (PHOs), the Accident Compensation
RELEASED
Corporation (ACC) and veterans’ affairs, to ensure services are coordinated with other service providers working with each client.
OFFICIAL
Page 5 of 83
Page 5 of 107
Document 1
Home and Community Support Services Audit Report
Summary of Attainment
CI
FA
PA Negligible
PA Low
PA Moderate
PA High
PA Critical
Standards
0
15
0
1
4
0
0
Criteria
0
54
0
2
6
0
0
UA Negligible
UA Low
UA Moderate
UA High
UA Critical
Not Applicable
Pending
Not Audited
Standards
0
0
0
0
0
0
0
11
1982
Criteria
0
0
0
0
0
0
0
48
THE
ACT
Corrective Action Requests (CAR) Report
Code
Name
Description
Attainment
Finding
Corrective Action
Timeframe (Days)
HCS.2012
Standard 1.9:
The consumer's right
PA Moderate
Click here to enter
UNDER
Complaints
to make a complaint
text.
is understood,
respected, and
upheld.
HCS.2012
Criterion 1.9.3
An up-to-date
PA Moderate
Where complaints are
Ensure the
90
complaints register is
open more than 20
investigation includes
maintained that
working days,
all aspects of the
documents and
communications with
complaint and the
includes all
the complainant are
complainant is
INFORMATION
complaints, dates,
not consistently
advised of the
and actions taken.
occurring or
outcome. Ensure
RELEASED
documented as
ongoing
occurring.
communications
Communication with
occur with the
the complainant on
complainant in the
the outcome of
event a complaint is
complaints is not
unable to be
always noted or has
addressed within 20
not included all
working days.
OFFICIAL
aspects in the
complaint.
Page 6 of 83
Page 6 of 107
Document 1
Home and Community Support Services Audit Report
Code
Name
Description
Attainment
Finding
Corrective Action
Timeframe (Days)
HCS.2012
Standard 2.3: Quality
Consumers receive
PA Moderate
Click here to enter
and Risk
services that reflect
text.
Management
continuous quality
improvement
principles through the
organisation having
an established,
documented, and
maintained quality
1982
and risk management
system.
THE
HCS.2012
Criterion 2.3.4
A process to measure
PA Low
Some staff
Provide applicable
180
achievement against
undertaking self-
staff with training on
ACT
the quality and risk
assessments have
undertaking self-
management plan is
not been trained in
assessments. Ensure
implemented.
the process and
self-assessments are
follow-up action
undertaken in the
required. There is
required timeframes,
UNDER variation across the results
services / branches in
documented in a
how the results of
consistent manner,
self-assessments are
action plans
documented, the
developed where
frequency they are
applicable and
conducted, the
implemented and
documentation of
monitored for
results, and the
effectiveness.
development and
Analyse staff exit
INFORMATION
follow-up of action
interview data in a
plans in response to
timely manner and
RELEASED
self-assessment
develop an action
findings.
plan to address
There is no
findings.
systematic analysis of
staff exit interview
data and an
organisation wide
plan to address
OFFICIAL
findings has not been
developed.
Page 7 of 83
Page 7 of 107
Document 1
Home and Community Support Services Audit Report
Code
Name
Description
Attainment
Finding
Corrective Action
Timeframe (Days)
HCS.2012
Criterion 2.3.5
The development and
PA Moderate
The corrective actions
Ensure corrective
90
implementation of
taken in response to
action plans are
corrective action
some incidents,
consistently
plans that address
complaints, self-
developed in a timely
areas identified for
assessments and
manner where areas
improvement.
staff exit survey data
for improvement are
are not always
identified, are
documented or
implemented, and
followed up in a timely monitored for
1982
manner. Where
effectiveness. Ensure
advice is sought from
feedback received
THE
the complex issues
from the complex
group or national care
issues group or
and protection team,
national care and
ACT
recommendations
protection team are
received are not
linked to the client’s
always linked to the
record / incident
client record or
management system.
incident management
UNDER system.
HCS.2012
Standard 2.7:
Consumers receive
PA Low
Click here to enter
Essential and
an appropriate and
text.
Emergency Systems
timely response
during emergency
and security
situations.
HCS.2012
Criterion 2.7.2
The organisation, in
PA Low
Mental Health
Expand the list of
90
INFORMATION
consultation with the
Christchurch has a list client addresses and
consumer, identifies
of client addresses
phone numbers to
and implements an
and phone numbers;
include a priority list
RELEASED
appropriate plan
however, a priority list
based on risk for use
relevant to the
based on risk has
in an emergency.
consumer’s needs in
been not been
an emergency.
developed.
HCS.2012
Standard 3.2:
Consumers receive
PA Moderate
Copies of industry
Orientation, Induction,
services from service
approved qualification
Ongoing
providers who are
records / certificates
OFFICIAL
Development, and
trained and assessed
are obtained for the
Competency
staff records where
Page 8 of 83
Page 8 of 107
Document 1
Home and Community Support Services Audit Report
Code
Name
Description
Attainment
Finding
Corrective Action
Timeframe (Days)
as competent to
employees have
provide services.
qualifications at
employment.
HCS.2012
Criterion 3.2.2
A developed,
PA Moderate
Whilst a training plan
Implement a training
90
implemented, and
has been developed
plan relevant to the
recorded training plan
for recovery
service and include
relevant to the service
facilitators working in
topics detailed above.
provider’s scope of
Christchurch, training
1982
practice is
is not consistently
maintained.
being provided.
Records are not
THE
available to
demonstrate that staff
ACT
working in this service
have completed
training on abuse and
neglect, management
of actual or potential
UNDER aggression
/challenging
behaviour training,
and infection
prevention and
control.
HCS.2012
Criterion 3.2.3
There is a system to
PA Moderate
Some support
Ensure staff
90
determine and
workers are overdue
consistently complete
develop the
annual performance
competency
INFORMATION
competencies of the
appraisals in all
requirements and
organisation’s service
locations audited
records are retained.
providers to meet the
except mental health
Undertake annual
RELEASED
needs of consumers.
services and Hamilton performance
This shall be achieved
community services.
appraisals for staff
by, but is not limited
Some support
to:
workers, including
(a) The service
those caring for
provider’s
clients with traumatic
competency is
brain injuries, spinal
OFFICIAL
assessed against the
cord injuries are
organisation’s policies
overdue annual
and procedures;
competency review in
Page 9 of 83
Page 9 of 107
Document 1
Home and Community Support Services Audit Report
Code
Name
Description
Attainment
Finding
Corrective Action
Timeframe (Days)
(b) Competency gaps
all locations audited
between consumer’s
except Hamilton
needs and service
community services.
provider’s
competency are
identified;
(c) Specialist advice,
training, information,
and oversight are
1982
provided by
individuals who are
THE
trained/qualified and
competent to
undertake this role.
ACT
HCS.2012
Standard 4.11:
Consumers are
PA Moderate
Click here to enter
Review of Service
supported to achieve
text.
Delivery
their goals through
regular monitoring
UNDER
and review of service
delivery.
HCS.2012
Criterion 4.11.2
Reviews are
PA Moderate
Although progress
Ensure service plan
180
documented,
has been made,
reviews are
consumer focused,
reviews of goals in the documented, client
indicate the degree of
rehabilitation and
focused and indicate
achievement or
community services
the progress towards
response to the
do not consistently
meeting the client’s
support and progress
indicate the progress
goals.
INFORMATION
towards meeting the
towards meeting the
consumer’s goals.
client’s goals.
RELEASED
HCS.2012
Criterion 4.11.4
There is formal
PA Moderate
Apart from the mental
Complete overdue
180
evidence of a review
health service, not all
reviews in the
occurring in line with
reviews meet the
rehabilitation and the
the organisation’s
required timeframes
community services.
policy.
in the rehabilitation
and community
services.
OFFICIAL
Page 10 of 83
Page 10 of 107
Document 1
Home and Community Support Services Audit Report
Recommendations Report
Code
Name
Description
Attainment
Recommendation
HCS.2012 Standard 2.1:
Consumers receive services that
FA
Organisation meeting minute templates be made available to managers and their use
Governance
are planned, co-ordinated, and
encouraged.
appropriate to their needs.
HCS.2012 Standard 3.2:
Consumers receive services
PA Moderate
Copies of industry approved qualification records / certificates are obtained for the
Orientation,
from service providers who are
staff records where employees have qualifications at employment.
Induction,
trained and assessed as
1982
Ongoing
competent to provide services.
Development,
THE
and Competency
ACT
Continuous Improvement (CI) Report
Code
Name
Description
Attainment
Finding
UNDER
INFORMATION
RELEASED
OFFICIAL
Page 11 of 83
Page 11 of 107
Document 1
Home and Community Support Services Audit Report
NZS 8158:2012: Home and Community Support Sector Standards
Outcome 1: Consumer Rights
Every consumer’s values, dignity, and culture are recognised and supported; their choices respected; and their rights upheld.
Standard 1.1: Consumer Rights Under Legislation
(HCS.2012:1.1)
Consumers receive services in accordance with their rights.
1982
Attainment and Risk: FA
THE
Evidence: The organisation has a client code of rights policy that meets the requirements of the standard and guides staff practice.
ACT
The Health and Disability Commissioner's (HDC) Code of Health and Disability Services Clients’ Rights (the Code), the Code of ACC Claimant Rights together with
information about the HDC Advocacy Service information are required to be given to each client in the three services by way of each individual’s service guide and agreement
booklet for ACC clients and service agreements for rehabilitation and mental health services. The allocated service coordinators, recovery facilitators, service managers
and/or registered health professionals provide this information at the time of the first face-to-face meeting and outline the client’s rights and responsibilities. There is
opportunity for further discussion/clarification during this time and at any time following. Clients are informed of their right to have a support person/advocate present during
UNDER
all contacts and should they wish to make a complaint.
As required by the organisational informed consent policy, signed consents were sighted in the client's individual files reviewed. Any additional consents are recorded in files
as required.
Training in the Codes and Advocacy Services occurs at orientation and on an ongoing basis for support workers and recovery facilitators. Support workers and recovery
facilitators demonstrated a sound understanding of the Code and how this is used to guide their day-to-day work.
Clients interviewed across the service streams were complementary of the way services are delivered, stated that their rights are respected and they are fully informed and
involved in all decisions relating to their service delivery.
INFORMATION
Recommendation:
Click here to enter text.
RELEASED
Criterion 1.1.1 (HCS.2012:1.1.1)
Service providers demonstrate knowledge and understanding of consumer rights and obligations, and incorporate them as part of their everyday practice.
Attainment and Risk: FA
OFFICIAL
Evidence:
Click here to enter text.
Page 12 of 83
Page 12 of 107
Document 1
Home and Community Support Services Audit Report
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Criterion 1.1.2 (HCS.2012:1.1.2)
1982
Information about the Code and other rights is provided at the earliest opportunity in languages and formats suited to the needs of consumers who are using the service.
Attainment and Risk: FA
THE
Evidence:
ACT
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
UNDER
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Criterion 1.1.3 (HCS.2012:1.1.3)
There are opportunities for discussion, explanation, and clarification of the information with service providers.
Attainment and Risk: FA
INFORMATION
Evidence:
Click here to enter text.
RELEASED
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
OFFICIAL
Page 13 of 83
Page 13 of 107
Document 1
Home and Community Support Services Audit Report
Criterion 1.1.4 (HCS.2012:1.1.4)
Consumers are informed of the availability of advocates, particularly in the event a complaint is made.
Attainment and Risk: FA
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
1982
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
THE
ACT
Criterion 1.1.5 (HCS.2012:1.1.5)
Consumers have the right to have an advocate/support person present.
Attainment and Risk: FA
UNDER
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
INFORMATION
RELEASED
Criterion 1.1.6 (HCS.2012:1.1.6)
Consumers have the right to make an informed choice and give informed consent to actively participate in decision making and in support service delivery.
Attainment and Risk: FA
Evidence:
Click here to enter text.
OFFICIAL
Finding:
Click here to enter text.
Page 14 of 83
Page 14 of 107
Document 1
Home and Community Support Services Audit Report
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Criterion 1.1.7 (HCS.2012:1.1.7)
The service provider is able to demonstrate that consent is obtained where required in accordance with the Code.
Attainment and Risk: FA
1982
Evidence:
Click here to enter text.
THE
Finding:
ACT
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
UNDER
Standard 1.2: Individual Privacy, Dignity and Respect
(HCS.2012:1.2)
Consumers are treated with respect and receive services in a manner that has regard for their dignity, privacy, confidentiality, and independence.
Attainment and Risk: Not Audited
Evidence: Click here to enter text.
INFORMATION
Recommendation:
Click here to enter text.
RELEASED
Criterion 1.2.1 (HCS.2012:1.2.1)
Services are provided in a way that maintains and respects privacy, dignity, and the consumer’s independence.
OFFICIAL
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
Page 15 of 83
Page 15 of 107
Document 1
Home and Community Support Services Audit Report
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Criterion 1.2.2 (HCS.2012:1.2.2)
1982
Consumers' information is maintained in a confidential manner.
Attainment and Risk: Not Audited
THE
Evidence:
ACT
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
UNDER
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Standard 1.3: Individual Values and Beliefs Respected
(HCS.2012:1.3)
Consumers receive culturally safe services which recognise and respect their ethnic, cultural, and spiritual values and beliefs.
Attainment and Risk: Not Audited
INFORMATION
Evidence: Click here to enter text.
RELEASED
Recommendation:
Click here to enter text.
OFFICIAL
Page 16 of 83
Page 16 of 107
Document 1
Home and Community Support Services Audit Report
Criterion 1.3.1 (HCS.2012:1.3.1)
Consumers receive services in a manner that takes into account their individual cultural values and beliefs.
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
1982
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
THE
ACT
Criterion 1.3.2 (HCS.2012:1.3.2)
The consumer is consulted on individual values and beliefs. Family/whānau of choice or other representatives are involved at the consumer’s request.
Attainment and Risk: Not Audited
UNDER
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
INFORMATION
RELEASED
Standard 1.4: Recognition of Maori Values and Beliefs
(HCS.2012:1.4)
Māori consumers have their health and disability needs met in a manner that respects and acknowledges their individual and cultural values and beliefs.
Attainment and Risk: Not Audited
Evidence: Click here to enter text.
OFFICIAL
Recommendation:
Click here to enter text.
Page 17 of 83
Page 17 of 107
Document 1
Home and Community Support Services Audit Report
Criterion 1.4.1 (HCS.2012:1.4.1)
Service providers understand and respect the key principles outlined in relevant health and disability strategy documents, and demonstrate a commitment to these principles
in the provision of services.
Attainment and Risk: Not Audited
Evidence:
1982
Click here to enter text.
Finding:
THE
Click here to enter text.
Corrective Action:
ACT
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
UNDER
Criterion 1.4.2 (HCS.2012:1.4.2)
Māori consumers have access to appropriate services. Barriers to access within the control of the service provider are identified and eliminated.
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
INFORMATION
Corrective Action:
RELEASED
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
OFFICIAL
Page 18 of 83
Page 18 of 107
Document 1
Home and Community Support Services Audit Report
Criterion 1.4.3 (HCS.2012:1.4.3)
Māori consumers receive services consistent with their cultural values and beliefs.
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
1982
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
THE
ACT
Criterion 1.4.4 (HCS.2012:1.4.4)
The right of Māori consumers to practice their cultural values and beliefs while receiving services is acknowledged and facilitated by service providers.
Attainment and Risk: Not Audited
UNDER
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
INFORMATION
RELEASED
Criterion 1.4.5 (HCS.2012:1.4.5)
The importance of whānau and their involvement with Māori consumers is recognised and supported by service providers.
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
OFFICIAL
Finding:
Click here to enter text.
Page 19 of 83
Page 19 of 107
Document 1
Home and Community Support Services Audit Report
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Standard 1.5: Recognition of Pacific People’s Values and Beliefs
(HCS.2012:1.5)
Pacific consumers have their health and disability needs met in a manner that respects and acknowledges their individual and cultural values and beliefs.
1982
Attainment and Risk: Not Audited
Evidence:
THE
Click here to enter text.
Recommendation:
ACT
Click here to enter text.
Criterion 1.5.1 (HCS.2012:1.5.1)
UNDER
Service providers understand and respect the key principles outlined in relevant health and disability strategy documents, and demonstrate a commitment to these principles
in the provision of services.
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
INFORMATION
Corrective Action:
RELEASED
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
OFFICIAL
Page 20 of 83
Page 20 of 107
Document 1
Home and Community Support Services Audit Report
Criterion 1.5.2 (HCS.2012:1.5.2)
Services for Pacific peoples recognise the dignity and the sacredness of life are integral in the delivery of services.
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
1982
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
THE
ACT
Criterion 1.5.3 (HCS.2012:1.5.3)
Pacific people receive services that are co-ordinated and culturally competent.
Attainment and Risk: Not Audited
UNDER
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
INFORMATION
RELEASED
Criterion 1.5.4 (HCS.2012:1.5.4)
The service provider facilitates access to a Pacific recognised/accredited trained advocate and interpreter to advocate on cultural issues on behalf of Pacific people receiving
care and support.
Attainment and Risk: Not Audited
Evidence:
OFFICIAL
Click here to enter text.
Finding:
Click here to enter text.
Page 21 of 83
Page 21 of 107
Document 1
Home and Community Support Services Audit Report
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Standard 1.6: Communication in a Manner that the Consumer can Understand
(HCS.2012:1.6)
Information is communicated to consumers in a manner that the consumer can understand.
1982
Attainment and Risk: Not Audited
Evidence:
THE
Click here to enter text.
Recommendation:
ACT
Click here to enter text.
Criterion 1.6.1 (HCS.2012:1.6.1)
UNDER
Consumers have a right to full and frank information and open disclosure.
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
INFORMATION
Corrective Action:
Click here to enter text.
RELEASED
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Criterion 1.6.2 (HCS.2012:1.6.2)
Service providers allow sufficient time for discussions to take place.
OFFICIAL
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
Page 22 of 83
Page 22 of 107
Document 1
Home and Community Support Services Audit Report
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Criterion 1.6.3 (HCS.2012:1.6.3)
1982
Service providers identify themselves to consumers when visiting their home.
Attainment and Risk: Not Audited
THE
Evidence:
ACT
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
UNDER
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Criterion 1.6.4 (HCS.2012:1.6.4)
Wherever necessary and reasonably practicable, interpreter services (including a New Zealand Sign Language interpreter) are provided.
Attainment and Risk: Not Audited
INFORMATION
Evidence:
Click here to enter text.
RELEASED
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
OFFICIAL
Page 23 of 83
Page 23 of 107
Document 1
Home and Community Support Services Audit Report
Standard 1.7: Freedom from Abuse or Neglect
(HCS.2012:1.7)
Consumers are free from any discrimination, coercion, harassment, sexual, financial, or other exploitation, abuse (physical, psychological, sexual, or financial), or neglect.
Attainment and Risk: FA
Evidence: Policies and procedures that include all elements required by this standard are provided to guide staff, including signs and indicators of abuse and neglect. These documents
have been recently updated. A new policy has been developed ‘vulnerable children and child protection policy’ and a care and protection team established to provide advice
and support within the organisation where applicable. All incidents of discrimination, abuse or neglect, either suspected or observed, are required to be reported. Training on
this topic is included in the orientation programme for new support workers, recovery facilitators, office-based staff, and managers with one exception (refer to the area for
improvement raised in 3.2.2). This topic is also included in the ongoing education programme for staff who are working towards an industry-approved qualification. Staff are
1982
required to report any concerns about a client at risk of abuse of neglect to either the service manager, the coordinator, the registered health professional or the locality / line
manager, and applicable events are also reported via the incident management system. The support workers and recovery facilitators interviewed demonstrated a good
THE
understanding of their responsibilities. Where staff had reported concerns to their line manager these concerns had been investigated and followed up in a timely manner, as
observed during audit. Communication with the funder and other applicable external agencies has also occurred when appropriate.
ACT
Support workers and recovery facilitators interviewed demonstrated a sound understanding of professional boundaries. These are discussed during orientation and the Code
of Conduct given to staff to review and sign as a component of the employment process. Suspected or identified breaches in maintaining professional boundaries are reported
via the incident management system and followed up by the applicable manager.
Team meetings are held at various frequencies in the homes of rehabilitation clients with complex care needs. The discussions include any areas of concern or client / family
safety.
UNDER
The information provided to new clients includes information on the professional conduct required of support workers. All clients interviewed reported being satisfied with their
support workers or recovery facilitators and confirmed they have not experienced any sort of abuse or neglect from staff.
Recommendation:
Click here to enter text.
INFORMATION
Criterion 1.7.1 (HCS.2012:1.7.1)
There are policies and procedures to ensure consumers are not subjected to discrimination, coercion, harassment, sexual, financial, or other exploitation, abuse (physical,
RELEASED
psychological, sexual, or financial), or neglect.
Attainment and Risk: FA
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
OFFICIAL
Corrective Action:
Click here to enter text.
Page 24 of 83
Page 24 of 107
Document 1
Home and Community Support Services Audit Report
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Criterion 1.7.2 (HCS.2012:1.7.2)
Service providers maintain professional boundaries and refrain from acts or behaviour which could benefit the service provider or organisation at the expense or well-being of
the consumer.
Attainment and Risk: FA
Evidence:
1982
Click here to enter text.
Finding:
THE
Click here to enter text.
ACT
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
UNDER
Criterion 1.7.3 (HCS.2012:1.7.3)
All al egations of discrimination, abuse, or neglect of any kind are managed and recorded according to the organisation’s policies and procedures, and link to the quality and
risk management system.
Attainment and Risk: FA
Evidence:
Click here to enter text.
INFORMATION
Finding:
Click here to enter text.
RELEASED
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
OFFICIAL
Page 25 of 83
Page 25 of 107
Document 1
Home and Community Support Services Audit Report
Criterion 1.7.4 (HCS.2012:1.7.4)
A process is established to record and report incidents of discrimination, abuse, or neglect.
Attainment and Risk: FA
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
1982
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
THE
ACT
Criterion 1.7.5 (HCS.2012:1.7.5)
Abuse and neglect prevention awareness is included in the induction programme for all service providers and is updated regularly to maintain knowledge.
Attainment and Risk: FA
UNDER
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
INFORMATION
RELEASED
Standard 1.8: Consumers' Belongings, Property, and Finances are Respected and Protected
(HCS.2012:1.8)
Consumers’ belongings, property, and finances are respected at al times.
Attainment and Risk: FA
Evidence: Policies and procedures protect the client’s money, belongings and property during service delivery, including entering the homes of clients.
OFFICIAL
Service coordinators stated in the branches visited that all clients on the high-risk registers have been reviewed and the numbers of clients remaining on the registers has
decreased significantly. Review of the electronically held high-risk registers confirmed this. Support workers reported they are not involved in money matters with clients if
possible. Clients who require shopping either go on an outing with the support worker to undertake the shopping directly with assistance if required. Some clients order
Page 26 of 83
Page 26 of 107
Document 1
Home and Community Support Services Audit Report
groceries from supermarkets or buy food boxes online and pay for the items online directly with the supplier. Support workers can collect the items if required on behalf of the
client or the items can be delivered to the client’s home. Clients’ families/EPOA are also encouraged to support the client with shopping, especially for larger items.
If shopping is required to be undertaken by a support worker, a specific form is utilised to document each transaction including the cash given, receipt total and change given
and that the totals align. Entries are signed by the client / nominated representative and the support worker. Organisation policy requires that the specific arrangements and
monitoring process must be clearly documented in the support plan. All service/support plans reviewed evidenced the specific arrangements and monitoring. Senior service
coordinators/managers are responsible overall for monitoring the high-risk registers and any changes to a client’s situation is discussed fully with the client and other staff and
the register updated.
Staff, if required, are provided with information on how to enter a client’s home. This includes knowledge of the location of a hidden key or knowing the pin number of a lock
box or medicine storage box. On rare occasions, a support worker may have a key to the client’s home. In this situation, information is documented in the client’s electronic
file and on the high-risk register.
1982
Support workers demonstrated they know of the requirements set out in policy and stated they always knock and wait for a response before entering a client’s home. The
stated exceptions include when the client is known to require staff assistance to get out of bed and another family member may not be present. In this event, the support
THE
workers note they will knock and enter and call out to the client that they have arrived. The support workers stated this is only undertaken at the request of the client / family
and with the prior knowledge of the specific service coordinator. Policies and procedures protect the client’s money, belongings and property during service delivery, including
ACT
entering the homes of clients.
New clients are provided with information on policies and the process around management of money (if applicable), access to their home and protection of property during
their initial contact with the service. Clients reported that support/care workers carry out procedures as described. The finding from the verification audit in 2017 has been
addressed and is now closed.
UNDER
‘Access to a Person’s Home’ policy is a mental health service policy and provides guidance for staff accessing a client’s home which is agreed to by the client. The policy also
includes whether the client has any preferences, for example removing shoes before entering the client’s home. This information is documented in the client’s personal file.
Hazards are identified in a hazard assessment checklist. Review of clients’ files and hazard checklists confirmed this. The service managers reported recovery facilitators do
not hold keys to clients’ homes who are using mental health services, as it is not considered appropriate.
Recovery facilitators demonstrated they are knowledgeable with regards to knowing what the procedure is for ensuring the safety of clients and/or staff. The service manager
for the Hamilton and Tauranga branches reported two staff always attend the first home visit and includes either a recovery facilitator or the service manager and a clinical key
worker from the DHB mental health team. In the Christchurch branch, the service manager and a recovery facilitator undertake the initial visit.
The finding from the mental health certification audit in 2016 and the verification audit in November 2017 have been addressed and are now closed.
INFORMATION
Recommendation:
Click here to enter text.
RELEASED
Criterion 1.8.1 (HCS.2012:1.8.1)
There are policies and procedures for the protection of consumers’ money and property during service delivery.
Attainment and Risk: FA
OFFICIAL
Evidence:
Click here to enter text.
Page 27 of 83
Page 27 of 107
Document 1
Home and Community Support Services Audit Report
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Criterion 1.8.2 (HCS.2012:1.8.2)
1982
There are clear policies about entering the homes of consumers.
Attainment and Risk: FA
THE
Evidence:
ACT
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
UNDER
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Standard 1.9: Complaints
(HCS.2012:1.9)
The consumer's right to make a complaint is understood, respected, and upheld.
Attainment and Risk: PA Moderate
INFORMATION
Evidence: The policy and procedure for complaints includes definitions of complaints and describes how complaints are to be reported and includes the process and timeframes for
RELEASED
managing and responding to a complaint. The documents meet the requirements of this standard and Right 10 of the Code. The service managers, and the locality
managers, are responsible for the overall management of complaints, with the assistance of the coordinators and registered health professionals as applicable / required.
Complaints are required to be reported electronically. This is via Promapp for all community clients excluding the mental health services where complaints are recorded on
‘Recordbase’, (the mental health client management programme). Complaints are also to be referenced within the client’s individual file. Promapp and Recordbase are utilised
as the complaints registers.
Progress updates were not consistently evident for complaints open more than 20 working days. Some complaints did not have sufficiently detailed investigation and
responses. This was raised as an area for improvement in the 2017 certification audit and continues to be an area requiring improvement. There are escalation processes to
OFFICIAL
ensure applicable local, regional and national managers are advised of significant complaints. There have been three complaints received via the Health and Disability
Commissioner since January 2018 in the branches audited. A complaint was received in Christchurch in February 2019 and is currently being investigated. Two other
Page 28 of 83
Page 28 of 107
Document 1
Home and Community Support Services Audit Report
complaints received related to services provided in Palmerston North (March 2018) and in Penrose (February 2018), were not formally investigated and referred to the HDC
advocate for resolution. Both complaints were resolved to the complainant’s satisfaction via the advocacy process.
Regular reports are issued from the quality and risk team at national office summarising complaints and the themes and trends over time to the quality safety and clinical
governance and individually to each region and service type (community, rehabilitation and mental health).
The information pack for all new clients includes information on the complaints process. Clients interviewed reported they knew how to make a complaint if needed, and any
concerns raised had been followed up.
Recommendation:
Click here to enter text.
1982
THE
Criterion 1.9.1 (HCS.2012:1.9.1)
ACT
An easily accessed, responsive, and fair complaints process, which complies with Right 10 of the Health and Disability Commissioner’s Code of Health and Disability Services
Consumers’ Rights is documented and implemented. This shall include, but is not limited to:
(a) The service operates the complaints process in a fair and appropriate manner, including the involvement of advocacy services, where appropriate;
(b) The organisation encourages consumers to use the complaints process when they have a complaint about service providers;
(c) Service providers attend training on how to receive and manage complaints;
(d) Clearly written guidelines for service providers on what constitutes feedback or complaint;
UNDER
(e) A link to the quality and risk management system.
Attainment and Risk: FA
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
INFORMATION
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
RELEASED
OFFICIAL
Page 29 of 83
Page 29 of 107
Document 1
Home and Community Support Services Audit Report
Criterion 1.9.2 (HCS.2012:1.9.2)
Information about a consumer’s right to complain and the complaints process is available to consumers prior to service commencement, and they are supported in their right
to use the complaints process.
Attainment and Risk: FA
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
1982
Corrective Action:
Click here to enter text.
THE
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
ACT
Criterion 1.9.3 (HCS.2012:1.9.3)
An up-to-date complaints register is maintained that documents and includes all complaints, dates, and actions taken.
UNDER
Attainment and Risk: PA Moderate
Evidence:
The complaints management processes were reviewed in each branch audited and included community health, rehabilitation and mental health services (where applicable).
Some complaints have been managed very well with clear communication occurring with the complainant and all issues being investigated and responded to in a timely
manner. The rehabilitation service in Tauranga managed the sampled complaints well. However, complaints are not always being responded to in timeframes that align with
the Code. Examples were sighted in Penrose, Palmerston North, Hamilton and Tauranga of complaints that have been or are open for more than 20 working days.
Communications with the complainant about additional time required to complete investigations and respond to the complaint are not documented as occurring, although
some managers advise verbal communications had occurred, but conversations have not been documented.
The Tauranga locality manager has undertaken an internal audit of the investigation and response to all complaints received in 2018 and developed an action plan in
INFORMATION
response to findings. Three localities managers advised they are now utilising the services complaints management tool kit to assist in ensuring a more robust complaints
management process.
RELEASED
An adverse events manager was appointed in January 2019 on a 12 month contact for Albany and Penrose offices to assist the applicable staff and managers in investigating
and responding to incidents and complaints in a timely manner.
Four complaints sampled in Hamilton and one in Albany did not have all aspects of the complaint investigated or the response / outcome clearly communicated to the
complainant. (refer to 2.3.5)
Finding:
Where complaints are open more than 20 working days, communications with the complainant are not consistently occurring or documented as occurring.
OFFICIAL
Communication with the complainant on the outcome of complaints is not always noted or has not included all aspects in the complaint.
Page 30 of 83
Page 30 of 107
Document 1
Home and Community Support Services Audit Report
Corrective Action:
Ensure the investigation includes all aspects of the complaint and the complainant is advised of the outcome. Ensure ongoing communications occur with the complainant in
the event a complaint is unable to be addressed within 20 working days.
Timeframe (days): 90
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Outcome 2: Organisational Management
1982
Consumers receive services that comply with legislation and are managed in a safe, efficient, and effective manner.
Standard 2.1: Governance
(HCS.2012:2.1)
THE
Consumers receive services that are planned, co-ordinated, and appropriate to their needs.
ACT
Attainment and Risk: FA
Evidence: The service is governed by a board of directors who monitor the organisation’s performance. The HealthCare of NZ divisional chief executive reports on a regular basis to the
HealthcareNZ Limited chief executive.
UNDER
A sample of service manager, locality manager, clinical services manager and regional operations manager monthly reports reviewed, as well as other documentation showed
information to monitor performance is regularly reported on topics including financial performance, legislative changes/compliance, business development, emerging risks,
human resources/staff training and operational/business issues, quality, client care needs as part of meeting the organisation’s national business/strategic plan (2017-2019).
The organisational chart describes the existing structure and relevant reporting lines. Regular meetings are held by locality managers and regional operations managers with
direct reports. The shortfall from the 2017 verification audit has been addressed. There is variation in the content/format of minutes in some locations as the managers were
unaware of meeting minute templates that are available.
Recommendation:
Organisation meeting minute templates be made available to managers and their use encouraged.
INFORMATION
RELEASED
Criterion 2.1.1 (HCS.2012:2.1.1)
The structure, purpose, values, scope, direction, and goals of the organisation are clearly identified and reviewed.
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
OFFICIAL
Finding:
Click here to enter text.
Page 31 of 83
Page 31 of 107
Document 1
Home and Community Support Services Audit Report
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Criterion 2.1.2 (HCS.2012:2.1.2)
The governing body shall ensure the organisational performance is aligned with and regularly monitored against the identified strategic direction and goals.
Attainment and Risk: FA
1982
Evidence:
Click here to enter text.
THE
Finding:
ACT
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
UNDER
Criterion 2.1.3 (HCS.2012:2.1.3)
The governing body has processes which ensure quality improvement at all levels within the organisation.
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
INFORMATION
Finding:
Click here to enter text.
RELEASED
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
OFFICIAL
Page 32 of 83
Page 32 of 107
Document 1
Home and Community Support Services Audit Report
Standard 2.2: Service Management
(HCS.2012:2.2)
Consumers receive timely, appropriate, and safe services through efficient and effective service management.
Attainment and Risk: FA
Evidence: The locality managers, the regional operations managers (ROMs), the service manager’s for mental health, and clinical services manager or service manager for rehabilitation
services in the six locations audited were interviewed. The ROMs were all appointed to this new role in October 2018, however all held similar type roles for four or more
years prior to the restructuring. All the locality managers were appointed to the role in September 2018. Five of the locality managers were in similar level positions for at least
one year, with one of the locality managers having worked for this organisation in various roles for 12 years. The locality manager in Albany was acting branch manager for
one month prior to her permanent appointment. Staff in clinical services manager / service manager roles in rehabilitation were in similar roles prior to the restructure except
1982
for Hamilton where the rehabilitation clinical services manager was appointed in January 2019. The service manager for mental health services has been in the role since
September 2016 in Hamilton / BOP and for over 36 months in Christchurch.
THE
Role descriptions detail the roles and responsibilities for each position. The managers have relevant experience in managerial or service delivery roles (including as service
coordinators), as verified during interview and / or review of the managers' curriculum vitaes. The managers are required to complete monthly reports for their line manager.
ACT
Examples of these were sighted and included discussion on staffing / human resources issues, contracts legislative changes, client volumes and changes, quality and risk
issues and service delivery. The regional operations managers’ report to the HealthCare New Zealand divisional chief executive. All managers including the division chief
executive interviewed are satisfied that relevant issues that potentially impact on service delivery or related to changing risk are communicated to them in a timely manner.
Clients and family members can provide feedback on services. This includes via the client experience survey process or during regular service delivery reviews. The service
aims to phone new clients three weeks after commencing services for feedback. Rehabilitation clients are also contacted for feedback after a new staff member has provided
UNDER
services. Further communication with clients occurs at three months (mental health services Hamilton), or where otherwise contractually required, and six months after the
client enters the service. The clients / next of kin offered the opportunity to provide feedback on services at these times. This process is repeated during the service review
meetings which are required at least annually although some are overdue (refer to CAR at 4.11.4).
Clients are able to contact office-based staff, or afterhours staff and make requests, or express concerns / complaints or to discuss any aspect of the services being provided
at any time. The clients' files reviewed during audit in all branches demonstrated active ongoing communication is occurring with clients and applicable family members. Such
communication is being recorded into the electronic records.
An annual client experience survey is conducted of mental health clients. The feedback sighted (dated October 2018) was very positive about services. An annual client
experience survey (census) is also conducted of rehabilitation clients. The report was dated June 2018. For the other community clients, the client experience survey is an
INFORMATION
ongoing process with clients in each branch selected fortnightly for inclusion. However, since September 2018 until early April 2019, with the changes made to Care Call, a
new extract process has had to be developed and information has been able to be collated during this time. The results of the client experience surveys are reported via a
RELEASED
heat map process which enables the branch/service to clearly identify what their strengths are as well as opportunities for improvement, and to compare their results with that
of other branches and the organisation overall.
Focus groups have been held in 2018 in Hamilton, Whakatane and Alexandra for clients over aged 65 years and (their family members) that are receiving services. The focus
group outcomes informed the changes made to service provision across the organisation for clients aged over 65 years of age. The national quality manager advised the
intention is to work with rehabilitation clients in 2019 to identify appropriate service outcome measures. At the 2016 mental health certification audit an area for improvement
was raised for mental health services as terms of reference had been developed for the client advisory group, however no meetings held. The service has determined these
meetings will not occur as there are other opportunities for clients to provide feedback on the services received including via their recovery facilitator, communication with the
service managers, the client experience survey and other reviews, and these opportunities are more frequent. This meets the requirements of the standards.
OFFICIAL
Recommendation:
Click here to enter text.
Page 33 of 83
Page 33 of 107
Document 1
Home and Community Support Services Audit Report
Criterion 2.2.1 (HCS.2012:2.2.1)
The service is managed by a suitably qualified and experienced person with authority, accountability, and responsibility for the provision of services.
Attainment and Risk: FA
Evidence:
Click here to enter text.
1982
Finding:
Click here to enter text.
THE
Corrective Action:
Click here to enter text.
ACT
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
UNDER
Criterion 2.2.2 (HCS.2012:2.2.2)
Consumers are consulted on the management of services in ways that encourage open feedback.
Attainment and Risk: FA
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
INFORMATION
Corrective Action:
Click here to enter text.
RELEASED
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
OFFICIAL
Page 34 of 83
Page 34 of 107
Document 1
Home and Community Support Services Audit Report
Standard 2.3: Quality and Risk Management
(HCS.2012:2.3)
Consumers receive services that reflect continuous quality improvement principles through the organisation having an established, documented, and maintained quality and
risk management system.
Attainment and Risk: PA Moderate
Evidence: The quality and risk programme for HealthCare NZ Ltd (2018-2020) has been developed. The quality plan provides the overarching direction for quality and risk activities. The
Quality, Safety and Clinical Governance Committee, meets four time per annum. The chair of this committee is the CEO of HealthCare NZ who reports to the board. The
quality and risk programme are supported by relevant policies and procedures. The quality and risk programme includes a range of activities including but is not limited to,
complaints, compliments, incident/event reporting, client experience surveys (refer to 2.2), conducting self-assessments (internal audits), quality improvement projects, and
1982
policy and procedure review. Policies and procedures have been reviewed and updated with common policies now being used across the home and community services.
Mental Health have additional service specific policies. The documents sighted were current and have been recently released electronically for office-based staff on
THE
‘Filevision’. The paper copies of the new manuals were delivered prior to the end of this audit. The review dates are monitored nationally by a member of the quality team. The
managers interviewed informed that they are advised of policies under review or being newly developed and have the opportunity to have input, and normally once finalised,
ACT
the managers are advised. The managers have the responsibility of ensuring document control processes are implemented at a local level.
Self-assessments are utilised to review key aspects of service provision. There is variation in how these tools are being used, the training provided to staff and the follow-up of
results. There is also some variation in the corrective action planning processes. The issues raised in the 2017 certification and verification audits continue to be areas
requiring improvement.
HealthcareNZ Limited is an accredited employer by the Accident Compensation Corporation (ACC) at tertiary level. The certificate for the period 1 April 2019 to 31 March
UNDER
2020 was sighted.
Processes are in place to monitor organisation risk. There is a formal area in the managers’ and regional operations managers’ monthly report to summarise any changes in
organisation risk(s). The three regional operations managers (ROMs), and the division chief executive were confident changes in risk were being identified and reported in a
timely manner as managers are expected to escalate issues to their immediate line manager at the time there is actually or potentially a significant change in risk. This
includes risks associated with adverse events or complaints. The risk management profile and the risk register for Mental Health New Zealand was dated February 2019. A
‘dynamic’ risk register was sighted for HealthCare New Zealand. This was dated March 2019. The ROMs report risk is discussed as an agenda item at their regular meetings.
In addition, an organisation wide high-risk register is maintained of clients who have staff involved with high risk activities. This includes having financial transactions
completed as part of services, or staff having the knowledge of how to get into the client’s home.
INFORMATION
A quality improvement committee meets in the Christchurch office. This group is discussing quality and risk, health and safety, and human resources issues, and feedback
from support workers and recovery facilitators relevant to mental health, community and rehabilitation services. In this and other branches audited quality and risk topics are
RELEASED
also discussed in office based staff meetings, as well as support worker or recovery facilitator meetings when these occur.
A staff engagement survey was conducted in 2018. The results have been provided to managers, who advise they are reviewing the findings relevant to their area. Action
plans have been developed by the two ROMs where this was discussed. Challenges with technology systems has been identified as an issue, and work is ongoing related to
this issue.
A ‘complex issues’ group meets regularly in Waikato/BOP region to ensure that clients with complex care needs, and the staff involved with providing their care, are well
supported and appropriately trained. A new complex issues group has been recently established in the lower South Island. There are 14 documented objectives for the group
in the terms of reference. ‘The purpose of this committee is to support and advise managers and their teams (the service) in situations where risks to clients, staff and others
OFFICIAL
have been identified. The multidisciplinary team will foster a collaborative approach to addressing issues to improve the quality and safety of services to clients’. Staff and
managers advise this has been an excellent forum to obtain access to additional resources / expertise and training and to have multidisciplinary input into support plans for
the more complex or at-risk clients.
Page 35 of 83
Page 35 of 107
Document 1
Home and Community Support Services Audit Report
A number of quality improvement projects have been undertaken. These have included the mental health services Hamilton, developing a male mentoring / support
programme, building stronger relationships with local kaumatua, and a recovery facilitator and her dog ‘Lucy’ who has been trained and is now an approved mental health
therapy dog. The clinical quality team have introduced a ‘STOPandWATCH’ programme that provides a formal framework detailing the type of client events and possible
symptoms / changes that should be reported to the coordinator, registered health professional or other designated staff member. Care and protection policies have been
implemented and the medicine policy and staff competency framework reviewed and updated. The Palmerston North branch has an action plan in place aimed towards
becoming a ’dementia friendly’ service.
A number of quality / health and safety reports are provided nationally. Aspects monitored include client incident / accident and complaints data (including the number, risk
rating, themes and trends), staff injuries per month, severity of injury, time lost, mechanism of injury and themes and trends.
Correction action planning is occurring although where areas for improvement are required, corrective action plans are not consistently developed and implemented. The
shortfall from the 2017 verification audit continues to be an area requiring improvement.
1982
Nationally two senior quality improvement advisers and two quality improvement advisors have been appointed based in Wellington. They are assisting with review of and
implementing quality improvement projects including analysis of incidents and complaints, analysis of client’s experience survey data, undertaking a review of the incident
THE
reporting systems across the organisation and have made recommendations on how processes can be improved. The quality team are assisting with some process mapping
including the management of referrals. The team have developed the terms of reference for a client and staff safety committee (CASS) meeting. The terms of references have
ACT
been developed but not yet ratified. The draft purpose is ‘to provide evidence-based and timely advice to the Quality Safety and Clinical Governance (QSCG) and Healthcare
NZ divisions to address identified quality and safety issues - and, as a result, to continuously improve the quality strategy and resources nationally’. The quality improvement
team have summarised some of the improvements in the quality reflections 2018 document that was provided. The quality improvement team are also working with clinical
staff on pressure injury prevention.
Recommendation:
UNDER
Click here to enter text.
Criterion 2.3.1 (HCS.2012:2.3.1)
Development and implementation of organisational policies and procedures that are aligned with current good practice and service delivery, meet the requirements of
legislation, and are reviewed at regular intervals as defined by the organisational policy.
INFORMATION
Attainment and Risk: FA
Evidence:
RELEASED
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
OFFICIAL
Page 36 of 83
Page 36 of 107
Document 1
Home and Community Support Services Audit Report
Criterion 2.3.2 (HCS.2012:2.3.2)
The development and implementation of a quality and risk management system.
Attainment and Risk: FA
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
1982
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
THE
ACT
Criterion 2.3.3 (HCS.2012:2.3.3)
The collection, analysis, and evaluation of quality improvement data is implemented and communicated to service providers and, where appropriate, consumers.
Attainment and Risk: FA
UNDER
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
INFORMATION
RELEASED
Criterion 2.3.4 (HCS.2012:2.3.4)
A process to measure achievement against the quality and risk management plan is implemented.
Attainment and Risk: PA Low
Evidence:
Self-assessments are utilised to review the content of client documentation, timeliness and/or completeness of records present in both clients' files and staff personnel files
OFFICIAL
and other aspects including (but not limited to) incident and complaints management, non-signing clients, and staff competency. An annual self-assessment programme has
been developed detailing the aspects required each month over the year (July to June). However, there is variation in the frequency that these are occurring, who is
undertaking these ‘snapshots’ or self-assessments and what happens with the information over time. A new manager interviewed (employed January 2019) was unaware of
Page 37 of 83
Page 37 of 107
Document 1
Home and Community Support Services Audit Report
these tools and the schedule. The results of snapshot audits undertaken prior to her employment could not be located during audit. The service manager mental health had
only recently started to undertake these in Hamilton and Tauranga. In Hamilton, the recovery facilitators were evaluating the documentation of peers. In Tauranga the
recovery facilitators were conducting self-assessments. The service manager of mental health services in Christchurch advised self-assessments have not been conducted
for at least 18 months and was unaware of the self-assessment programme ‘until a couple of weeks ago’. An action plan in response to the client experience survey mental
health services Christchurch has not been documented (refer to 4.11). Some self-assessment templates in use note that staff are to tick if the required component has been
included. There is inadequate guidance on how to record if the aspect is not applicable or not attained / incomplete. In Hamilton community services, there were five different
ways that staff were recording the results where non conformities were identified. This included with a cross, a dash, a blank space, an asterix or another method observed.
There were also variations observed in other services/branches which included some staff noting aspects not applicable in the same manner as aspects that had not been
completed giving an incorrect overall result. Other staff member (mental health services Hamilton and Tauranga) had noted incorrectly that some aspects were not applicable,
while for some recovery facilitators a number of components were not relevant due to differences in the service’s contractual requirements.
1982
Staff undertaking the self-assessments across most branches/services audited advised they had not received any training on the requirements and process for undertaking
self-assessments and the management of results. Where non conformities were identified in some locations, actions required have been documented and noted to have been
implemented. In other areas it was unclear what actions had been taken in response to findings.
THE
At a previous audit the need to implement a process for the regular review and analysis of staff exit data was raised as an area for improvement. ‘Survey-monkey’ is being
ACT
used to collect exit interview data and the results were sighted for 2017-2019 to date. While staff turnover is being monitored on an ongoing process, analysis of this
information and a clear organisation action plan to address the findings has not been developed.
Finding:
Some staff undertaking self-assessments have not been trained in the process and follow-up action required. There is variation across services / branches in how the results
of self-assessments are documented, the frequency they are conducted, the documentation of results, and the development and follow-up of action plans in response to self-
UNDER
assessment findings.
There is no systematic analysis of staff exit interview data and an organisation wide plan to address findings has not been developed.
Corrective Action:
Provide applicable staff with training on undertaking self-assessments. Ensure self-assessments are undertaken in the required timeframes, the results documented in a
consistent manner, action plans developed where applicable and implemented and monitored for effectiveness.
Analyse staff exit interview data in a timely manner and develop an action plan to address findings.
Timeframe (days): 180
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
INFORMATION
RELEASED
Criterion 2.3.5 (HCS.2012:2.3.5)
The development and implementation of corrective action plans that address areas identified for improvement.
Attainment and Risk: PA Moderate
Evidence:
The HCNZ quality framework 2018-2020 details the ‘plan, do study, act’ quality improvement cycle. In branches audited there were examples of corrective actions or quality
improvement plans developed when areas for improvement or quality improvement opportunities were identified. This included in response to the previous certification audit
OFFICIAL
findings, complaints, incidents, and results of self-assessments. For many of these, there are examples of progress being made to address the issues. However, this is not
Page 38 of 83
Page 38 of 107
Document 1
Home and Community Support Services Audit Report
consistent. Some areas continued to have overdue staff performance appraisals (refer to 3.2.3), overdue client reviews (refer to 4.11.4), overdue competency assessments
(refer to 3.2.3), with limited evidence of progress being made in response to the findings or changing interventions to address the issue, in some cases.
Self-assessments sighted did not always include a documented action plan in response to the findings, or when an action plan was developed, evidence that the interventions
had been undertaken. For example, the follow up in response to self-assessment findings and personnel files in Christchurch has not been completed approximately 12
months after self-assessment was completed. Action plans had not been developed for some self-assessments sampled including for Hamilton community services and
Tauranga rehabilitation services.
Incidents reports sampled in mental health services Hamilton and Tauranga did not always contain information on the results of investigations or interventions undertaken in
response to the events although staff and managers interviewed could describe some of the actions taken. In mental health services Christchurch, documented follow-up was
not present for sampled events, including events that had been reported over three months prior to audit, although the service manager verbalised some of the actions that
had been taken. In Hamilton and Tauranga (community services) incidents did not always include sufficient information on the investigation and / or follow-up undertaken for
1982
sampled events. This included several events related to missed medications, a staff member and professional boundaries and episodes of challenging behaviour. In Hamilton
community services, where assistance was sought from the complex issues group or the national care and protection team, the feedback from these committees was not
THE
linked to or documented in either the clients’ records or incident management process.
While staff turnover is being monitored on an ongoing process and ROMs are developing some strategies to address this issue, analysis of staff exit data and an organisation
ACT
action plan to address the findings has not been developed (refer to 2.3.4).
A staff member has been employed in the Penrose / Albany branches to assist office-based staff in ensuring adverse events and complaints are being investigated and
responded to in a timely manner. Four complaints sampled in Hamilton, and one in Albany did not have all aspects of the complaint investigated or the response / outcome
clearly communicated to the complainant (refer to 1.9.3).
UNDER
Meeting minute templates included detailed what actions are required as either a component of the meeting minutes or noted in an action list attached. Minutes of the
previous meeting are reviewed up each meeting.
Finding:
The corrective actions taken in response to some incidents, complaints, self-assessments and staff exit survey data are not always documented or followed up in a timely
manner. Where advice is sought from the complex issues group or national care and protection team, recommendations received are not always linked to the client record or
incident management system.
Corrective Action:
Ensure corrective action plans are consistently developed in a timely manner where areas for improvement are identified, are implemented, and monitored for effectiveness.
Ensure feedback received from the complex issues group or national care and protection team are linked to the client’s record / incident management system.
INFORMATION
Timeframe (days): 90
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
RELEASED
Standard 2.4: Adverse Event Reporting and Resolution
(HCS.2012:2.4)
All adverse unplanned or untoward events are systematically recorded and reported to affected consumers and where appropriate their family/whānau in an open manner.
Attainment and Risk: FA
OFFICIAL
Evidence: Policies and procedures detail the processes for the reporting, investigating and management of incidents or adverse events. An electronic incident management system
(Promapp) is used to record incidents and accidents with exception of mental health services where incidents are reported electronical y on ‘Recordbase’. Support workers
Page 39 of 83
Page 39 of 107
Document 1
Home and Community Support Services Audit Report
are required to phone the service managers, coordinators or the after-hours service, and alert them of any incidents/events that occur. The service manager is normally
responsible for entering the incident/event on to Promapp and commencing the investigation and follow-up. The recovery facilitators alert the mental health service manager
of events. Recovery facilitators advise they will also discuss events amongst themselves if there is any doubt whether an event should be reported. At the 2016 mental health
certification audit an area for improvement was raised in relation to the implementation of a national incident reporting system, and associated staff training for staff working in
mental health services. These areas have been addressed.
The Promapp data base has fields where staff are to record the incident, investigation and follow-up. Some sampled events have been investigated and followed up in a
comprehensive and timely manner, however there is some variation in this between staff / managers and locations. A number of sampled events did not contain a
comprehensive investigation, or the actions taken were either not documented, or not documented in a timely manner. This is included in the area for improved raised in
2.3.5.
Events reported to the afterhours service are recorded in the client record as a note, and any significant risks identified and addressed. The events are also noted on the
1982
afterhours shift summary report which is reviewed daily by the coordinators and service managers. These events are entered onto Promapp by a member of the quality and
risk team and investigation and the follow-up the responsibility of the applicable line manager.
THE
The type of events sampled across all branches/services included client falls, support worker conduct, damage or loss of property, safety concerns/hazards, medicine
errors/omissions, challenging behaviours, allegations of abuse/neglect and staff injuries/accidents. Advice and support was sought from the complex issues group and the
ACT
organisation’s child protection team where applicable. Refer to 2.3.5 in relation to the need to link feedback received to the incidents/client record. The majority of the reported
events sampled, with infrequent exception, are clearly referenced in the client’s records. This is not raised as an area for improvement as it is not a systemic issue.
Members of the quality and risk team at national office provide a report on the number and type of incidents that are being reported across the organisation as well as each
area. This includes identifying and reporting on the number of incidents, the categories of events and themes and trends. The top five category of reported events are noted
for each area. The locality managers, service managers and the regional operations manager interviewed advise these reports are useful in helping identify if there are any
UNDER
areas where they have incident rates that are significantly different to national rates (refer to 2.3).
Staff related injuries and accidents are being reported and monitored by the national health and safety team members, who report on total numbers of reported events, and
those requiring time off work (refer to 2.3).
Open disclosure is documented as occurring for applicable events sighted and the communications are documented. All clients and the family members interviewed
confirmed they are informed of events or changes in the client's condition in a timely manner by staff.
All the managers and regional operations managers interviewed described their responsibilities in relation to statutory or contractual essential notifications/funder escalation
and reporting guidelines. These are linked to legislation and contractual obligations. The reporting process was described by each locality manager, service manager,
coordinator or clinical services manager and was appropriate for the type of event reported. Examples of essential notifications sighted included allegations of abuse and
INFORMATION
neglect (child and adult), client injuries during care, a client with significant challenging behaviour posing a risk to staff, non-provision of services, and other significant events
that impacted on the health and safety of clients. Managers have recently been provided with training on the essential notification /escalation requirements. Essential
RELEASED
notification communications to ACC are facilitated nationally by the client services manager.
The deaths of two clients have been reported to the Coroner in branches audited. One event has been subsequently closed with the Coroner being satisfied as to the cause
of death. The other inquiry section 9(2)(a)
remains open, with HCNZ being asked to provide information about services provided. For both these events the services provided
by HCNZ are not under investigation in relation to the cause of death, but rather general information sought to inform the overall investigation.
Recommendation:
Click here to enter text.
OFFICIAL
Page 40 of 83
Page 40 of 107
Document 1
Home and Community Support Services Audit Report
Criterion 2.4.1 (HCS.2012:2.4.1)
The service provider documents adverse, unplanned, or untoward events including service/service delivery shortfalls in order to identify opportunities to improve service
delivery, and to identify and manage risk.
Attainment and Risk: FA
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
1982
Corrective Action:
Click here to enter text.
THE
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
ACT
Criterion 2.4.2 (HCS.2012:2.4.2)
The adverse event reporting system is a planned and co-ordinated process that links to the quality and risk management system.
UNDER
Attainment and Risk: FA
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
INFORMATION
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
RELEASED
Criterion 2.4.3 (HCS.2012:2.4.3)
Adverse, unplanned, and untoward events are addressed in an open manner.
Attainment and Risk: FA
Evidence:
OFFICIAL
Click here to enter text.
Finding:
Click here to enter text.
Page 41 of 83
Page 41 of 107
Document 1
Home and Community Support Services Audit Report
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Criterion 2.4.4 (HCS.2012:2.4.4)
The organisation understands their statutory and/or regulatory obligations in relation to essential notification reporting and the correct authority is notified when required.
Attainment and Risk: FA
1982
Evidence:
Click here to enter text.
THE
Finding:
ACT
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
UNDER
Standard 2.5: Entry to and Exit from Services
(HCS.2012:2.5)
Consumers’ entry into and exit from services is facilitated in an equitable, timely, and respectful manner.
Attainment and Risk: FA
Evidence: The mental health service operations manual includes policies on entry to services, declining referrals and planned discharge from the service and includes a step by step
INFORMATION
procedures to guide staff. The declining referral policy was last reviewed in March 2019. The policy is clear that a referral can only be declined by the service manager and
lists the reasons for declining. If a decision is made to decline, the referral status held electronically (Recordbase) is updated with the reason for decline. Review of the
RELEASED
database confirmed this. The policy also details the method to be used to advise the referrer of the decline.
The policy documents that if the mental health service is unable to provide support due to capacity and the person requires support earlier than a wait list may be able to offer,
the person will be referred to another provider as opposed to being ‘wait listed’. The service manager for Hamilton and Tauranga stated they do not have waiting lists, rather
the status of the person is ‘pending’ until all information is gathered. If the service is unable to accept the person, another organisation will be suggested. The Christchurch
branch contract with the DHB is for people over the age of 65 years. The service manager stated all referrals are ‘pending’ initially and then go on to a wait list which is
prioritised urgent or semi-urgent. People are not declined unless they have a physical disability or dementia.
Recovery facilitators demonstrated they are knowledgeable with regards to knowing what the procedure is for ensuring the safety of clients and/or staff. The service manager
OFFICIAL
for the Hamilton and Tauranga branches reported two staff always attend the first home visit and includes either a recovery facilitator or the service manager and a clinical key
worker from the DHB mental health team. In the Christchurch branch the service manager and a recovery facilitator attend the first home visit.
Page 42 of 83
Page 42 of 107
Document 1
Home and Community Support Services Audit Report
The ‘Planned Discharge from Services’ policy is current and was last reviewed March 2019. The policy includes a list of reasons for discharging people from the service. A
planned and coordinated approach is taken on exit from services. Discharge planning is discussed with the person and their family/EPOA at the initial visit and documented in
the service plan and involves the person’s clinician or their GP. The service managers confirmed this. Files of people who have left the service in the Hamilton and Tauranga
branches evidenced the organisation’s processes were fol owed and included a discharge plan, a discharge checklist and a discharge letter to the person discharged from the
service. In the Christchurch branch clients are discharged after 12 months. Planning for discharge starts two months prior to the discharge date. Once discharged, the case
manager or the client’s GP can refer the client back to the service if required. Clients can be exited prior to 12 months or they can exit the service themselves.
The finding from the last mental health certification audit in 2016 has been addressed and is now closed.
Recommendation:
Click here to enter text.
1982
THE
Criterion 2.5.1 (HCS.2012:2.5.1)
ACT
Access processes and entry criteria are clearly documented, and are communicated to consumers, their family/whānau of choice where appropriate, local communities, and
referral agencies.
Attainment and Risk: FA
Evidence:
UNDER
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
INFORMATION
Criterion 2.5.2 (HCS.2012:2.5.2)
RELEASED
There is a planned exit in co-operation with the consumer and this is documented, communicated, and effectively implemented.
Attainment and Risk: FA
Evidence:
Click here to enter text.
Finding:
OFFICIAL
Click here to enter text.
Corrective Action:
Click here to enter text.
Page 43 of 83
Page 43 of 107
Document 1
Home and Community Support Services Audit Report
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Criterion 2.5.3 (HCS.2012:2.5.3)
The organisation operates at times most appropriate to meet the needs of the consumer group.
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
1982
Finding:
Click here to enter text.
THE
Corrective Action:
ACT
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
UNDER
Standard 2.6: Consumer Information Management Systems
(HCS.2012:2.6)
Consumer information is uniquely identifiable, accurately recorded, current, confidential, and accessible when required.
Attainment and Risk: FA
Evidence: The mental health services have al moved to using ‘Recordbase’ to record client records and ensure integrated records are readily accessible/available. The shortfall from
the 2016 mental health certification audit has been addressed.
The other community services are using a combination of Goldcare, Caduceus and an upgraded Care Call system. There is a national programme underway to convert all the
INFORMATION
client management systems (excluding mental health) to Care Call. This requires specific planning per site, testing data sources and transfer, and review of the outcome of
migration of large quantities of information. Due to the scale of this project and resources required, this is occurring in one geographical area at a time. Office based staff have
RELEASED
access to the applicable client management systems for their branch or service.
In association with the move to Care Call for client management systems, HCNZ has introduced an electronic time and attendance record (ETAR) instead of paper-based
timesheets. This is a new initiative, in the beginning stages of implementation and is currently not compulsory for staff. This will reduce the amount of client related information
that support workers / recovery facilitators carry with them in paper form. Other staff are sent rosters and timesheets which contains some client information including the
client name, contact details / address. However, in the interim the service requirements for maintaining the confidentiality of timesheets, rosters and other client information
has been clearly communicated to staff and is noted in policy/procedures. All support workers and recovery facilitators interviewed in all branches could detail the
organisation’s requirements for maintaining the privacy of client information and how the information was to be destroyed when no longer required. Support workers have
OFFICIAL
details of only one client on each timesheet. The theft of information from a support worker’s locked vehicle and from the mail delivery services was promptly reported via the
incident reporting system and investigated. The clients and/or next of kin were informed of the potential privacy breech and the funders notified. The service is managing
processes well and the shortfall from the 2017 certification audit has been sufficiently addressed.
Page 44 of 83
Page 44 of 107
Document 1
Home and Community Support Services Audit Report
Recommendation:
Click here to enter text.
Criterion 2.6.1 (HCS.2012:2.6.1)
Information is entered into the consumer information management system in an accurate and timely manner, appropriate to the service type and setting.
Attainment and Risk: Not Audited
1982
Evidence:
Click here to enter text.
THE
Finding:
Click here to enter text.
ACT
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
UNDER
Criterion 2.6.2 (HCS.2012:2.6.2)
The detail of information required to manage consumer records is recorded relevant to the service type and setting.
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
Finding:
INFORMATION
Click here to enter text.
RELEASED
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
OFFICIAL
Page 45 of 83
Page 45 of 107
Document 1
Home and Community Support Services Audit Report
Criterion 2.6.3 (HCS.2012:2.6.3)
A record of past and present consumers is maintained.
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
1982
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
THE
ACT
Criterion 2.6.4 (HCS.2012:2.6.4)
Management of health information meets the requirements of appropriate legislation and relevant professional and sector Standards where these exist.
Attainment and Risk: FA
UNDER
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
INFORMATION
RELEASED
Criterion 2.6.5 (HCS.2012:2.6.5)
Information of a private or personal nature is maintained in a secure manner that is not publicly accessible or observable.
Attainment and Risk: FA
Evidence:
Click here to enter text.
OFFICIAL
Finding:
Click here to enter text.
Page 46 of 83
Page 46 of 107
Document 1
Home and Community Support Services Audit Report
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Criterion 2.6.6 (HCS.2012:2.6.6)
Service providers use up-to-date and relevant consumer records.
Attainment and Risk: Not Audited
1982
Evidence:
Click here to enter text.
THE
Finding:
ACT
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
UNDER
Criterion 2.6.7 (HCS.2012:2.6.7)
All records are legible and the name and designation of the service provider is identifiable.
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
INFORMATION
Finding:
Click here to enter text.
RELEASED
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
OFFICIAL
Page 47 of 83
Page 47 of 107
Document 1
Home and Community Support Services Audit Report
Standard 2.7: Essential and Emergency Systems
(HCS.2012:2.7)
Consumers receive an appropriate and timely response during emergency and security situations.
Attainment and Risk: PA Low
Evidence: The branch emergency plan is aligned to the regional plan. The electronic client management system includes information and planning relating to the individual client in
emergency situations and can be accessed nationally. Each client is required to have an assigned client priority level based on assessed risk to facilitate priority emergency
response. The client's plan considers their level of mobility, independence and the individual’s living situation, whether living alone or with others. This information is linked to
the branch and the disaster management activities, nationally.
1982
The Hamilton and Tauranga branches have a ‘Grab and Go’ file that has been developed and includes all information for an emergency, should the electronic management
system fail.
THE
The mental health service Christchurch has an emergency list of clients, with their address and phone numbers. The service manager reported they do not have a priority
rating for clients. Clients' service plans contained instructions and information for use in the event of an emergency. Clients interviewed using mental health services knew
ACT
about their individual information relating to emergency situations. The finding from the mental health service certification audit of 2016 remains open.
Recommendation:
Click here to enter text.
UNDER
Criterion 2.7.1 (HCS.2012:2.7.1)
Service providers receive appropriate information, training, and equipment to respond to identified emergency situations. This shall include fire safety and emergency
procedures.
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
INFORMATION
Finding:
Click here to enter text.
RELEASED
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
OFFICIAL
Page 48 of 83
Page 48 of 107
Document 1
Home and Community Support Services Audit Report
Criterion 2.7.2 (HCS.2012:2.7.2)
The organisation, in consultation with the consumer, identifies and implements an appropriate plan relevant to the consumer’s needs in an emergency.
Attainment and Risk: PA Low
Evidence:
The mental health service is included in the branch emergency plan and is aligned to the regional plan depending on where the branch is situated. The electronic client
management system (Recordbase) includes information and planning relating to the individual client in emergency situations and this information can be accessed nationally.
Each client is required to have an assigned client priority level based on assessed risk to facilitate an emergency response. This is reviewed as part of the client reviews and
updated if required. The client's plan and emergency rating considers their level of mobility, independence and the individual’s living situation, whether living alone or with
others. This information is linked to the branch and the disaster management activities, nationally.
1982
The mental health service Hamilton and Tauranga have a ‘Grab and Go’ file. This file includes priority codes, emergency phone numbers, contact family numbers and clients’
numbers. The file is a ‘back-up’ should a situation occur where due to an emergency, the electronic management system has failed.
THE
The mental health service Christchurch has an emergency list of clients, with their address and phone numbers which is updated monthly. The service manager reported they
do not have a priority rating for clients. The service manager advised that during the latest emergency in Christchurch, all clients using the mental health service were phoned
ACT
to ensure they were safe and supported.
Finding:
Mental Health Christchurch has a list of client addresses and phone numbers; however, a priority list based on risk has been not been developed.
Corrective Action:
UNDER
Expand the list of client addresses and phone numbers to include a priority list based on risk for use in an emergency.
Timeframe (days): 90
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Criterion 2.7.3 (HCS.2012:2.7.3)
Consumers who require a greater degree of supervision receive the level of support necessary to protect their safety in the event of an emergency.
Attainment and Risk: Not Audited
INFORMATION
Evidence:
RELEASED
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
OFFICIAL
Page 49 of 83
Page 49 of 107
Document 1
Home and Community Support Services Audit Report
Outcome 3: Human Resources
Consumers receive safe, efficient, and effective services from an organisation that is a good employer and follows accepted human resource practices.
Standard 3.1: Recruitment
(HCS.2012:3.1)
Consumers receive services that are based on good employment practices and relevant legislation.
Attainment and Risk: Not Audited
Evidence:
1982
Click here to enter text.
Recommendation:
THE
Click here to enter text.
ACT
Criterion 3.1.1 (HCS.2012:3.1.1)
The skills, knowledge, and attitudes required of each position are identified and its functions, accountabilities, responsibilities, and authority as well as the outcomes to be
UNDER
achieved in each position, are documented.
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
INFORMATION
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
RELEASED
Criterion 3.1.2 (HCS.2012:3.1.2)
The organisation uses a documented recruitment procedure that includes interviewing, reference checking, police record checking, and providing an employment agreement
that complies with relevant legislation.
OFFICIAL
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
Page 50 of 83
Page 50 of 107
Document 1
Home and Community Support Services Audit Report
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Standard 3.2: Orientation, Induction, Ongoing Development, and Competency
(HCS.2012:3.2)
1982
Consumers receive services from service providers who are trained and assessed as competent to provide services.
THE
Attainment and Risk: PA Moderate
Evidence:
ACT
A comprehensive induction / orientation programme sighted is required to be completed by all new staff prior to delivering services and introduces support workers and
recovery facilitators to the organisation, key personnel, policies and procedures and their roles and responsibilities and help identify any gaps in competency. Records are
maintained electronically via ‘learning tree’ to verify that new staff are completing the requirements. The orientation training package is then completed by the support workers
/ recovery facilitator. The orientation programme for support workers includes being buddied with an allocated ‘buddy trainer’, an experienced support worker allocated to work
alongside new staff. The buddy role is a formal role and applicable staff are required to complete a one-day training programme. The buddies work with new staff for up to
three days to teach the new support worker aspects of the role and then ensure the support worker can safely complete all the generic personal cares and household
UNDER
management tasks required via ‘buddy verification’. Additional time can be allocated if required where a new support worker is identified as needing additional training/time.
Following this the support worker has a meeting with either the locality manager, a coordinator or a service manager to complete the manager verification component. This
includes asking the staff member questions about key aspects of service delivery to ensure the staff member understands the requirements. Both the buddy observation
documents and the manager verification documents are sent through to the national learning and development service. There is some variation in processes associated with
this. In some locations a copy of the buddy and manager assessments are placed on the support worker’s electronic file, in other locations a copy is held in the employee’s
paper based personnel file, and in other areas there is no reference at all to these having been completed as the forms were submitted directly to learning and development
staff in the affiliated business entity ‘My Skil s’, who are responsible for overseeing the organisation wide generic learning and development activities. The learning and
development service issue regular ‘learning tree’ reports to line managers detailing new employees, components of orientation completed and any outstanding activities. The
staff members stay on this list until all required components have been completed. The ‘learning tree’ reports are considered the ‘source of truth’, and staff in the learning and
INFORMATION
development service are responsible for ensuring appropriate orientation records are maintained. Over time it is anticipated that line managers will be able to access the
‘learning tree’ databases directly, however this is not currently possible.
RELEASED
New support workers are also required to complete e-learning modules; your role as a support worker, take care, taking care (health and safety video) and medication (stage
one) – prompting.
Support workers interviewed in the community and rehabilitation services reported that the changes made to the orientation programme has been very positive and has
improved the overall orientation process, enhanced consistency and created a more positive experience for new and existing staff.
Role specific orientation programmes are in place for coordinators, registered health professionals and managers, and records are held electronically or in paper-based files.
Examples were sighted of staff working to complete the orientation requirements.
OFFICIAL
Recovery facilitators in Hamilton and Tauranga have completed the organisation’s mental health orientation programme and records are maintained. The service manager of
mental health services in Christchurch has developed his own orientation programme for staff. This does not include all required topics, such as abuse and neglect, infection
prevention and control. This is now included in the area for improvement raised in 3.2.2. New recovery facilitators are automatically enrolled in the e-learning modules
Page 51 of 83
Page 51 of 107
Document 1
Home and Community Support Services Audit Report
personal safety and conflict awareness, and safe lone worker. Recovery facilitators interviewed in all branches felt the orientation programme suitably prepared them for their
role and responsibilities. The shortfall raised at the 2016 mental health certification audit and the 2017 verification audit have been addressed.
Placement with individual clients by the coordinator or service manager are based on the competencies achieved by support workers. Some staff are overdue annual
competency assessments and performance appraisals. The shortfall raised at the 2017 certification audit and 2017 verification audit continue to be areas requiring
improvement.
Ongoing training relevant to staff roles and responsibilities is planned and facilitated by the learning and development team based in the associated company ‘My Skills’
nationally, and by line managers. Ongoing training has not been provided to recovery facilitators working in the mental health service in Christchurch. The shortfall from the
2016 mental health certification audit continues to be an area requiring improvement.
Support workers and recovery facilitators confirmed they felt confident and supported to carry out their roles competently. They report they can contact the coordinators or
1982
services managers, or registered health professionals, and the after-hours staff when they need to. Clients and family members interviewed verified they were satisfied
support workers were given appropriate training and were competent to provide their required care. Recovery facilitators have regular meetings with their service manager to
discuss clients and their needs. External supervision arrangement is also in place for recovery facilitators in Christchurch.
THE
Systems are in place to support staff members who are registered health professionals (RHPs) to maintain their registration and operate within their scope of practice. All
ACT
RHPs interviewed reported being well supported to access education internally and externally and had no problems meeting the education hours required to maintain their
annual practising certificates (APCs). The organisation has a professional development and recognition programme. Staff are being encouraged to complete their portfolios.
Renewal of APCs is overseen nationally. A data base is maintained by an administrator in Wellington. All RHPs in the branches audited have a current APC.
Processes are in place to monitor the number of MidCentral DHB clients who are receiving services provided by a family member. Reports are issued to the DHB on a regular
basis. At audit there are eight family members providing care.
UNDER
Recommendation:
Copies of industry approved qualification records / certificates are obtained for the staff records where employees have qualifications at employment.
Criterion 3.2.1 (HCS.2012:3.2.1)
An induction process is completed by all service providers, prior to commencement of duties, and a record of the induction programme and attendance is maintained.
INFORMATION
Attainment and Risk: FA
Evidence:
RELEASED
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
OFFICIAL
Page 52 of 83
Page 52 of 107
Document 1
Home and Community Support Services Audit Report
Criterion 3.2.2 (HCS.2012:3.2.2)
A developed, implemented, and recorded training plan relevant to the service provider’s scope of practice is maintained.
Attainment and Risk: PA Moderate
Evidence:
Following induction, support workers are registered to complete level two of an industry recognised qualification if they do not already have an industry approved qualification
at level two or higher. Progress in monitoring staff completion is undertaken via ‘learning tree’ and line managers and coordinators kept updated.
The line managers interviewed are aware of contractual requirements related to staff working with complex needs clients. Support workers are provided with the opportunity to
complete a level three industry approved qualifications. Several support workers interviewed were currently working to complete a level four industry approved qualification.
1982
A variety of e-learning programmes have been developed and are available for staff on ‘learning tree’ or via scheduled in-service. Topics include (but are not limited to)
manual handling, positive behaviours, autism, pal iative care, ‘open minds open doors’. Each branch negotiates ongoing education priorities with the learning and
THE
development staff or local health agencies, for example, Alzheimers New Zealand and Aged Concern, based on staff need, contractual obligations, incidents and complaints
and or staff request. Approximately 75% of support workers in Christchurch have completed the ‘walking in other’s shoes’ training provided by the DHB over an eight month
period.
ACT
Recovery facilitator ongoing training is discussed and planned in the regular staff meetings in Hamilton and Tauranga. A schedule of topics for 2019 was sighted. Recovery
facilitators interviewed in Hamilton and Tauranga confirmed education is provided in a timely manner including on topics relevant to their role and where a need has been
identified, or when requested by staff. Recovery facilitators working in Christchurch advise they have not participated in ongoing education for approximately 18 months
despite requests and the training calendar that had been developed. Management of actual or potential aggression ‘MAPA’ training has subsequently been scheduled for
Christchurch mental health staff.
UNDER
Monthly education sessions are planned and provided to registered health professionals. The topics are advised in advance and all staff nationally are invited to join via the
internet or telephone.
Finding:
Whilst a training plan has been developed for recovery facilitators working in Christchurch, training is not consistently being provided. Records are not available to
demonstrate that staff working in this service have completed training on abuse and neglect, management of actual or potential aggression /challenging behaviour training,
and infection prevention and control.
Corrective Action:
INFORMATION
Implement a training plan relevant to the service and include topics detailed above.
Timeframe (days): 90
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
RELEASED
Criterion 3.2.3 (HCS.2012:3.2.3)
There is a system to determine and develop the competencies of the organisation’s service providers to meet the needs of consumers. This shall be achieved by, but is not
limited to:
(a) The service provider’s competency is assessed against the organisation’s policies and procedures;
OFFICIAL
Page 53 of 83
Page 53 of 107
Document 1
Home and Community Support Services Audit Report
(b) Competency gaps between consumer’s needs and service provider’s competency are identified;
(c) Specialist advice, training, information, and oversight are provided by individuals who are trained/qualified and competent to undertake this role.
Attainment and Risk: PA Moderate
Evidence:
There is a competency assessment framework which has been reviewed since the last audit and includes but is not limited to medicine management, thrombolytic embolism
stockings (TEDS), testing blood glucose levels stoma management, bowel cares, catheter management, assisted cough, care of clients with fentanyl patches, and
compression stockings and other clinical components relevant to individual clients. The medicine competency framework has been changed. The competency for medicine
prompting is included with induction/orientation. The new stage three medicine management includes application of eye drops and eardrops, transdermal medicines and
subcutaneous injections. Records are made of when staff have completed training although the annual review dates are not always noted, and this along with other work
pressures have resulted in some staff being overdue for annual review. Some of the competencies are assessed individually with support workers, others assessed as a team
1982
of staff caring for an applicable client and some are undertaken in generic group sessions. For example, in Christchurch, support workers come into the office to complete a
competency afternoon that includes TEDS, medicines and other components. In all locations audited excluding Hamilton community services, a number of support staff are
THE
overdue one or more aspects of their annual competency reassessment. Recovery facilitators are required to have a level four industry approved qualification as their
competency assessment. Service managers advise they sight copies of the qualification certificate during staff interviews and note these, but do not always obtain a copy for
ACT
the employees file. A recommendation is made that copies are consistently obtained.
In Hamilton, staff caring for children under the medically fragile contract are required to have been assessed for specific activities prior to caring for applicable children and to
complete reassessment annually for a range of care activities including but not limited to use of oxygen, percutaneous endoscopic gastrostomy (PEG) devices, seizure
management, care of tracheostomy, diabetes (high and low blood glucose levels), ‘J tube’ and low button. These were current for all applicable staff. A register is maintained
to details when the applicable support workers are due to be reassessed. All support workers caring for the children under this contract are required to have a current first aid
UNDER
certificate, and records demonstrate this is occurring.
Support workers caring for complex rehabilitation clients including those with spinal cord injuries (SCI) or traumatic brain injuries (TBI) are required to undertake baseline, SCI
and / or TBI specific competency assessments prior to caring for applicable clients and then again annually thereafter. The assessments are conducted by a registered health
professional (RHP) and includes catheter management, bowel cares, suppository administration, pressure injury prevention, managing challenging behaviours and other
relevant components. Records are retained of when staff are due. This includes on the support workers electronic personnel file and / or on spreadsheets maintained by
designated staff. In Christchurch, staff advised the annual TBI, SCI and baseline reassessments were no longer required for applicable staff and as a result were not being
completed. In all locations audited, a number of support workers caring for the complex clients are overdue one or more of these annual competency re-assessments.
Staff are required to have an annual performance appraisal. In the last 12 months the appraisal process for support workers has been streamlined / simplified. This is a focus
for line managers, and some actions have been taken to improve completion rates with the number of staff overdue appraisals being monitored on a monthly basis. However,
INFORMATION
despite this a significant number of support workers in each location audited excluding staff working in Hamilton ‘community’ services are overdue annual performance
appraisals.
RELEASED
Appraisals were current for all the recovery facilitators in Hamilton and Christchurch and were initially overdue for three recovery facilitators in Tauranga. The service manager
advised this was due to misreading the date of the last appraisal as all other staff had been completed. The service manager subsequently provided evidence the overdue
appraisals were completed prior to the completion of this audit.
Concerns were expressed by some office based staff about the time needed to complete the verifications on employment and competency assessments. Timeliness has also
been impacted by the significant organisation change as well as turnover / vacancies in service coordinator and registered health professional roles in some branches.
Finding:
OFFICIAL
Some support workers are overdue annual performance appraisals in all locations audited except mental health services and Hamilton community services.
Page 54 of 83
Page 54 of 107
Document 1
Home and Community Support Services Audit Report
Some support workers, including those caring for clients with traumatic brain injuries, spinal cord injuries are overdue annual competency review in all locations audited
except Hamilton community services.
Corrective Action:
Ensure staff consistently complete competency requirements and records are retained.
Undertake annual performance appraisals for staff
Timeframe (days): 90
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
1982
Criterion 3.2.4 (HCS.2012:3.2.4)
Service providers understand the scope of their role and the support available to them. This shall be achieved by, but is not limited to:
THE
(a) Direct support is part of each service provider’s position description and the level of assistance/intervention is clearly defined in a consumer’s individual service plan;
(b) Service providers clearly recognise and understand their defined role and responsibilities;
ACT
(c) Service providers clearly understand how to seek assistance or advice when the limit of their competency, knowledge, or experience is reached.
Attainment and Risk: FA
Evidence:
Click here to enter text.
UNDER
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
INFORMATION
Criterion 3.2.5 (HCS.2012:3.2.5)
RELEASED
The organisation ensures that all service providers access supervision and support.
Attainment and Risk: FA
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
OFFICIAL
Corrective Action:
Click here to enter text.
Page 55 of 83
Page 55 of 107
Document 1
Home and Community Support Services Audit Report
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Criterion 3.2.6 (HCS.2012:3.2.6)
The organisation implements a policy and procedure to assist registered health practitioners retain their registration and operate within their scope of practice.
Attainment and Risk: FA
Evidence:
Click here to enter text.
1982
Finding:
Click here to enter text.
THE
Corrective Action:
ACT
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
UNDER
Standard 3.3: Health and Safety
(HCS.2012:3.3)
Consumers receive services that promote the health and safety of the consumer and service providers.
Attainment and Risk: Not Audited
Evidence: Click here to enter text.
Recommendation:
Click here to enter text.
INFORMATION
RELEASED
Criterion 3.3.1 (HCS.2012:3.3.1)
Service providers are issued with, given training in, and follow a written policy that clearly identifies requirements of the Health and Safety in Employment Act. The policy shall:
(a) Be authorised by the organisation;
(b) Incorporate the organisation’s commitment to comply with relevant legislation, regulations, codes of practice, and safe operating procedures;
OFFICIAL
Page 56 of 83
Page 56 of 107
Document 1
Home and Community Support Services Audit Report
(c) Specify the organisation’s responsibilities for health and safety;
(d) Specify service providers’ responsibilities for health and safety.
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
1982
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
THE
ACT
Criterion 3.3.2 (HCS.2012:3.3.2)
The policy shall include a process for:
(a) The active identification and management of existing hazards (which may include consumer behaviour) associated with the service;
(b) Regularly assessing each hazard identified (including any new hazard), determining whether or not it is a significant hazard, and if it is eliminating, isolating, or minimising
UNDER
it to the extent possible within the home environment;
(c) Ensuring service providers are allocated to consumers in a way that minimises risk of injury;
(d) Enabling service providers to have an emergency plan that meets relevant emergency service requirements to evacuate from potential emergency situations;
(e) Responding to a health and safety incident in the workplace that may include access to first aid and emergency treatment;
(f) Providing debriefing and post-incident support that may include counselling;
(g) Ensuring that corrective action is undertaken on any deficiencies identified during an investigation of incidents, injuries, and work-related illnesses.
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
INFORMATION
Finding:
RELEASED
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
OFFICIAL
Page 57 of 83
Page 57 of 107
Document 1
Home and Community Support Services Audit Report
Outcome 4: Service Delivery
Consumers receive services that contribute to their agreed outcomes, and that support their independence, safety, and well-being.
Standard 4.01: Service Agreement
(HCS.2012:4.01)
The consumer, organisation, and service provider have a full understanding of and agree to the services to be provided.
Attainment and Risk: FA
Evidence:
1982
The service agreements meet the requirements of the standard. A copy of this agreement, once signed, is retained by the service and a copy provided to the client. Clients
confirmed this. Clients reported they are happy with the agreement they have and are aware they can change support workers if they wish. They also reported that they were
THE
satisfied with the times their service is delivered as well as the reliability of the service.
The service coordinators, service managers, recovery facilitators and registered health professionals confirmed they can negotiate with clients to agree to a time that suits at
ACT
the initial visit. Changes are made to rostered duty times to fit in with clients’ wishes and attendance at activities or appointments as and when they are planned. Regular
appointments and activities in the community are detailed during the service planning process and included in both service plans and support plans. Clients confirmed
appropriate support is provided to attend regular activities and appointments to assist in their rehabilitation and recovery in a timely way.
The service plan for the mental health service clients has been reviewed and updated. The service plan includes services specific to the individual client and the timeframes
for when the services are to occur. The service agreement for the mental health service meets all the requirements of the standard. The finding from the mental health
UNDER
certification audit of 2016 has been addressed and is now closed.
The service managers and operations managers reported that a national project is in place and all service agreements currently in use are being reviewed. It is envisaged that
there will be one service agreement with specific attachments for the different service streams.
Service coordinators in the Palmerston North branch reported they can access the interRAI assessments for referrals from the DHB. The manager reported they are working
with the DHB with regards to being provided with more information especially for people with complex clinical issues. A regional clinical manager, which is a new position, has
been in the role for three months and has made a difference in terms of information sharing. An electronic programme is used to assess the level of need and this is used to
triage clients. The interRAI is reviewed and any detail is forwarded to the service coordinators. This has meant the right level of support is able to be provided. InterRAI
electronic communication was reviewed and evidenced detailed information.
INFORMATION
Recommendation:
Click here to enter text.
RELEASED
Criterion 4.01.1 (HCS.2012:4.01.1)
Each consumer shall have a written service agreement with the organisation providing the services. The written service agreement shall be in languages and formats suited to
the needs of the consumer. It shall explain the services to be provided. The agreement shall include, but not be limited to:
OFFICIAL
(a) Name, address, and telephone number of the organisation including out of hours and emergency contact details;
(b) Name, address, and telephone number of the consumer;
(c) Services provided as part of the agreement, including when or how frequently, and by whom;
Page 58 of 83
Page 58 of 107
Document 1
Home and Community Support Services Audit Report
(d) Any fees payable for the service, when or how frequently, by whom, and options for how payments can be made;
(e) Rights and responsibilities of both parties;
(f) Obligations of the consumer for the health and safety of the service provider;
(g) Any equipment and supplies to be made available by the consumer or organisation;
(h) The use of equipment and enablers as part of service delivery;
(i) Consent to retain consumer’s information and the purpose for which it wil be used;
(j) A statement outlining the organisation’s policy on the handling of the consumer’s money;
(k) Circumstances in which the service may be cancelled by either party;
(l) That the client should be able to ask for a different service provider if the person assigned is not right for them. This may be particularly important if the service includes
personal care;
(m) How long the service will be provided (if known) and the process for ending it.
1982
Attainment and Risk: FA
THE
Evidence:
Click here to enter text.
ACT
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
UNDER
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Criterion 4.01.2 (HCS.2012:4.01.2)
Consumers receive services at times which meet their needs and the support they require.
Attainment and Risk: FA
Evidence:
INFORMATION
Click here to enter text.
RELEASED
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
OFFICIAL
Page 59 of 83
Page 59 of 107
Document 1
Home and Community Support Services Audit Report
Criterion 4.01.3 (HCS.2012:4.01.3)
The consumer receives a copy of the agreement signed by the organisation and the consumer or the consumer’s representative.
Attainment and Risk: FA
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
1982
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
THE
ACT
Standard 4.02: Promoting and Supoporting Independence
(HCS.2012:4.02)
Consumers maintain their independence during the course of service delivery by being supported to exercise choice and control over their lives.
Attainment and Risk: FA
UNDER
Evidence: The three services (community, rehabilitation and mental health) all have different service plan templates. Assessment and planning for clients document the level of support
required. The mental health service plan includes a section on current strengths and future wishes. Recovery facilitators and support workers were clear about what clients
wish to achieve, what they are able to achieve themselves and what support is required. Staff and clinicians involved in the initial visit to the client’s home ensure clients have
the support they need to make their own decisions. If a client is unable to represent themselves, their family is present and if that is not possible, another independent person.
The individual service plan/support plans are completed with relevant details to indicate levels of support needed to maximise client involvement. Plans reviewed evidenced
goals are set for recovery, returning to and maximising independence and for the older clients who require general household support and personal support, maintaining their
levels of independence as much as possible. The service plans document accessing the wider community and there were good examples sighted in the plans reviewed.
INFORMATION
Clients interviewed using the three different service streams confirmed they are well supported, feel in control of the services they are receiving and that they can maintain
their links with family/whanau and the community.
RELEASED
Interviews with service managers, registered health professionals, RNs, service coordinators, recovery facilitators and support workers confirmed that staff are committed to
supporting clients to maintain their independence and exercise autonomy. Staff, managers and coordinators hold regular discussions/meetings to review the levels of support
required for clients as they increase or maintain their levels of independence and recovery.
Whether clients are using mental health services, rehabilitation services or community services there is a strong focus on returning clients to levels of independence
experienced prior to injury, for other clients, maintaining their current level of independence and for mental health clients, recovery. Case managers and key workers work
closely with the services and this enables additional support to be given to clients who would benefit from an increase or change to the type of support they receive to promote
their independence.
OFFICIAL
Recommendation:
Click here to enter text.
Page 60 of 83
Page 60 of 107
Document 1
Home and Community Support Services Audit Report
Criterion 4.02.1 (HCS.2012:4.02.1)
Consumers are supported to make decisions about their own lives in their own homes.
Attainment and Risk: FA
Evidence:
Click here to enter text.
1982
Finding:
Click here to enter text.
THE
Corrective Action:
Click here to enter text.
ACT
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
UNDER
Criterion 4.02.2 (HCS.2012:4.02.2)
Consumers are supported to undertake tasks and activities and the individual service plan documents their wishes in relation to lifestyle choices. Note: The consumer's rights
and legal choices shall only be limited by clearly defined legal grounds.
Attainment and Risk: FA
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
INFORMATION
Corrective Action:
RELEASED
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
OFFICIAL
Page 61 of 83
Page 61 of 107
Document 1
Home and Community Support Services Audit Report
Criterion 4.02.3 (HCS.2012:4.02.3)
When the consumer is unable to represent themselves input is sought from the consumer’s family/whānau or other designated representative.
Attainment and Risk: FA
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
1982
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
THE
ACT
Criterion 4.02.4 (HCS.2012:4.02.4)
Consumers are supported to maintain links with their family/whānau and to access services within the community.
Attainment and Risk: FA
UNDER
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
INFORMATION
RELEASED
Standard 4.03: Links with Other Groups
(HCS.2012:4.03)
Consumers receive continuity of service through effective links with other groups.
Attainment and Risk: Not Audited
Evidence: Click here to enter text.
OFFICIAL
Recommendation:
Click here to enter text.
Page 62 of 83
Page 62 of 107
Document 1
Home and Community Support Services Audit Report
Criterion 4.03.1 (HCS.2012:4.03.1)
Links are identified and maintained with key groups, including primary healthcare teams, to facilitate continuity of service.
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
1982
Finding:
Click here to enter text.
THE
Corrective Action:
Click here to enter text.
ACT
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
UNDER
Criterion 4.03.2 (HCS.2012:4.03.2)
There is evaluation of the effectiveness of their links with other key health groups.
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
INFORMATION
Corrective Action:
Click here to enter text.
RELEASED
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
OFFICIAL
Page 63 of 83
Page 63 of 107
Document 1
Home and Community Support Services Audit Report
Criterion 4.03.3 (HCS.2012:4.03.3)
Consumers are advised of options to access services from other groups.
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
1982
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
THE
ACT
Criterion 4.03.4 (HCS.2012:4.03.4)
The consumer’s safety and right to be kept informed in a timely manner is managed by organisations co-operating during the referral process.
Attainment and Risk: Not Audited
UNDER
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
INFORMATION
RELEASED
Standard 4.04: Service Delivery Planning
(HCS.2012:4.04)
Consumers have an individual service plan that describes their goals, support needs, and requirements.
Attainment and Risk: FA
Evidence: All clients’ files reviewed had an individual service plan with support needs and short term and long-term goals clearly recorded. Clients confirmed they are very involved in
OFFICIAL
the development of their goals, in the planning and how this would be achieved. Some clients spoke of involving their family members and other health professionals (e.g.,
from the DHB and ACC). The three service streams use different service/support plans with a mix of handwritten and scanned into the system, hard copies, an electronically
Page 64 of 83
Page 64 of 107
Document 1
Home and Community Support Services Audit Report
written depending on the client management system used. All plans were clear and the templates are in an easy to read format. The support workers confirmed they use the
support plan to guide them in their tasks. Copies are kept in the homes of clients, so they are readily available.
Clients interviewed confirmed their active participation in the development, monitoring of their service and support plans. Family/whanau are involved in these processes, with
the consent of the client.
The non-signing policy includes monitoring and review requirements. The revised policy has been implemented across the organisation. The number of ‘non-signing’ clients in
the community service has decreased. Review of registers confirmed this. Service coordinators reported that some clients are able to sign their service agreements and
service plans as they are ‘one-offs’, but they would find it difficult to sign documents every day. There are clients that are unable to sign support workers time sheets.
However, where there is family living in the same house, they sign for the client. Service coordinators are responsible for monitoring this process and this is reviewed on a
continuous basis with the register and service plan updated and clients contacted. Timesheets reviewed evidenced where a client is unable to sign, the support worker enters
‘worked’ and shows this to the client.
1982
Currently in the rehabilitation service, because the care and support is continuous, if a client is unable to sign the time sheets, the support worker on the next shift signs off the
previous support worker’s time sheet. Team leaders also sign off if need be. The client information system used by the rehabilitation service (CareCall) records the information
THE
and has an alert feature which can be used that corresponds with the event notes.
ACT
The client management system (CareCal ) has the ability to record support workers rostered shift start and finish times. This is achieved with an ‘app’ named ‘Kahu’ that
support workers down-load onto their cell phones. The support worker can see their roster over a six-week period and the service coordinators can make changes in live time.
The support workers use the ‘app’ to clock in when they arrive at a client’s home and when they have finished their shift. The national programme director reported this is
being used currently in a number of branches and is currently being rolled out in others. Review of the information confirmed live information is recorded at branch level and
means support workers no longer need to send in time sheets. The numbers of support workers who are using the ‘app’ differs in the branches audited, however the up-take
is increasing. It is proposed that all service streams in the organisation (excluding mental health) will eventually use ‘CareCal ’ as the client management system.
UNDER
Clients interviewed were happy with the process in place if for some reason they could not sign the support worker’s time sheet.
The finding identified at the certification audit of 2017 relating to non-signing clients has been addressed and is now closed.
Recommendation:
Click here to enter text.
INFORMATION
Criterion 4.04.1 (HCS.2012:4.04.1)
RELEASED
An individual service plan is developed to reflect the consumer’s goals, support needs, and requirements. This shall include, but is not limited to:
(a) Where more than one organisation is involved, the development of the individual service plan is co-ordinated;
(b) Where the organisation responsible for developing the individual service plan is different to the organisation responsible for service delivery, linkages exist between the
two;
(c) The individual service plan reflects any natural supports/family/whānau;
(d) The individual service plan reflects the home environment;
OFFICIAL
Page 65 of 83
Page 65 of 107
Document 1
Home and Community Support Services Audit Report
(e) The individual service plan reflects the consumer’s support needs and goals;
(f) The individual service plan defines the use of equipment and enablers as part of service delivery and sets out service provider responsibilities.
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
1982
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
THE
ACT
Criterion 4.04.2 (HCS.2012:4.04.2)
The consumer is actively involved in consultation, planning, monitoring, and implementation of the individual service plan. With consent, family/whānau and other service
providers as relevant are actively involved in any or each of these parts of the development of the individual service plan.
Attainment and Risk: FA
UNDER
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
INFORMATION
RELEASED
Criterion 4.04.3 (HCS.2012:4.04.3)
The individual service plan is developed and agreed with the consumer prior to commencement of service delivery and clearly details the actions to be taken by the service
provider(s).
Attainment and Risk: Not Audited
Evidence:
OFFICIAL
Click here to enter text.
Page 66 of 83
Page 66 of 107
Document 1
Home and Community Support Services Audit Report
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Standard 4.05: Implementation of Individual Service Plan
(HCS.2012:4.05)
1982
Consumers’ goals and support requirements are met through provision of services.
THE
Attainment and Risk: FA
Evidence:
ACT
Support workers and recovery facilitators are carefully matched with clients around the skills the support worker and recovery facilitators have. This is documented in the
service plans.
Health and safety checks are carried out on site and these were sighted in individual files reviewed. Tasks are well documented. One-on-one training is put in place for any
new support workers for those clients with complex needs. The service managers and service coordinators are responsible for the allocating of support workers and recovery
coordinators and for maintaining records of these allocations. Rosters are managed electronically and a pool of back up support workers or other members of a support team
UNDER
are available for all clients if the regular rostered staff are not available. The use of a buddy system for new staff for more complex clients, ensures relevant tasks are able to
be completed as appropriate for everyone. Communication books are also used as required for support workers to pass on relevant information where several workers are a
part of a team involved in supporting the client.
Advice and assistance from senior staff is available as needed and support workers confirmed this is readily accessed. Support workers and recovery facilitators interviewed
confirmed a good understanding of scopes of practice, limits of responsibility and what to do in an emergency.
Clients reported they felt their support workers and recovery facilitators were well trained and the communication processes in place keeps them informed of any changes in
rostered support during office hours.
The national programme director reported the after-hours service has been reviewed and the technology behind the system has been upgraded. Two customer service
INFORMATION
representatives are now based in Palmerston North and they take calls, solve problems and co-ordinate staff. An RN was expected to join the team on-call during the audit.
The service has been extended and is available seven days a week, 5pm to 9pm. A staff member answers a cell phone from 9pm until the staff member goes to bed.
RELEASED
Following this, clients leave a message.
The national programme director advised a handover period was introduced during this audit. The system is currently being rolled out to branches across the country in a
staged way, so that all branches will eventually be using the same after-hours system. Currently, there is a mix of after hour services across the three service streams using
different after-hours systems. For example, in the Christchurch branch the community service is using the new system, rehabilitation and the mental health services use their
own systems.
For the services using the improved system, the after-hours staff have access to all the client databases across HCNZ. The after-hours service provides a report daily to the
branches of calls and outstanding issues, and a report on Monday morning to summarise the weekends. A summary of all reported events is forwarded to the quality and risk
OFFICIAL
team at the national office for entering in to an electronic system (Promapp). This system differs from the other systems currently in use. For example, in the mental health
service Christchurch, the service is client resolvent based and problems are resolved by the clinical mental health manager for older adults. The service manager advised
they are made aware of after-hours contact and are phoned after hours if needed.
Page 67 of 83
Page 67 of 107
Document 1
Home and Community Support Services Audit Report
Clients and support workers interviewed stated there has been a significant improvement with regards to the after-hour service. Clients stated they no longer must wait in a
queue to have their call answered. Replacement support workers are made available in a timely manner with the support worker being clear about what tasks are expected of
them.
An electronic ‘mapping tool’ linked to rostering has been implemented national y to track travel time between appointments for support workers. Service coordinators can
enter the addresses of clients the support worker is visiting on the day and the programme shows in real time through google maps the route the support worker should take
and the time it takes to travel between appointments. The programme also has alerts in red when there are problems with the route and times require adjusting, so that the
client can be notified of a delay if needed. Clients and support workers reported this has helped with traveling times and stress levels for both clients and support workers.
The findings from the last certification audit in 2017 relating to the after-hours service and travel time has been addressed and is now closed.
Recommendation:
1982
Click here to enter text.
THE
ACT
Criterion 4.05.1 (HCS.2012:4.05.1)
The individual service plan will be delivered by service providers who:
(a) Have been assessed as competent in providing the level and type of care and support;
(b) Clearly recognise and understand their defined role and responsibilities;
(c) Receive an appropriate level of supervision for the level of support they are providing;
UNDER
(d) Know how to seek assistance or advice from their supervisor when the limit of their competency, knowledge, or experience is reached;
(e) Can provide support that meets the needs of the consumer.
Attainment and Risk: FA
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
INFORMATION
Corrective Action:
Click here to enter text.
RELEASED
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
OFFICIAL
Page 68 of 83
Page 68 of 107
Document 1
Home and Community Support Services Audit Report
Criterion 4.05.2 (HCS.2012:4.05.2)
There is a system of recording the allocation of service providers to consumers and for maintaining records of this. This system includes processes for contingency planning
in the event of emergencies or other events which would require changes to scheduled support.
Attainment and Risk: FA
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
1982
Corrective Action:
Click here to enter text.
THE
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
ACT
Criterion 4.05.3 (HCS.2012:4.05.3)
Consumers receive first aid and emergencies are managed in line with the organisation’s policy.
UNDER
Attainment and Risk: FA
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
INFORMATION
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
RELEASED
Standard 4.06: Medicine Management
(HCS.2012:4.06)
Consumers receive medicines in a safe and timely manner that complies with current legislative requirements and safe practice guidelines.
Attainment and Risk: FA
Evidence:
OFFICIAL
The new medication policy has been reviewed by the director of nursing and the national clinical services team and provided to all the branches. Interview of the director of
nursing and review of the policy confirmed this. The policy and framework include self-administration. Responsibilities at each stage of medication management are clear.
Flowcharts for administration include photos and are easy for support workers to understand. An early warning tool, ‘Stop and Watch’ has been designed for support workers
Page 69 of 83
Page 69 of 107
Document 1
Home and Community Support Services Audit Report
to use if they identify any changes while working with a client. The support worker is required to circle the change and send in to their line manager. There is also an ‘Adverse
Medication Reactions Procedure’ that includes response guidelines for mild al ergic reaction or life-threatening anaphylaxis. The requirement from the certification audit in
2017 has been addressed and is now closed.
The medication management competency and training framework procedure has been implemented. The framework is clear and has good guidance for staff to follow. There
are four stages relating to the management of medicines; self-administration, prompting, administration and administration plus. Self-administration is where the person is fully
responsible for the management of their medicines. Prompting is where the person requires reminding, but the support worker does not assist in any way. The support worker
is required to sign the medication sheet. Administration is where the person needs assistance with opening the blister pack, selecting the right dose and time, and assisting
the person to take the medicine. The support worker is required to sign the medicine sheet. Once competent, support workers may administer including, but not limited to,
nasal sprays, ear and eye medicines, tropical ointments and creams. Administration plus is where additional training with an RN is required to demonstrate competency. Staff
who have current competencies can undertake more complex tasks (e.g., oxygen therapy, PEG medication, subcutaneous insulin injections and fentanyl patches).
1982
Training and competency of staff is a ‘work in progress’ and is currently being implemented across the branches (see link to 3.2.3). There was good evidence of signing
sheets being completed fully and returned to the offices at the end of each month. Monitoring and review is undertaken by service coordinators. If there are gaps in the
THE
signing sheet, it is the responsibility of the senior service coordinator to follow up. Review of medicine signing sheets and interview of senior coordinators confirmed this.
Support workers are encouraged to contact the service coordinators and document in the communication book and signing sheet if there are issues around medicine
ACT
management for clients. Any medication errors are entered into an electronic system (Promapp).
The different templates for service plans have a section to record medicine management. Allergies are also documented and the electronic CareCall client management
system has an alert in red (if entered) that appears on the first screen if a client has an allergy to either medication or food.
The service managers, mental health service, reported recovery facilitators are not involved in medicine management. If a client requires some form of medicine support, a
clinical team member from the DHB visits the client and manages this.
UNDER
The Hamilton branch has an RN who has a specialist role relating to medicine oversight. The RN receives referrals from the DHB and MoH for clients including those with
dementia or a disability. The RN visits the client, liaises with the pharmacy and trains support workers to the competency framework. The RN documents in the service plan
under medication actions and is involved in annual reviews. Interview of the RN confirmed this.
Recommendation:
Click here to enter text.
INFORMATION
Criterion 4.06.1 (HCS.2012:4.06.1)
RELEASED
A medicines management system is implemented that complies with legislation, protocols, and safe practice guidelines. The system shall include the detection and
management of all medication errors.
Attainment and Risk: FA
Evidence:
Click here to enter text.
Finding:
OFFICIAL
Click here to enter text.
Page 70 of 83
Page 70 of 107
Document 1
Home and Community Support Services Audit Report
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Criterion 4.06.2 (HCS.2012:4.06.2)
Policies and procedures clearly document the service provider’s responsibilities at each stage of medication management.
Attainment and Risk: FA
1982
Evidence:
Click here to enter text.
THE
Finding:
ACT
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
UNDER
Criterion 4.06.3 (HCS.2012:4.06.3)
Service providers responsible for medicine management are competent to perform the function for each stage they manage.
Attainment and Risk: FA
Evidence:
Click here to enter text.
INFORMATION
Finding:
Click here to enter text.
RELEASED
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
OFFICIAL
Page 71 of 83
Page 71 of 107
Document 1
Home and Community Support Services Audit Report
Criterion 4.06.4 (HCS.2012:4.06.4)
The facilitation of safe self-administration of medicine by consumers where appropriate.
Attainment and Risk: FA
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
1982
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
THE
ACT
Standard 4.07: Infection Prevention and Control
(HCS.2012:4.07)
Consumers and service providers are protected from infection through promotion and implementation of current infection prevention and control practices.
Attainment and Risk: FA
UNDER
Evidence: The Infection, Prevention and Control policy is based on standard precautions and includes guidance on infectious disease management. Information is comprehensive and
includes who the recovery facilitator is to notify, including the service manager and regional infection control coordinator. If an outbreak is suspected, the local public health
unit is notified. Documentation sighted for recovery facilitators includes knowing when a person may have an infection and lists of common infections. Staff support clients to
contact their own GP if a client is suspected of experiencing an infection. The service managers stated recovery facilitators report to the service manager daily over any
issues including those concerned with infection prevention and control.
Currently, the RNs in the branches are utilised should advice be required relating to infections or the clinical services team. The national clinical quality advisor reported that a
job description for regional infection control coordinators is yet to be ratified by the board, and once this has occurred, regional infection control coordinators positions will be
INFORMATION
advertised.
The induction/orientation includes prevention and controlling infections. Recovery facilitators have attained a relevant level 4 NZQA qualification and have competed on-going
RELEASED
training and have current competencies in both the Hamilton and Tauranga branches. Recovery facilitators and review of records confirmed this. The recovery facilitators in
the Christchurch branch have not received on-going education in the last 12 months.
The finding from the mental health certification audit of 2016 is now included in 3.2.2.
Recommendation:
Click here to enter text.
OFFICIAL
Page 72 of 83
Page 72 of 107
Document 1
Home and Community Support Services Audit Report
Criterion 4.07.1 (HCS.2012:4.07.1)
Policies and procedures exist to support current infection prevention and control practices. Policies and procedures shall cover the:
(a) Identification and reporting of notifiable diseases;
(b) Management of common infectious diseases;
(c) Appointment of an infection prevention and control officer.
Attainment and Risk: FA
Evidence:
Click here to enter text.
Finding:
1982
Click here to enter text.
THE
Corrective Action:
Click here to enter text.
ACT
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Criterion 4.07.2 (HCS.2012:4.07.2)
UNDER
Each service provider is competent in current infection prevention and control practice. This shall include:
(a) Use and knowledge of personal protection equipment;
(b) Use and knowledge of cleaning and disposal techniques;
(c) Knowledge of signs and symptoms of common infectious diseases;
(d) Use and knowledge of basic infection prevention and control practices.
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
INFORMATION
Finding:
Click here to enter text.
RELEASED
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
OFFICIAL
Page 73 of 83
Page 73 of 107
Document 1
Home and Community Support Services Audit Report
Standard 4.08: Equipment, Aids and Enablers
(HCS.2012:4.08)
Consumers are supported to safely use any required or prescribed equipment, aids, or enablers.
Attainment and Risk: Not Audited
Evidence: Click here to enter text.
Recommendation:
Click here to enter text.
1982
THE
Criterion 4.08.1 (HCS.2012:4.08.1)
ACT
Consumer-specific information and training is made available to service providers in the use of equipment, aids, and enablers, including definitions and descriptions of each.
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
UNDER
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
INFORMATION
Criterion 4.08.2 (HCS.2012:4.08.2)
All equipment, aids, and enablers are used safely and as required or prescribed to support the consumer to maintain their independence, dignity and respect.
RELEASED
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
OFFICIAL
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Page 74 of 83
Page 74 of 107
Document 1
Home and Community Support Services Audit Report
Standard 4.09: Nutrition and Safe Food Management
(HCS.2012:4.09)
The consumer’s nutrition and hydration is supported by service delivery.
Attainment and Risk: Not Audited
Evidence: Click here to enter text.
1982
Recommendation:
Click here to enter text.
THE
ACT
Criterion 4.09.1 (HCS.2012:4.09.1)
Consumers are monitored for signs and symptoms of dehydration and malnutrition and interventions implemented as needed.
Attainment and Risk: Not Audited
UNDER
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
INFORMATION
RELEASED
Criterion 4.09.2 (HCS.2012:4.09.2)
Consumers who require special or modified diets are supported to meet these needs.
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
OFFICIAL
Finding:
Click here to enter text.
Page 75 of 83
Page 75 of 107
Document 1
Home and Community Support Services Audit Report
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Criterion 4.09.3 (HCS.2012:4.09.3)
Consumers with enteral feeding tubes have their needs met by service providers with specific training and demonstrated competencies.
Attainment and Risk: Not Audited
1982
Evidence:
Click here to enter text.
THE
Finding:
ACT
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
UNDER
Criterion 4.09.4 (HCS.2012:4.09.4)
Consumers are safe from disease caused by unsafe food storage and preparation. Service providers are oriented to safe food-handling practices.
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
INFORMATION
Finding:
Click here to enter text.
RELEASED
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
OFFICIAL
Page 76 of 83
Page 76 of 107
Document 1
Home and Community Support Services Audit Report
Standard 4.10: Skin Integrity
(HCS.2012:4.10)
Consumers’ skin integrity is maintained.
Attainment and Risk: Not Audited
Evidence: Click here to enter text.
Recommendation:
Click here to enter text.
1982
THE
Criterion 4.10.1 (HCS.2012:4.10.1)
ACT
Consumers are monitored for signs of skin breakdown.
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
UNDER
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
INFORMATION
Criterion 4.10.2 (HCS.2012:4.10.2)
Service providers implement preventive measures to promote skin integrity.
RELEASED
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
OFFICIAL
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Page 77 of 83
Page 77 of 107
Document 1
Home and Community Support Services Audit Report
Standard 4.11: Review of Service Delivery
(HCS.2012:4.11)
Consumers are supported to achieve their goals through regular monitoring and review of service delivery.
Attainment and Risk: PA Moderate
Evidence: There was evidence of progress in all branches visited around reducing the numbers of reviews that are overdue. The three service streams have different requirements
1982
relating to review timeframes and how the reviews are documented.
Three monthly reviews are completed with the clients using the mental health service branches and include a case manager from the DHB mental health clinical team in the
THE
Hamilton and Tauranga branches. The service manager Christchurch branch advised there is no requirement to report to the DHB under the current contract. Review of the
clients’ files evidenced regular monitoring and reviews. The electronic programme also provides useful percentages and graphs showing progress towards meeting the
client’s goals.
ACT
A ‘client experience survey’ is completed annually for the mental health service and the last one was in June/July 2018. Feedback is also sought from the case managers
from the DHB mental health clinical team. Collated results showed high satisfaction with the service, however, corrective actions identified have not been developed and
implemented. (See link 2.3.5) The finding from the 2016 mental health service certification audit is closed.
Clients using the rehabilitation service have different timeframes for reviews depending on the length of time using the service and the complexity. Reports are completed and
UNDER
sent to ACC. The reports are comprehensive and showed detailed progress. An exception report is generated when goals are not able to be achieved. Not all annual reviews
of service plan goals in the branches visited were up to date. Not all reviews reflected the degree of achievement towards meeting the goals.
The community service uses a client management system (‘Caduceus’), apart from the Tauranga and Christchurch branches who currently use a different one (Goldcare).
Clients who are not under ACC receive phone reviews at set intervals and this is facilitated by the service coordinators. An annual review of the client’s goals is required to be
completed at the client’s home. Reviews were often a tick in a box with no narrative or a new service plan completed with different goals.
The services in each branch had evidence of a ‘bring-up’ system that shows what clients are due/overdue for reviews.
If there is a change in need identified, a new service plan is completed. Support workers confirmed they alert the office if they note any changes or an increase in needs. If
this does occur, a visit is made and changes required are responded to.
INFORMATION
Recommendation:
RELEASED
Click here to enter text.
Criterion 4.11.1 (HCS.2012:4.11.1)
To keep individual service plans up-to-date, service delivery is reviewed:
(a) Regularly, relative to the complexity of the consumer’s support needs and risks;
OFFICIAL
Page 78 of 83
Page 78 of 107
Document 1
Home and Community Support Services Audit Report
(b) At the request of the consumer; or
(c) If a change in need occurs.
Attainment and Risk: FA
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
1982
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
THE
ACT
Criterion 4.11.2 (HCS.2012:4.11.2)
Reviews are documented, consumer focused, indicate the degree of achievement or response to the support and progress towards meeting the consumer’s goals.
Attainment and Risk: PA Moderate
UNDER
Evidence:
Progress with reviewing overdue client’s goals is a focus at al the branches visited and review of the registers evidenced in-roads are being made in some branches.
In the mental health service, review of the client management system (Recordbase) evidenced regular monitoring and reviews. This electronic programme also has the
capability of producing a percentage, so that recovery facilitators can see how far the client has progressed to meeting their goals. The programme also generates graphs
which show progress.
In the rehabilitation service a ‘progress/exception/completion’ report is completed and provided to ACC. The reports are comprehensive and show detailed progress towards
meeting the goals. An exception report is generated when goals are not able to be achieved. Long term clients have a different process whereby if there are concerns raised,
a multidisciplinary meeting with ACC, client and family is held. Reviews are completed every 26 weeks and the service and support plans are updated. The reviews are
scanned into the client management system (CareCall). There was a mix of entries for reviews including ‘on going’ and ‘no change’ rather than documenting progress. (See
INFORMATION
also 4.11.4)
RELEASED
The community service uses a client management system (‘Caduceus’), apart from the Tauranga and Christchurch branches who currently use a different one (Goldcare).
Clients who are not under ACC have phone reviews at three weeks and six weeks and this is facilitated by the service coordinators. An annual review of the client’s goals is
completed at the client’s home. The Hamilton branch reviews had been completed apart from one from 2016, however, there remains inconsistency across the branches. The
template for the community service plan reviews does not encourage service coordinators to document progress towards meeting the client’s goals. A ‘tick box’ in the service
plan template has three levels to note the level of progress made and this was not completed in a significant number of service plans reviewed. Where it had been completed,
there was always commentary to indicate progress or any changes or if the goals needed updating. In some instances, a new service plan had been completed with totally
different goals.
OFFICIAL
The finding from the certification audit of 2017 remains open.
Finding:
Although progress has been made, reviews of goals in the rehabilitation and community services do not consistently indicate the progress towards meeting the client’s goals.
Page 79 of 83
Page 79 of 107
Document 1
Home and Community Support Services Audit Report
Corrective Action:
Ensure service plan reviews are documented, client focused and indicate the progress towards meeting the client’s goals.
Timeframe (days): 180
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Criterion 4.11.3 (HCS.2012:4.11.3)
Feedback from family/whānau and other providers is sought as part of the input for the review, where appropriate.
Attainment and Risk: FA
1982
Evidence:
Click here to enter text.
THE
Finding:
ACT
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
UNDER
Criterion 4.11.4 (HCS.2012:4.11.4)
There is formal evidence of a review occurring in line with the organisation’s policy.
Attainment and Risk: PA Moderate
Evidence:
The mental health service completes three monthly reviews with the client, their family and may involve other service providers if appropriate. The reviews are attended by the
INFORMATION
case manager from the DHB mental health clinical team. Review of the client management system (Recordbase) evidenced regular monitoring and reviews. The finding from
the 2016 certification audit is now closed.
RELEASED
The rehabilitation service completes reviews at least six monthly and the support plans annually. The reviews are scanned into the client management system (CareCall). Not
all reviews in the branches visited are up to date.
The community service uses a client management system (‘Caduceus’), apart from the Tauranga and Christchurch branches who currently use (Goldcare). Clients who are
not under ACC have phone reviews at three weeks and six weeks and this is facilitated by the service coordinators. An annual review of the client’s goals is completed at the
client’s home. There are significant numbers of reviews that are not current. The Hamilton branch annual reviews had been completed apart from one from 2016. (See link to
4.11.2).
The finding from the mental health certification audit of 2016 is closed, however the finding from the Certification audit of 2017 remains open.
OFFICIAL
Finding:
Apart from the mental health service, not all reviews meet the required timeframes in the rehabilitation and community services.
Page 80 of 83
Page 80 of 107
Document 1
Home and Community Support Services Audit Report
Corrective Action:
Complete overdue reviews in the rehabilitation and the community services.
Timeframe (days): 180
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Criterion 4.11.5 (HCS.2012:4.11.5)
Where progress is different to that expected, the service provider responds by initiating changes to the individual service plan.
Attainment and Risk: FA
1982
Evidence:
Click here to enter text.
THE
Finding:
ACT
Click here to enter text.
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
UNDER
Standard 4.12: Challenging Behaviours
(HCS.2012:4.12)
Consumers with behaviours that challenge are treated with respect and receive services in a manner that has regard for their safety, dignity, privacy, and independence.
Attainment and Risk: FA
Evidence: The policy and procedures related to the prevention, minimisation and management of challenging behaviours meet the requirements of the standard. A process for
INFORMATION
identification, documentation and referral for specialist input is used when required. Any specialist behavioural management plans are included in the individual’s service plan.
A fact sheet for recovery facilitators gives good guidance on managing challenging behaviour. If a client enters the mental health service with challenging behaviour, a risk
RELEASED
management plan is developed. A ‘How to Guide’ has a section on challenging behaviour and includes who to contact re escalation. Event notes concerning challenging
behaviours evidenced updating of the service plan.
Recovery facilitators in the Hamilton branch were last provided with management of actual or potential aggression (MAPA) training February 2019 and the Tauranga branch in
April 2019. Interview of recovery facilitators and review of training records confirmed this. The service manager from the Christchurch branch reported the recovery facilitators
have not been provided with any training relating to challenging behaviour. The service manager advised because of the age group is over 65 years, this has not presented
as an issue. If it was, a risk management plan would be developed. (See link to 3.2.2).
OFFICIAL
The finding from the last mental health certification audit in 2016 is now closed.
Recommendation:
Click here to enter text.
Page 81 of 83
Page 81 of 107
Document 1
Home and Community Support Services Audit Report
Criterion 4.12.1 (HCS.2012:4.12.1)
Policies and procedures exist to support consumers with challenging behaviours to ensure their safety, dignity, privacy, and independence are maintained. Policies and
procedures shall cover:
(a) Initiation of appropriate assessment of the consumer to determine the presence and nature of any challenging behaviours;
(b) Identification and documentation within the individual service plan of support required in the home and/or in community environments;
(c) Documentation of behaviours in the individual service plan;
1982
(d) Reporting protocols;
(e) Escalation protocol if behaviours present an immediate threat to the client, service provider, or others;
(f) Management of any deterioration in behaviour including protocols for initiating specialist intervention services.
THE
Attainment and Risk: FA
ACT
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
UNDER
Corrective Action:
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Criterion 4.12.2 (HCS.2012:4.12.2)
Consumers with behaviours that challenge are supported by suitably trained and competent service providers.
INFORMATION
Attainment and Risk: Not Audited
RELEASED
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
Click here to enter text.
OFFICIAL
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
Page 82 of 83
Page 82 of 107
Document 1
Home and Community Support Services Audit Report
Criterion 4.12.3 (HCS.2012:4.12.3)
Service providers working with consumers with behaviours that challenge receive adequate and appropriate supervision.
Attainment and Risk: Not Audited
Evidence:
Click here to enter text.
Finding:
Click here to enter text.
Corrective Action:
1982
Click here to enter text.
Timeframe (days): Choose an item.
(e.g. for 1 week choose 7, for 1 month choose 30, for 6 months choose 180, etc.)
THE
ACT
UNDER
INFORMATION
RELEASED
OFFICIAL
Page 83 of 83
Page 83 of 107

Document 2
+, FNY\NVKNZ +)+)
9Z 6[QUNa 7UXXVORNUM
9RZNL\XZ'=NWNZJU XO >NJU\Q
@RWR[\Za XO >NJU\Q
7a NVJRU3 J[QUNa(KUXXVORNUM5QNJU\Q(PX^\(Wb
2]yU vz\ 9Z 7UXXVORNUM
1982
-CAD@6?BG*
0;6@G>-6E; 3;I 5;6@6B9
THE
4HE E;<*
/'%0.-%&()&$,1,
ACT
HN QJ^N ZNLNW\Ua ZNLNR^NM J W]VKNZ XO LXVYUJRW\[ ZJR[RWP LXWLNZW[ JKX]\ >NJU\Q8JZN
AN_ INJUJWM $>8AI%(
6\ \QN \RVN XO _ZR\RWP& \QNZN QJ^N KNNW */ LXVYUJRW\[ ZNLNR^NM [RWLN * <NKZ]JZa +)+)&
_R\Q QJUO XO \QN[N ZNLNR^NM JO\NZ * 6]P][\ +)+)(
UNDER
6W JWXWaVR[NM \JKUN []VVJZR[RWP \QN LXVYUJRW\[ _R\Q \QR[ BOORLN R[ ;B8@CF;9 OXZ aX]Z
RWOXZVJ\RXW( ? WX\N \QJ\ OX]Z XO \QN[N LXVYUJRW\[ RW^XU^N LJZN YZX^RMNM RW \QN
+TyTT'HQJWPJW]R ZNPRXW& _R\Q \QZNN RW \QN 7Ja XO CUNW\a JWM 8JW\NZK]Za ZNPRXW[
ZN[YNL\R^NUa( ?W JMMR\RXW& \QNZN JZN OR^N XYNW LXVYUJRW\[ _QRLQ _N JZN RW \QN YZXLN[[
XO J[[N[[RWP(
INFORMATION
<XZ [XVN XO \QN[N LXVYUJRW\[& _N QJ^N WX\ KNNW JKUN \X RMNW\ROa _QN\QNZ \QNa ZNUJ\N
\X [NZ^RLN[ O]WMNM Ka \QN @RWR[\Za XO >NJU\Q& \QN ZNUN^JW\ 9R[\ZRL\ >NJU\Q 7XJZM $9>7%
RELEASED
XZ 6LLRMNW\ 8XVYNW[J\RXW 8XZYXZJ\RXW $688%( GQNZNOXZN& _N QJ^N JU[X YZX^RMNM JW
JWXWaVR[NM []VVJZa XO \QN[N LXVYUJRW\[ \X KX\Q 688 JWM \QN ZNUN^JW\ 9>7[& J[ \QN
X\QNZ VJSXZ O]WMNZ[ XO [NZ^RLN[ YZX^RMNM Ka >8AI( ?O aX] JYYZXJLQ X]Z BOORLN& _N _RUU
NWMNJ^X]Z \X _XZT _R\Q aX] \X RMNW\ROa \QN LXVYUJRW\[ \QJ\ ZNUJ\N \X \QN [NZ^RLN[ aX]
O]WM(
OFFICIAL
?W JMMR\RXW \X \QN LXVYUJRW\[ ZNLNR^NM Ka \QR[ BOORLN& _N QJ^N ZNLNW\Ua ZNLNR^NM J
WX\RORLJ\RXW OZXV \QN AJ\RXW_RMN >NJU\Q JWM 9R[JKRUR\a 6M^XLJLa FNZ^RLN JKX]\ J
W]VKNZ XO X\QNZ LXVYUJRW\[ ZNLNR^NM Ka \QJ\ [NZ^RLN( HN JZN RW \QN YZXLN[[ XO
J[[N[[RWP \QR[ RWOXZVJ\RXW(
6]LTUJWM BOORLN3 CB 7X` *02*& 6]LTUJWM **-)4 HNUURWP\XW BOORLN3 CB 7X` **2,-& HNUURWP\XW /*-+
<ZNNYQXWN3 )1)) ** ++ ,,4 ;VJRU3 QML5QML(XZP(Wb4 HNK[R\N3 ___(QML(XZP(Wb
Page 84 of 107


Document 2
+
GQN L]ZZNW\ LXVYUJRW\ JL\R^R\a R[ XO LXWLNZW WX\ UNJ[\ XW JLLX]W\ XO \QN ZNUJ\R^N
W]VKNZ RW^XU^NM K]\ JU[X RW URPQ\ XO \QN YJZ\RL]UJZUa ^]UWNZJKUN LXW[]VNZ PZX]Y[
ZNLNR^RWP LXVV]WR\a []YYXZ\ [NZ^RLN[(
GQN VJRW LXWLNZW[ ZJR[NM [RWLN <NKZ]JZa +)+) JZN XO J [RVRUJZ WJ\]ZN JWM VJRWUa ZNUJ\N
\X3
'
8XVV]WRLJ\RXW _R\Q \QN LJUU LNW\ZN& RWLU]MRWP ZN[YXW[N \RVN[ \X LJUU[
RVYJL\RWP XW \QN \RVNURWN[[ XO MNUR^NZa XO LJZN4
'
?WLXW[R[\NWLa RW \QN [NZ^RLN LXXZMRWJ\RXW JWM YZX^R[RXW XO LJZNZ[& RWLU]MRWP
LJZNZ[ WX\ J\\NWMRWP \X XOONZ LJZN[ J\ N`YNL\NM \RVN[ XZ& RW [XVN RW[\JWLN[& WX\
J\ JUU4 JWM
'
D]JUR\a XO [NZ^RLN[ YZX^RMNM& RWLU]MRWP \ZJRWRWP JWM LXWM]L\ XO [\JOO(
?W URPQ\ XO \QN ^XU]VN XO LXVYUJRW\[ JWM \QN ZNL]ZZRWP \QNVN[& ? QJ^N MNLRMNM \QJ\ R\ R[
MN[RZJKUN RW \QN Y]KURL RW\NZN[\ \X ZNONZ \QN[N LXVYUJRW\[ JWM \QN R[[]N[ \QNa ZJR[N \X
1982
\QN @RWR[\Za XO >NJU\Q OXZ R\[ LXW[RMNZJ\RXW( GQR[ ZNONZZJU R[ VJMN RW JLLXZMJWLN _R\Q
THE
[NL\RXW .2$-% XO \QN >NJU\Q JWM 9R[JKRUR\a 8XVVR[[RXWNZ 6L\ *22-(
ACT
? _RUU UNJ^N \QN @RWR[\Za XO >NJU\Q \X MN\NZVRWN _QJ\ JL\RXW& RO JWa& R[ \JTNW RW \QR[
RW[\JWLN K]\ _X]UM JYYZNLRJ\N KNRWP JM^R[NM XO \QN X]\LXVN XO \QR[ ZNONZZJU(
8XZZN[YXWMNWLN [QX]UM KN [NW\ \X >98E;FDCBF;F+>98#CE=#BK (
UNDER
>98 R[ LXW\RW]RWP \X J[[N[[ R\[ XYNW LXVYUJRW\[ JWM \QN L]V]UJ\R^N LXWLNZW[ ZJR[NM
JKX]\ >NJU\Q8JZN AI#[ [NZ^RLN[& JWM ? _RUU TNNY aX] JKZNJ[\ XO JWa O]Z\QNZ
MN^NUXYVNW\[ RW M]N LX]Z[N( ? \QJWT aX] OXZ aX]Z J[[R[\JWLN RW \QN VNJW\RVN(
,Uv qq yzT® yU
INFORMATION
RELEASED
EX[N HJUU
.;DHGJ 0;6@G> 6B9 .?F67?@?GJ -CAA?FF?CB;E
;WL
GJKUN XO JWXWaVR[NM LXVYUJRW\[
OFFICIAL
8XYa LXZZN[YXWMNWLN \X >8AI
LL
>8AI
Page 85 of 107
Document 2
Complaint Complaint
Date
Region
Type of care
Concerns raised
Stage
no.
Reference and
received
Name
1
s 9(2)(a)
13
Wel ington
ACC funded for
Support person not showing up or showing up on
Provider referral.
February
injury
incorrect days/times. Support person not adequately
2020
trained.
1982
2
19
Bay of
High needs
Concerns about changes to call centre which result in
S38(1) – no
THE
February
Plenty
disability
delay in clients accessing care.
action.
2020
ACT
3
3 March
Canterbury Unclear
Support worker not showing up. Ongoing issues.
Provider Referral
2020
UNDER
4
11 March
Wel ington
High needs
Diet changed without agreement. Alleges staff are
Formal referral to
2020
disability
bul ying him.
Advocacy
5
25 March
Bay of
High needs
Home help services discontinued with insufficient
S38(1) – no
2020
Plenty
disability
warning during COVID-19/coronavirus lockdown.
action.
6
12 May
Canterbury Aged care-
Medication administration error on three separate
Reviewing further
INFORMATION
2020
home help
occasions.
information.
RELEASED
7
17 June
Manawatū- Unclear
Concerns about new call centre system. Cannot get
Provider Referral.
2020
Whanganui
through to change carer times. Carers are often late as
they do not allow travel time between clients.
OFFICIAL
Page 86 of 107
Document 2
8
s 9(2)(a)
23 June
Otago
High needs
Difficulty accessing carers. Sent many different carers –
Reviewing further
2020
disability
too young, inappropriate, leave shortly after they start.
information.
Inconsistency of care.
9
3 August
Manawatū- Aged care –
Medication administration errors. Carers not turning up.
Awaiting further
2020
Whanganui home help
HCNZ give no notice when carers are not available.
information.
1982
10
3 August
Manawatū- Unclear
Consumer not had support worker turn up for 3 weeks,
Formal Referral
2020
Whanganui
despite calling HCNZ.
to Advocacy.
THE
11
10 August
Hawke’s
ACC funded for
Four occasions over short period of time where carer has
Formal Referral
ACT
2020
Bay
injury
not turned up.
to Advocacy.
12
10 August
Manawatū High needs
Lack of coordination of care. His carer provided advanced Formal Referral
2020
Whanganui disability
notice of his lack of availability on a particular date, but
to Advocacy.
HCNZ failed to arrange a replacement. Consumer soiled
UNDER
himself and sat in dirty clothing al night.
13
13 August
Waikato
Aged care –
Reports that HCNZ has centralised communication with
Provider referral.
2020
residential
call centre in Auckland and she does not have a
service
coordinator appointed at present to contact to make
changes.
14
24 August
Nelson
ACC funded for
Reports sexual harassment/abuse, threats and
Formal Referral
2020
injury
inappropriate/rude communication with staff member(s), to Advocacy.
INFORMATION
a lack of available staff on afternoon shifts and record-
keeping.
RELEASED
15
31 August
Bay of
Aged care –
Reports that the quality of care has declined since HCNZ’s
Obtaining further
2020
Plenty
retirement
recent reorganisation. Concerns she no longer receives a
information.
vil age
roster informing her of when cares will be undertaken and
by whom. Detailed an instance of a worker not showing
up and one where two carers showed up due to
OFFICIAL
Page 87 of 107
Document 2
miscommunication by HCNZ.
16
s 9(2)(a)
1
Canterbury Aged care –
Concerns of a threatening comment made to the
Obtaining further
September
retirement
complainant and she ended up falling, which had not
information.
2020
vil age
been reported. Reported difficulty with getting hold of
provider on the phone.
1982
THE
ACT
UNDER
INFORMATION
RELEASED
OFFICIAL
Page 88 of 107

Document 2
+, ENX[NUKNY +)+)
GJVNZZJ 9\MTN`
8QRNO ;_NL\[R]N AOORLNY $8;A%
=NJT[Q8JYN @N^ INJTJVM
s 9(2)(a)
1\sT pt[ ?Z 9\MTN`
-?BF<CH)
.84=E;+4C8 18G 384=4?7 6@>A=4<?ED
2FC C89)
-&$.,+$%'(%#*/*
1982
THE
HN QJ]N YNLNV[T` YNLNR]NM J V\UKNY WO LWUXTJRV[Z YJRZRVP LWVLNYVZ JKW\[ `W\Y WYPJVRZJ[RWV(
ACT
6[ [QN [RUN WO ^YR[RVP& [QRZ AOORLN QJZ YNLNR]NM */ LWUXTJRV[Z ZRVLN * <NKY\JY` +)+)& ^R[Q QJTO WO
[QNZN YNLNR]NM JO[NY * 6\P\Z[ +)+)( 6 [JKTN Z\UUJYRZRVP [QN LWUXTJRV[Z ^R[Q [QRZ AOORLN RZ
8?6=@D87 OWY `W\Y RVOWYUJ[RWV( > VW[N [QJ[ OW\Y RV]WT]N LJYN XYW]RMNM RV [QN
'HQJVPJV\R
YNPRWV& ^R[Q [QYNN RV [QN 7J` WO BTNV[` JVM 8JV[NYK\Y` YNPRWVZ YNZXNL[R]NT`( >V JMMR[RWV& [QNYN JYN
UNDER
OR]N LWUXTJRV[Z ^N JYN RV [QN XYWLNZZ WO JZZNZZZRVP(
>V JMMR[RWV& ^N QJ]N YNLNV[T` YNLNR]NM J VW[RORLJ[RWV OYWU [QN @J[RWV^RMN =NJT[Q JVM 9RZJKRTR[`
6M]WLJL` ENY]RLN JKW\[ J V\UKNY WO W[QNY LWUXTJRV[Z YNLNR]NM K` [QJ[ ZNY]RLN( HN JYN RV [QN XYWLNZZ
WO JZZNZZRVP [QRZ RVOWYUJ[RWV(
FQN L\YYNV[ LWUXTJRV[ JL[R]R[` RZ WO LWVLNYV VW[ TNJZ[ WV JLLW\V[ WO [QN YNTJ[R]N V\UKNY RV]WT]NM K\[
JTZW RV TRPQ[ WO [QN XJY[RL\TJYT` ]\TVNYJKTN LWVZ\UNY PYW\XZ YNLNR]RVP LWUU\VR[` Z\XXWY[ ZNY]RLNZ(
INFORMATION
FQN UJRV LWVLNYVZ YJRZNM ZRVLN <NKY\JY` +)+) JYN WO J ZRURTJY VJ[\YN JVM VJUNT` YNTJ[N [W3
RELEASED
'
8WUU\VRLJ[RWV ^R[Q [QN LJTT LNV[YN& RVLT\MRVP YNZXWVZN [RUNZ [W LJTTZ RUXJL[RVP WV [QN
[RUNTRVNZZ WO MNTR]NY` WO LJYN4
'
>VLWVZRZ[NVL` RV [QN ZNY]RLN LWWYMRVJ[RWV JVM XYW]RZRWV WO LJYNYZ& RVLT\MRVP LJYNYZ VW[
J[[NVMRVP [W WOONY LJYNZ J[ N_XNL[NM [RUNZ WY& RV ZWUN RVZ[JVLNZ& VW[ J[ JTT4 JVM
'
C\JTR[` WO ZNY]RLNZ XYW]RMNM& RVLT\MRVP [YJRVRVP JVM LWVM\L[ WO Z[JOO(
OFFICIAL
>V TRPQ[ WO [QN ]WT\UN WO LWUXTJRV[Z JVM [QN YNL\YYRVP [QNUNZ& > QJ]N MNLRMNM [QJ[ R[ RZ MNZRYJKTN RV [QN
X\KTRL RV[NYNZ[ [W YNONY [QNZN LWUXTJRV[Z JVM [QN RZZ\NZ [QN` YJRZN [W 688& [QN YNTN]JV[ 9RZ[YRL[ =NJT[Q
7WJYMZ JVM [QN ?RVRZ[Y` WO =NJT[Q(
6\LSTJVM AOORLN3 BA 7W_ *02*& 6\LSTJVM **-)4 HNTTRVP[WV AOORLN3 BA 7W_ **2,-& HNTTRVP[WV /*-+
<YNNXQWVN3 )1)) ** ++ ,,4 ;UJRT3 QML5QML(WYP(Va4 HNKZR[N3 ^^^(QML(WYP(Va
Page 89 of 107


Document 2
+
BTNJZN VW[N [QJ[ [QRZ YNONYYJT RVLT\MNZ [QN OR]N LWUXTJRV[Z [QJ[ YNUJRV WXNV ^R[Q [QRZ AOORLN JVM RZ
UJMN RV JLLWYMJVLN ^R[Q ZNL[RWV .2$-% WO [QN =NJT[Q JVM 9RZJKRTR[` 8WUURZZRWVNY 6L[ *22-(
+Tp• nyn stS§ sT
DWZN HJTT
,8AFEH .84=E; 4?7 ,<D45<=<EH +@>><DD<@?8C
;VL
FJKTN WO LWUXTJRV[Z
8L
s 9(2)(a)
?RVRZ[Y` WO =NJT[Q& 688& JVM DNTN]JV[ 9=7
1982
THE
ACT
UNDER
INFORMATION
RELEASED
OFFICIAL
Page 90 of 107
Document 3
1982
THE
ACT
UNDER
INFORMATION
RELEASED
OFFICIAL
Page 91 of 107
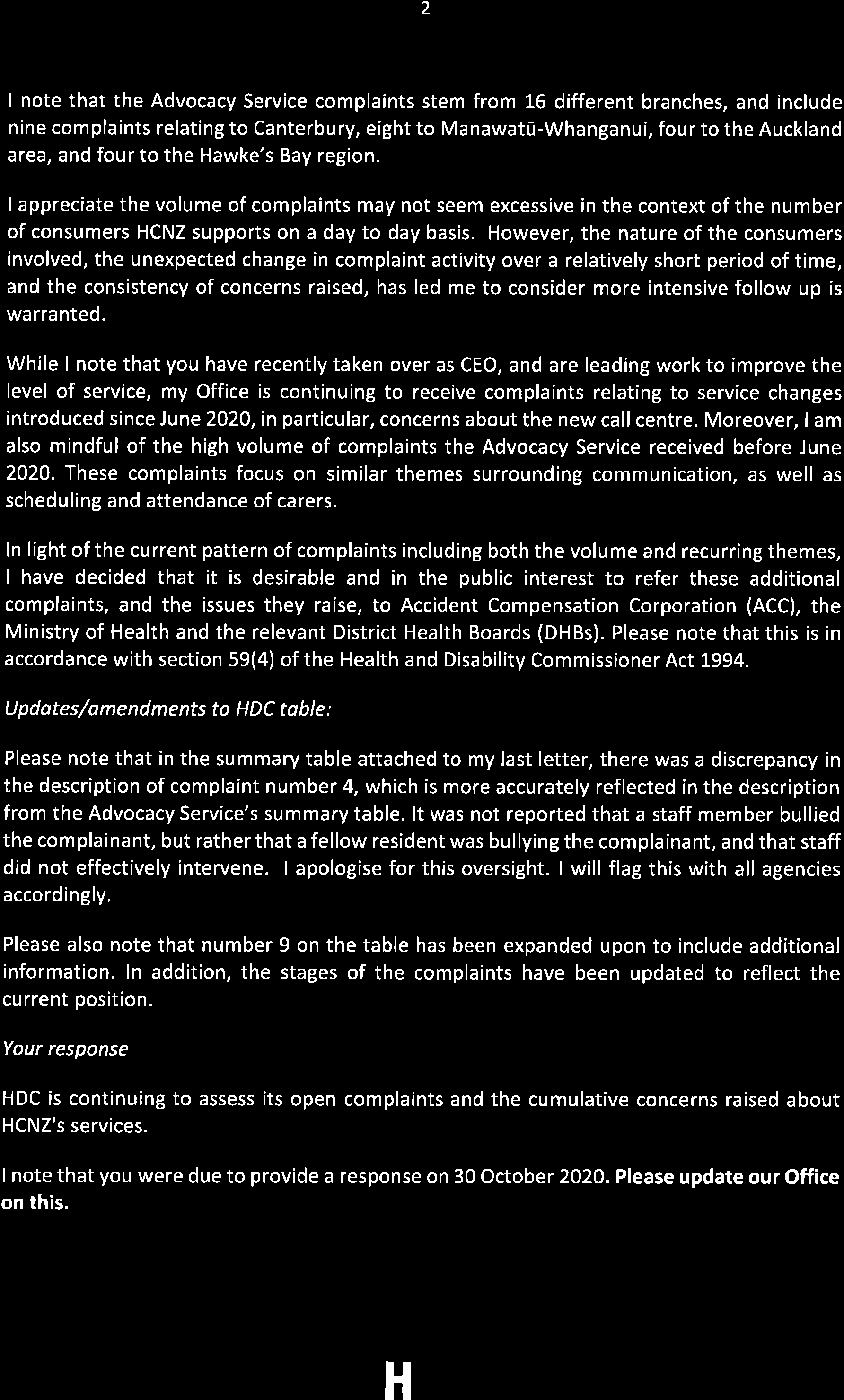
Document 3
1982
THE
ACT
UNDER
INFORMATION
RELEASED
OFFICIAL
Page 92 of 107
Document 3
1982
THE
ACT
UNDER
INFORMATION
RELEASED
OFFICIAL
Page 93 of 107

Document 4
6 November 2020
Dr Ashley Bloomfield
Director-General of Health
Ministry of Health
By email:
[email address]
Tēnā koe Dr Bloomfield
1982
Complaint: HealthCare New Zealand (HCNZ)
Our ref:
E20HDC01461/AKA
THE
I write further to my letter of 23 September 2020, and your response of 16 October 2020.
ACT
Since I wrote to you on 23 September 2020, this Office has received a further six complaints
about HCNZ’s service (see the
enclosed updated table). In addition, the Nationwide Health
and Disability Advocacy Service (Advocacy Service) has reported concerns about HCNZ to this
UNDER
Office. This information was provided under section 30(k) of the Health and Disability
Commissioner Act 1994.
The report from the Advocacy Service refers to 34 complaints the service has received about
HCNZ from across the country, since September 2019. The second report contains 11
complaints. I
enclose a summary table of these complaints for your information. Please note
that you have been notified of six of these complaints previously. For ease of reference, I have
set out the duplications for you below (the column on the left is the Advocacy complaint
INFORMATION
number that corresponds to the HDC complaint number in the right hand column):
RELEASED
Complaint number in table
Advocacy
HDC
15
4
22
6
31
16
OFFICIAL
33
11
35
14
37
10
I note that the Advocacy complaints stem from 16 different branches, and include nine
complaints relating to Canterbury, eight to Manawatū-Whanganui, four to the Auckland area,
and four to the Hawke’s Bay region.
Auckland Office: PO Box 1791, Auckland 1140; Wel ington Office: PO Box 11934, Wel ington 6142
Freephone: 0800 11 22 33; Email:
[email address]; Website
: www.hdc.org.nz
Page 94 of 107


Document 4
2
My Office is continuing to receive complaints relating to the service changes introduced since
June 2020, in particular, concerns about the new call centre. Moreover, I am also mindful
about the high volume of complaints the Advocacy Service received before June 2020. These
complaints focus on similar themes surrounding communication, as well as scheduling and
attendance of carers.
While I note that you are looking into these issues, and wil be fol owing up with HCNZ, ACC
and the relevant District Health Boards (DHBs), I wished to ensure that you had a fuller picture
of the issues my Office is assessing.
In light of the current pattern of complaints including both the volume and recurring themes,
I have decided that it is desirable and in the public interest to refer these additional
complaints, and the issues they raise to, Accident Compensation Corporation (ACC) and the
relevant DHBs. Please note that this is in accordance with section 59(4) of the Health and
1982
Disability Commissioner Act 1994.
THE
Updates/amendments to HDC table:
ACT
Please note that in the summary table attached to my last letter, there was a discrepancy in
the description of complaint number 4, which is more accurately reflected in the description
from the Advocacy Service’s summary table. It was not reported that a staff member bullied
the complainant, but rather that a fellow resident was bullying the complainant, and that staff
did not effectively intervene.
UNDER
Please also note that number 9 on the table has been expanded upon to include additional
information. In addition, the stages of the complaints have been updated to reflect the
current position.
Your response:
HDC is continuing to assess its open complaints and the cumulative concerns raised about
INFORMATION
HCNZ's services. I appreciate that the healthy ageing team will report back to this Office once
it receives a response from the above organisations. Correspondence should be sent to
RELEASED
[email address]. I will keep you abreast of any further developments at my Office.
I look forward to hearing from your team again in due course.
Nāku iti noa, nā
OFFICIAL
Rose Wall
Deputy Health and Disability Commissioner
Enc Updated table of complaints from HDC
Summary table of complaints from Advocacy
Copy letter to HCNZ
Cc
HCNZ
Page 95 of 107
Document 5
ADVOCACY SERVICE
Complaint Complaint Reference
Date Received
Region
Concerns raised
Stage
No.
And Name
1
s 9(2)(a)
16 September
Taranaki
Relief carer did not wash consumer
Resolved – provider got a new
2019
properly
coordinator, two new trained
Relief staff often unavailable to cover or carers and updates Mr Muir’s
help main caregiver
care plan.
Manner and communication from
coordinator
2
23 September
Manawatū-
Lack of communication with family
Withdrawn from Advocacy.
1982
2019
Whanganui
Inadequate care – consumer was unwell
and no one had put a pull up on her
OPEN at HDC (19/02265) –
THE
Inadequate care – consumer became
drafting s 38 provisional
increasingly unwell. Ended in hospital
ACT
coronary care unit.
3
26 September
Canterbury
Lack of communication about reduced
Not resolved – didn’t wish to
2019
care
engage further with provider.
Inadequate response to complaint
Closed with Advocacy.
UNDER
4
25 October 2019
Manawatū-
Mistreated by carers
Resolved – Advocacy liaised with
Whanganui
Disrespected and patronised by care
support funder to move
staff
consumer to a new flat
Lack of support to find paid
employment
5
30 October 2019
Bay of Plenty
Scheduled carers not coming
Resolved – provider responded to
Lack of communication about carers not concerns in writing
coming
INFORMATION
Manner and communication from
coordinator
RELEASED
6
2 December 2019
Canterbury
Scheduled carers showing up late
Resolved – provider responded in
Lack of communication about carers
writing
being late
Not notified when new staff were filling
in
7
19 December
Canterbury
HDC section 37 referral to Advocacy
Withdrawn – Advocacy lost
OFFICIAL
2019
Lack of communication about care plan
contact with consumer and
Consumer only had one visit and no
complainant.
further contact
Please note all redactions are made under section 9(2)(a) of the OIA, to protect the privacy of natural persons.
Page 96 of 107
Document 5
s 9(2)(a)
8
23 January 2020
Otago
Manner and communication of
Withdrawn – Advocacy advised
caregiver
she speak with provider directly.
Caregiver returned against consumer’s
No further action
wishes
9
24 February 2020
Canterbury
Continuation of her previous complaint about
Resolved – provider responded to
communication.
concerns.
Lack of communication about who was
providing her care
Lack of regular carers
1982
10
24 February 2020
East Coast
Carers not coming
Resolved – Advocacy supported
Lack of communication about carers not Mr Ford to speak with provider.
THE
coming
Provider responded in writing
11
3 March 2020
Bay of Plenty
Disclosure of mental health notes to her Resolved – provider responded in
ACT
carer who cares for physical injuries
writing
only
12
4 March 2020
Bay of Plenty
Carers cancelled on short notice and
Withdrawn
without a replacement arranged
UNDER
Lack of communication about carers
being cancelled
13
9 March 2020
Manawatū-
Carers not arriving at arranged time
Withdrawn – service improved
Whanganui
Lack of communication about carers
being delayed
Carers not listening to consumer
14
30 March 2020
Waikato
Disabled consumer discharged to care
Resolved – mentoring for self-
of elderly parents
advocacy.
INFORMATION
Lack of communication about this
decision
RELEASED
15
29 April 2020
Wellington
HDC section 37 referral to Advocacy
Not resolved – provider met
Failure to intervene when he reported
resolution outcomes but
his flatmate was bullying him
consumer did not accept the
Privacy breach concerning medication
complaint was resolved.
16
7 May 2020
Southland
Inconsistent care provided for his
Not resolved – provider
scabies – carers giving different care
responded in writing, but
OFFICIAL
instructions
consumer declined meeting.
Inadequate response to complaint
Carers late
Please note all redactions are made under section 9(2)(a) of the OIA, to protect the privacy of natural persons.
Page 97 of 107
Document 5
Lack of communication about carers
being late
17
s 9(2)(a)
17 June 2020
Hawke’s Bay
Carer not showing up
Resolved – provider responded in
Lack of communication about carers not writing
coming
18
18 June 2020
Northland
Unable to get permanent carers
Resolved – provider arranged for
Carers not showing up
a temporary support person until
a permanent one was found
19
18 June 2020
Manawatū-
Lack of communication – unable to get
OPEN
Whanganui
through
1982
Lack of communication about contact
number changing
THE
Lack of communication about changing
support staff for her children
ACT
20
23 June 2020
Hawke’s Bay
Scheduled carers not showing up
OPEN
Lack of communication about carers
being late or not coming
Inadequate response to complaint
UNDER
21
29 June 2020
Auckland
Scheduled carers not showing up
Resolved – care worker confirmed
Lack of communication about carers not
coming
Restructuring of Healthcare NZ making
it difficult to contact them
22
1 July 2020
Canterbury
Carer mixing up medication
Withdrawn
Carers showing up late
OPEN with HDC 20/00868 –
INFORMATION
reviewing section 14 response
23
2 July 2020
South Canterbury
Carers not coming or are late
Resolved – meeting with provider
RELEASED Lack of communication about carers not
coming or being late
24
6 July 2020
Auckland
Carers often off sick with no cover arranged
Resolved – provider apologised
and carers began to show up
regularly
25
13 July 2020
Taranaki
Lack of communication about carer
Resolved – provider responded to
OFFICIAL
changing
concerns
Inadequate care from carer
Manner and communication of carer
Please note all redactions are made under section 9(2)(a) of the OIA, to protect the privacy of natural persons.
Page 98 of 107
Document 5
Lack of communication – unable to
reach provider
26
s 9(2)(a)
17 July 2020
East Coast
Scheduled carers not arriving
Resolved
Lack of communication about carers not
coming
27
21 July 2020
Canterbury
Scheduled carers not arriving
OPEN
Lack of communication – provider not
responding to concerns
Lack of communication – unable to
reach provider
1982
28
21 July 2020
Manawatū-
No relief carer scheduled when usual
Resolved – provider responded to
Whanganui
carer is unavailable
concerns
THE
Lack of communication – unable to
reach provider
ACT
Inadequate response to complaint – not
responded to in a timely manner
29
23 July 2020
Auckland
Manner and communication of carers
Resolved – provider met with
Threatening behaviour from carer
consumer
UNDER
30
30 July 2020
Auckland
Scheduled carers not showing up
OPEN
No alternative support arranged
Delayed/lack of communication about
carer not coming
31
7 August 2020
Canterbury
Manner and communication of carer
Referred to HDC
Threatening behaviour from carer
Inadequate response to complaint
OPEN with HDC 20/01611 –
INFORMATION
drafting section 14
32
7 August 2020
Otago
Scheduled carers not coming
OPEN
RELEASED Lack of communication – unable to
reach provider
Inadequate response to complaint
33
28 August 2020
Hawke’s Bay
HDC section 37 referral to Advocacy
OPEN
No relief carer arranged when
permanent carer went on leave
OFFICIAL
Lack of communication about carer
going on leave
Please note all redactions are made under section 9(2)(a) of the OIA, to protect the privacy of natural persons.
Page 99 of 107
Document 5
Lack of communication – unable to
reach provider
34
s 9(2)(a)
31 August 2020
East Coast
Carers not coming or coming late
OPEN
Lack of communication about carers not
coming or coming late
35
07 September
Nelson
HDC s 37 FRA (C20HDC01551)
OPEN
2020
Inappropriate communication from RN
Manner and communication
36
09 September
South Canterbury
Caregiver not following care plan
Resolved – provided response
1982
2020
Carer refusing to assist with reading and
laundry
THE
37
09 September
Manawatū-
HDC s 37 FRA (C20HDC01395)
Resolved – provided written
2020
Whanganui
Carers not coming
response
ACT
No replacement carers arranged
Lack of communication
Unable to contact provider
38
18 September
Wellington
No replacement carers arranged
OPEN
UNDER
2020
Carers often cancelled
Inconsistencies in care plan
39
23 September
Hawke’s Bay
Carer not changing consumer’s schedule
OPEN
2020
when requested
“Erratic” care – carers not showing up
40
02 October 2020
Otago
Carers arriving late without explanation
OPEN
Carers not coming
Unable to contact provider
INFORMATION
Long phone wait times
41
05 October 2020
Canterbury
HDC s 37 FRA (C20HDC01772)
Resolved – withdrawn as provider
RELEASED Carers showing up late
addressed concerns with him
directly
42
07 October 2020
Manawatū-
Carers not coming
Withdrawn – consumer being
Whanganui
Consumer ended up in hospital
reassessed and may move rest
home
43
13 October 2020
Canterbury
Carers arriving late
OPEN
OFFICIAL
Inconsistent information regarding
student nurse
Please note all redactions are made under section 9(2)(a) of the OIA, to protect the privacy of natural persons.
Page 100 of 107
Document 5
s 9(2)(a)
44
21 October 2020
Manawatū-
Carer not coming
OPEN
Whanganui
Lack of communication about carers not
coming
Unable to contact provider due to long
phone wait times
45
23 October 2020
Taranaki
Carers not showing up
OPEN
Carers showing up late
Carers not staying for proper period of
time
Inadequate response to complaint
1982
THE
ACT
UNDER
INFORMATION
RELEASED
OFFICIAL
Please note all redactions are made under section 9(2)(a) of the OIA, to protect the privacy of natural persons.
Page 101 of 107
Document 6
Complaint Complaint
Date
Region
Type of care
Concerns raised
Stage
no.
Reference and
received
Name
1
s 9(2)(a)
13
Wellington
ACC funded for
Support person not showing up or showing up on
Provider referral.
February
injury
incorrect days/times. Support person not adequately
2020
trained.
1982
2
19
Bay of
High needs
Concerns about changes to call centre which result in
S38(1) – no
THE
February
Plenty
disability
delay in clients accessing care.
action.
2020
ACT
3
3 March
Canterbury Unclear
Support worker not showing up. Ongoing issues.
Provider Referral
2020
UNDER
4
11 March
Wellington
High needs
Diet changed without agreement. Reports being bullied
Formal referral to
2020
disability
by fellow resident and lack of effective intervention by
Advocacy
staff.
5
25 March
Bay of
High needs
Home help services discontinued with insufficient
S38(1) – no
2020
Plenty
disability
warning during COVID-19/coronavirus lockdown.
action.
6
12 May
Canterbury Aged care-
Medication administration error on three separate
Awaiting further
INFORMATION
2020
home help
occasions.
information.
RELEASED
7
17 June
Manawatū- Unclear
Medication administration error on one occasion and not Provider Referral.
2020
Whanganui
given at prescribed times. Concerns about new call
centre system. Cannot get through to change carer times.
Carers are often late as they do not allow travel time
between clients.
OFFICIAL
Page 102 of 107
Document 6
8
s 9(2)(a)
23 June
Otago
High needs
Difficulty accessing carers. Sent many different carers –
Preparing a
2020
disability
too young, inappropriate, leave shortly after they start.
further referral to
Inconsistency of care.
advocacy
9
3 August
Manawatū- Aged care –
Medication administration errors. Carers not turning up.
Awaiting further
2020
Whanganui home help
HCNZ give no notice when carers are not available.
information.
1982
10
3 August
Manawatū- Unclear
Consumer not had support worker turn up for 3 weeks,
Formal Referral
2020
Whanganui
despite calling HCNZ.
to Advocacy.
THE
11
10 August
Hawke’s
ACC funded for
Four occasions over short period of time where carer has
Formal Referral
ACT
2020
Bay
injury
not turned up.
to Advocacy.
12
10 August
Manawatū
High needs
Lack of coordination of care. His carer provided advanced Formal Referral
2020
Whanganui disability
notice of his lack of availability on a particular date, but
to Advocacy.
HCNZ failed to arrange a replacement. Consumer soiled
UNDER
himself and sat in dirty clothing all night.
13
13 August
Waikato
Aged care –
Reports that HCNZ has centralised communication with
Provider referral.
2020
residential
call centre in Auckland and she does not have a
service
coordinator appointed at present to contact to make
changes.
14
24 August
Nelson
ACC funded for
Reports sexual harassment/abuse, threats and
Formal Referral
2020
injury
inappropriate/rude communication with staff member(s), to Advocacy.
INFORMATION
a lack of available staff on afternoon shifts and record-
RELEASED keeping.
15
31 August
Bay of
Aged care –
Reports that the quality of care has declined since HCNZ’s Awaiting further
2020
Plenty
retirement
recent reorganisation. Concerns she no longer receives a
information.
village
roster informing her of when cares will be undertaken and
by whom. Detailed an instance of a worker not showing
up and one where two carers showed up due to
OFFICIAL
Page 103 of 107
Document 6
miscommunication by HCNZ.
s 9(2)(a)
16
1
Canterbury Aged care –
Concerns of a threatening comment made to the
Awaiting further
September
retirement
complainant and she ended up falling, which had not
information.
2020
village
been reported. Reported difficulty with getting hold of
provider on the phone.
1982
17
27
Hawke’s
High needs
HCNZ service changed and she was asked to call the
Awaiting further
September Bay
disability
Auckland office. She experiences long call waiting times
information.
THE
2020
and failure to return her calls, plus inconsistent carers and
poor communication.
ACT
18
28
Canterbury Unclear
Concerns that nurses do not attend at consistent times
Formal referral to
September
and it is difficult to coordinate with his sleep needs. His
Advocacy
2020
nurse ignored his concerns about his wound pain on one
occasion, and his scar opened up afterwards.
19
30
Canterbury Unclear
Concerns about inadequate response to a complaint
Obtaining further
UNDER
September
about inadequate treatment from support staff.
information
2020
20
14 October Otago
High needs
Concerns about incompleteness of rosters, waiting times
Formal referral to
2020
disability
with new call centre, lack of communication regarding
Advocacy
changes to her care, qualifications of staff and going
without cares.
21
14 October Manawatū
Unclear
Concerns about the circumstances surrounding and
Obtaining further
INFORMATION
2020
Whanganui
escalation of a fall.
information
RELEASED
22
27 October Southern
High needs
Concerns about difficult getting hold of provider by
Obtaining further
2020
disability
phone and carers do not attend at consistent times.
information
OFFICIAL
Page 104 of 107

Document 7
Memo
Update on quality issues at Healthcare NZ
Date:
16 February 2021
To:
Adri Isbister, Deputy Director-General, Disability
Copy to:
Clare Perry, Acting Deputy Director-General, Health System Improvement and
Innovation
Jim Nicolson, Manager, Healthy Ageing, Health System Improvement and
Innovation
1982
From:
Amanda Bleckmann, Group Manager Operational Performance, Disability
THE
For your:
Information
ACT
Purpose of report
1.
This memo updates you on actions taken in response to correspondence from Rose Wal , Deputy
UNDER
Health and Disability Commissioner (HDC) on 23 September 2020 about the quality of services
provided by Healthcare NZ (HCNZ).
Background and context
2.
The HDC has received several complaints about the services provided by HCNZ. The general
theme of the complaints was workers not turning up on time and an inability to contact HCNZ.
INFORMATION
3.
The correspondence from HDC was a representative sample numbering sixteen complaints. The
services are funded by District Health Boards (DHBs) (five complaints refer), ACC (three
RELEASED
complaints refer) and the Disability Directorate at the Ministry of Health (five complaints refer).
The funder was unclear for three of the complaints.
4.
The underlying issue largely relates to the move to a national cal centre that began in the third
quarter of 2019 resulting in poor communication between HCNZ support workers and
coordinators, and HCNZ clients and the cal centre.
OFFICIAL
5.
Dr Ashley Bloomfield responded to Rose Wal stating the funders would work collectively with
HCNZ to resolve the issues.
6.
We contacted the HCNZ Chief Executive, Vanessa Dudley, who provided a remediation plan on
11 November 2020. The plan was provided to al funders and outlined the HCNZ response to the
complaints. Vanessa Dudley subsequently resigned from the CE position and Josephine (Jo)
Gagan, CE of the parent company New Zealand Health Group assumed the role of acting CE of
HCNZ.
7.
In December 2020, ACC advised that the remediation plan HCNZ provided sufficient comfort
that HCNZ have addressed the issues raised in complaints made by ACC clients. Communication
between DHB regional Planning and Funding General Managers and Disability concluded that
Page 1 of 2
Page 105 of 107


Document 7
further information was needed from HCNZ for the funders to have confidence that issues were
being appropriately managed.
8.
DHB and Disability representatives agreed to meet with Jo Gagan on 28 January 2021. Following
further complaints between 1 December 2020 and 17 January 2021, ACC also joined the meeting.
Attendees were Ally Emerson from ACC, Kate Sladden, Nicola Ehau, Sandra Williams and Jason
Power representing DHBs, Jon Shapleski and Maria Shcherbakova from TAS, Martin Anderson
representing Disability and Jo Gagan from HCNZ.
Outcome of 28 January 2021 meeting
9.
Jo reported that HCNZ has continued to act on the initial complaints made to the HDC office
and the subsequent complaints (of a similar nature) that HCNZ had received. HCNZ is regularly
updating the remediation plan. Jo agreed to provide the meeting attendees with a copy of the
most recent version of the remediation plan. The version to the end of January 2021 is attached
1982
for your information.
10. Jo advised that within HCNZ, complaints are expected to be managed as close to the source of
THE
the complaint as possible. Senior management is often unaware of complaints that have not
been escalated to the regional manager level. Jo asked the funder representatives to inform the
ACT
regional manager or her of any complaints that are not being resolved within an acceptable
timeframe. As per HCNZ policy, complainants are informed of steps taken to resolve the
complaint.
11. We have planned meetings for each of the next three months
UNDER to track the progress HCNZ is
making against the remediation plan.
12. The Disability directorate continues to have concerns about the systems in place at HCNZ to
facilitate communication between clients and coordinators and between support workers and
coordinators. We continue to receive complaints relating to these issues and we wil continue to
raise our concerns in meetings with HCNZ.
13. The next meeting is on 26 February 2021.
INFORMATION
14. We will provide you with a further update wil fol owing the April meeting. Please advise if you
RELEASED
wish to be updated sooner.
Recommendations
It is recommended that you:
1. Note
The content of this upd
OFFICIAL ate
Yes/No
Signature ___________________________________________________
Date: 17/02/2021
Amanda Bleckmann
Group Manager Operational Performance, Disability
Signature ___________________________________________________
Date:
Adri Isbister
Deputy Director-General, Disability
Page 2 of 2
Page 106 of 107
Document 8
Excerpt of Quality record minutes about actions taken for this complaint
Provider
Complaint Description
Complaint lead Portfolio
Opened
Date
Update
Update
Update
Update
Update
Update
Manager
closed
Healthcare
Letter dated 6/11/20 from
Martin
Bella
9/12/2020 7/05/2021 7/5/21.
22/3/21. A meeting
14/2/21
17/2/21
2/2/21
15/12/20
NZ
Health & Disability
Representatives from
with Jo Gagan was
Updated
Another meeting
Had a meeting
Agreement with
Commissioner to Ashley
funders (DHBs, ACC
held on 26 January
performance
scheduled for 26
with Jo Gagan
DHBs that a meeting
Bloomfield re a table of 34
and Disability) met on
where Jo provided a plan from Jo
Feb.
the last Thursday will be held with
1982
complaints received about
29 April and
verbal update on
Gagan has
Performance
and have agreed Josephine Gagan to
HCNZ from across the
considered the most
actions. This was
been received Improvement
that MoH should
discuss the issues
country since Sep.19
recent Performance
followed up with an
in order to
Plan from HCNZ
let the Regional
raised in the
THE
Improvement Plan
update to the written update Ashley has been
Manager know of complaints, and the
received from HCNZ.
performance
about the
requested, and
any incidents etc. HCNZ plan to
The funders have
improvement plan,
progress.
MoH wil be
We have
address these. ACC
agreed that HCNZ is
received on 19
meeting with
scheduled
is considering how it
ACT
making good progress March and to the end
them every three monthly meetings wil respond to the
to resolve the issues
of February. Reports
months.
with Jo for the
issues. A meeting
that are behind the
that progress is
next 3 months
prior to Christmas
complaints, and
being made on
and hope to
has been requested.
monthly meetings with staffing the call
resolve issues by Martin Anderson
Jo Gagan are no
centres and bedding
then.
longer required. Any
in new systems and
UNDER
quality issues should
practices. Report
be managed local y
shared with Quality
now. This outcome is
team and Portfolio
to be communicated to Manager for review.
the Director-General
by Martin Anderson on
behalf of the 3 funders.
This can be closed
INFORMATION
RELEASED
OFFICIAL
Page 107 of 107
Document Outline
- H202106048 attachments.pdf