
the
Act
Annual Assessment of Results (AAR)
Report of the AAR for the New Zealand Aid Programme in the Ministry of
Foreign Affairs and Trade for AMAs and ACAs completed in 2017/18
under
Final Report
Information
Released
Prepared for //
IOD PARC is the trading name of International
Organisation Development Ltd//
Insights, Monitoring & Evaluation
Official Omega Court
Pacific and Development Group
362 Cemetery Road
New Zealand Aid Programme
Sheffield
Ministry of Foreign Affairs and Trade
S11 8FT
United Kingdom
Date // 3 July 2019
Tel: +44 (0) 114 267 3620
www.iodparc.com

Contents
Acronyms ............................................................................................................................................................ 3
Executive Summary ............................................................................................................................................ 4
1. Introduction .................................................................................................................................................... 9
2. Methodology ................................................................................................................................................. 10
Limitations of the AAR .............................................................................................................................. 13
3. Key findings .................................................................................................................................................. 14
3.1 Robustness of effectiveness ratings ..................................................................................................... 14
the
3.2 Robustness of other DAC criteria ratings (ACAs only) ...................................................................... 21
Act
3.3 Assessment of qualitative analyses in AMAs and ACAs ..................................................................... 22
4. Summary of Findings ................................................................................................................................ 29
5. Conclusions ................................................................................................................................................ 29
6. Recommendations ..................................................................................................................................... 30
under
Appendix 1: Methodology ................................................................................................................................. 32
Appendix 2: Terms of Reference ...................................................................................................................... 41
Appendix 3: Distribution of sample ................................................................................................................. 43
Appendix 4: Influence of scholarship activities on AMA robustness.............................................................. 46
Information
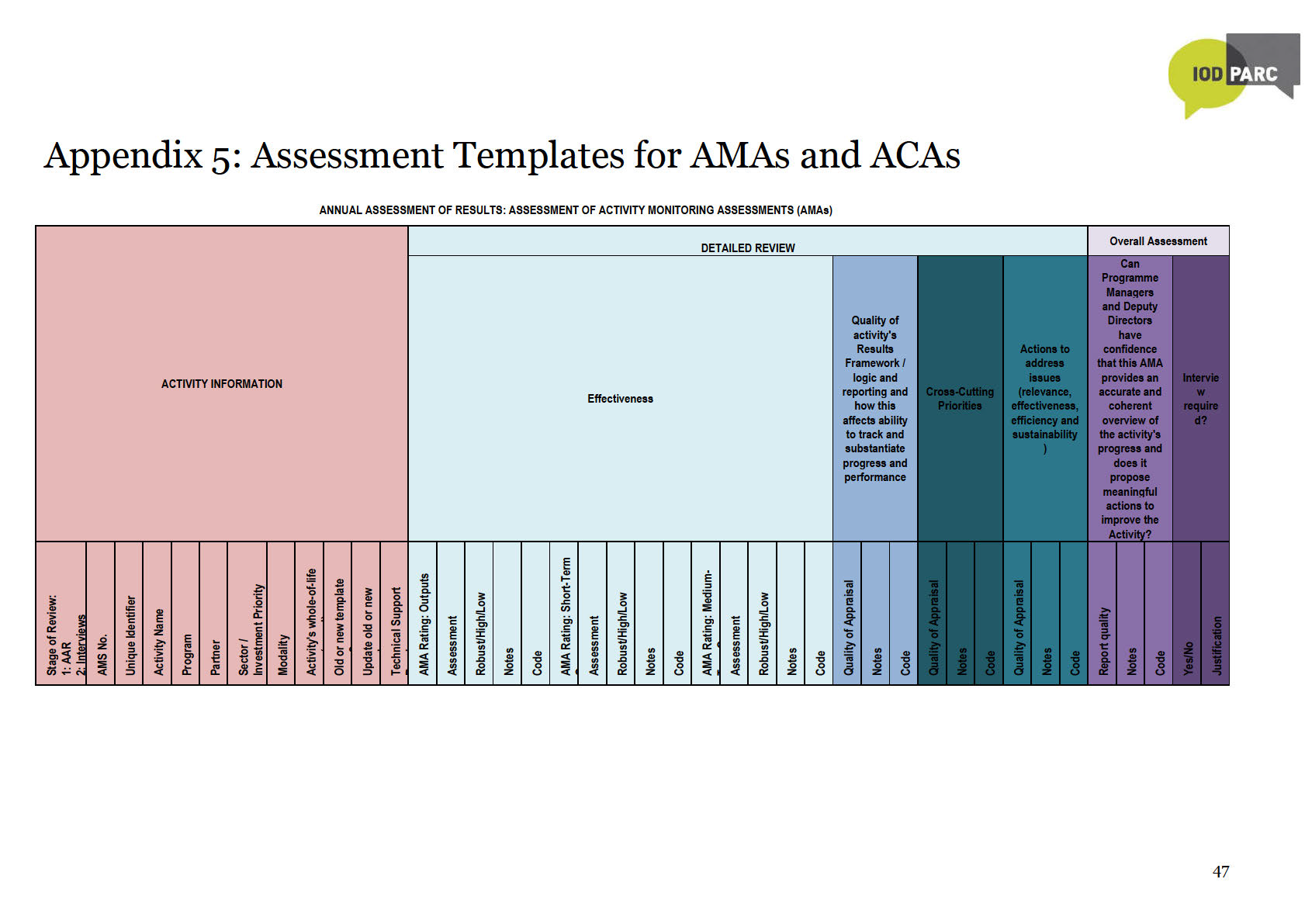
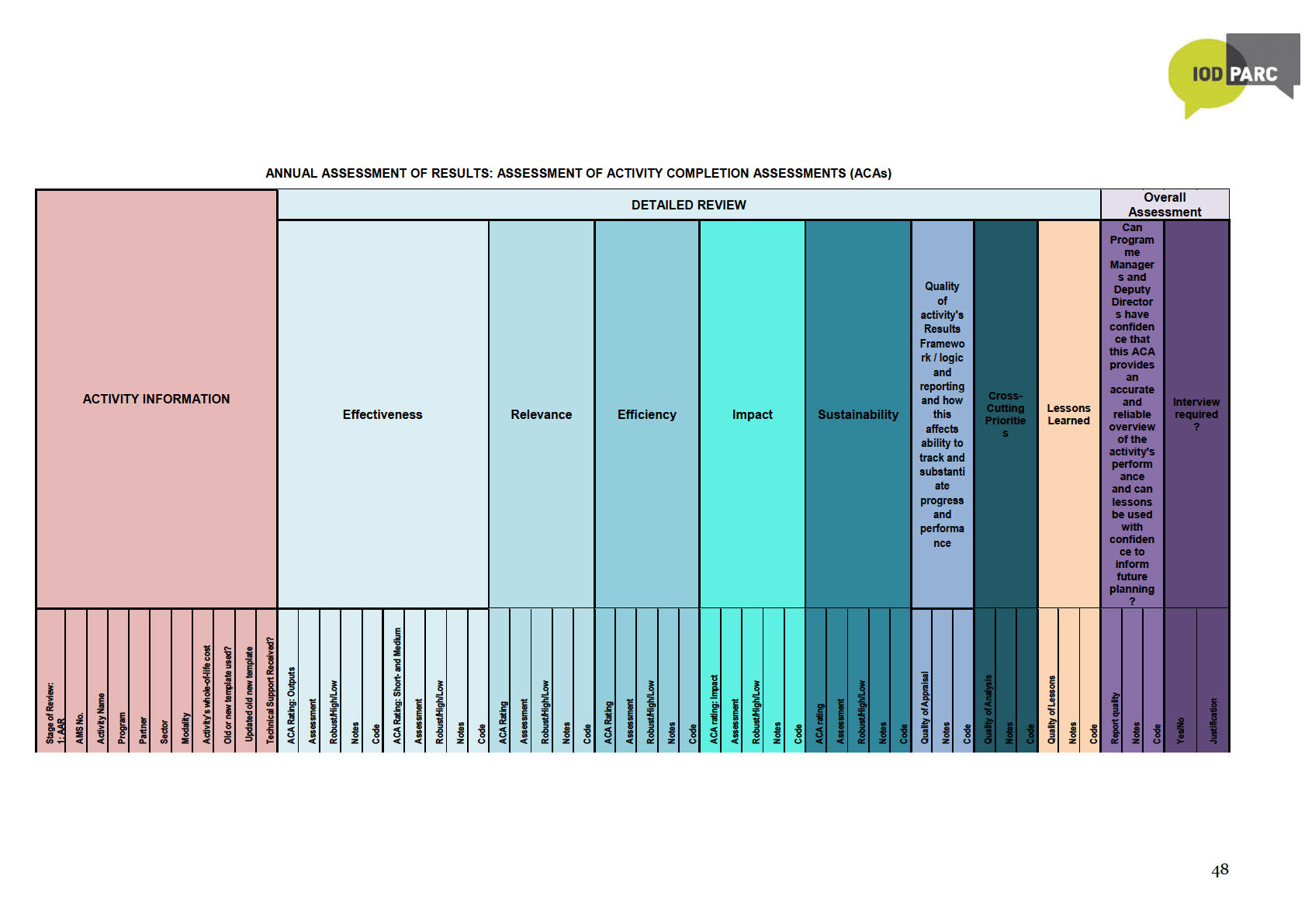
Appendix 5: Assessment Templates for AMAs and ACAs .............................................................................. 47
Appendix 6: Interviewing script ....................................................................................................................... 49
Released
Official

Acronyms
ACA
Activity Completion Assessment
AMA
Activity Monitoring Assessment
AQP
Activity Quality Policy
ARF
Activity Results Framework
CCIs
Cross Cutting Issues
DAC
Development Assistance Committee
DP&R
Development Planning and Results (team)
M&E
Monitoring and Evaluation
the
MFAT
Ministry of Foreign Affairs and Trade
Act
MO
Multilateral Organisation
N/A
Not Assessable
ODA
Official Development Assistance under
RMT
Results Measurement Table
SAM
Scholarships and Alumni Management System
UN
United Nations
VfM
Value for Money
Information
Released
Official
3

Executive Summary
Background
New Zealand’s Aid Programme is delivered through investments (known as Activities) administered
by the Ministry of Foreign Affairs and Trade (MFAT). The performance of individual Activities is
reported through Activity Monitoring Assessments (AMAs) and Activity Completion Assessments
(ACAs). Within AMAs and ACAs, Activity Managers rate performance on a five-point scale against set
criteria. Upon completion of an Activity, ACAs record ratings of effectiveness, relevance, impact,
efficiency, and sustainability. AMAs record ratings of effectiveness of on-going Activities. An
important element of AMAs and ACAs is that they identify issues that may affect the implementation
and results of activities, as well as recommendations and lessons to improve activities.
For many Activities, AMAs and ACAs are the only formal MFAT assessment of their progress and
performance. It is therefore important that MFAT has confidence in their robustness. The Annual
Assessment of Results (AARs) assesses the robustness of ratings in AMAs and ACAs. The AAR also
the
assesses whether AMAs and ACAs are helpful to improve Activities
Act
According to Activity Managers who were interviewed for this AAR, AMA and ACA templates have
become more user-friendly over the last five years through revisions based on outcomes of AARs,
amongst others. AMAs and ACAs are becoming increasingly embedded within MFAT’s performance
management system. Completion rates for AMAs and ACAs have increased substantially from 59% in
2013/14 AAR to 88% in 2017/18, the highest completion rate to date.
This is the fourth (AAR)1, providing an independent quality assurance of a randomly selected
under
representative sample of 66 AMAs and 36 ACAs, drawn from a total of 141 AMAs and 55 ACAs that
were completed between 1 July 2017 and 30 June 2018. Of those selected, 63 AMAs and 28 ACAs
were eventually reviewed.2 AMAs and ACAs with non-robust effectiveness ratings were progressed to
an interview with the relevant Activity Manager, following which reviewers finalised their assessment.
A proportionally low number of interviews conducted with Activity Managers to review non-robust
effectiveness ratings is a major limitation of this AAR3. To enhance comparability with previous
AARs, final effectiveness ratings were adjusted to allow for the low interviewing rate in the current
AAR.4
Information
Summary of Findings
Robustness of Effectiveness Ratings
Released
To have general confidence in the robustness of Activity Managers’ effectiveness ratings across all
AMAs and ACAs, MFAT would expect at least 75% of the assessed ratings to be robust.
MFAT can be reasonably confident in the robustness of AMA effectiveness ratings, especially for
short- and medium-term outcome ratings. Based on the adjusted post-interview ratings, it is
Official
encouraging that the robustness of short-term outcome ratings in
AMAs meets the 75% confidence
threshold, while that of medium-term outcome ratings is just under, at 74%. The robustness of output
ratings still trails at 64%.
1 Three previous AARs were conducted in 2015, 2016 and 2018 for AMAs and ACAs completed between 1 July 2013 – 30 June 2014;
between 1 July 2014 – 30 June 2015; and between 1 July 2016 – 30 June 2017, respectively.
2 The main reason for the differences between selected and reviewed totals is that Activity-related documents could not be provided in
time to be included in the review.
3 The interview rate for the current AAR (33%) is much lower compared to previous AARs (86% in the inaugural AAR; then 92% and 84% in
the two subsequent AARs).
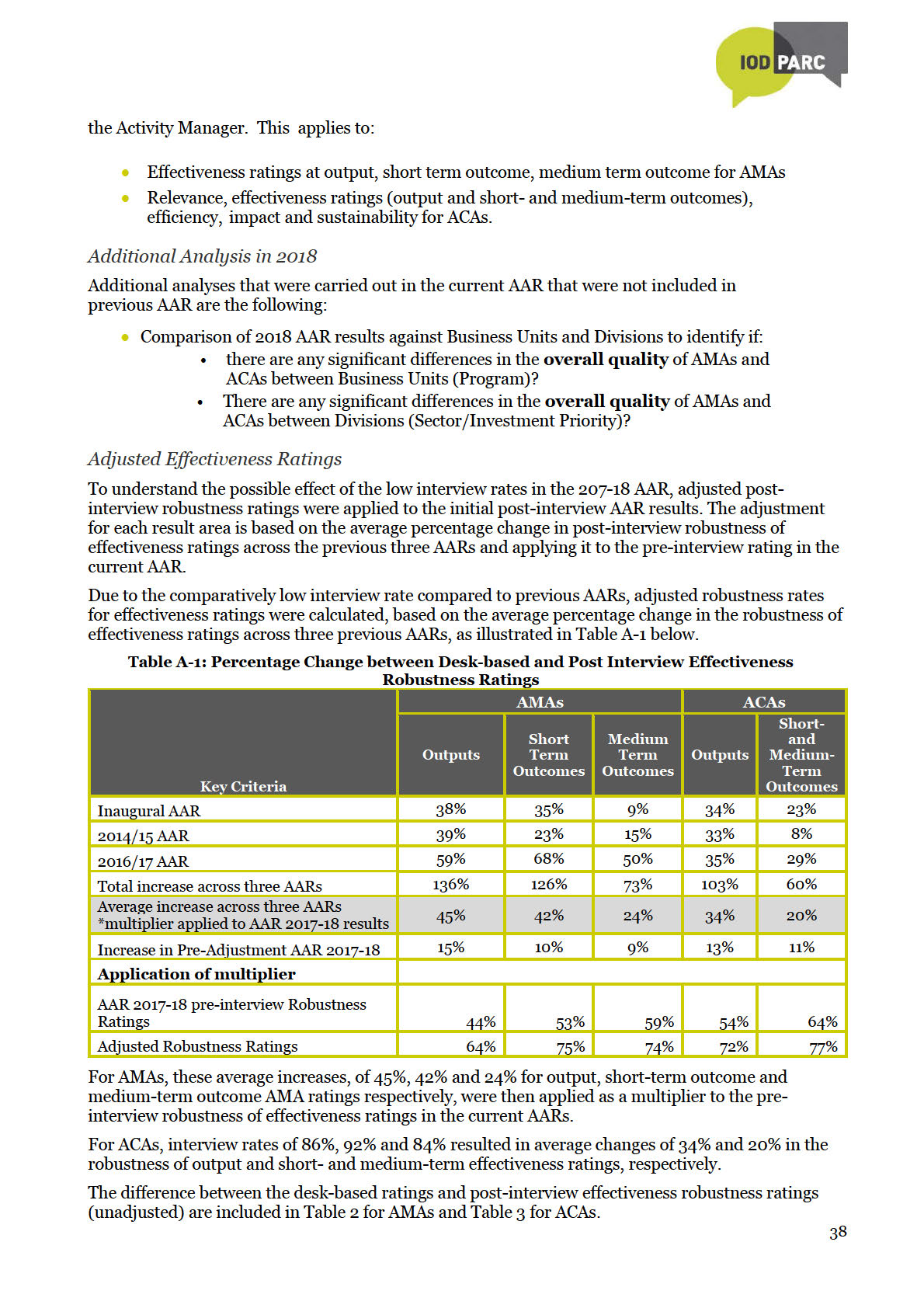
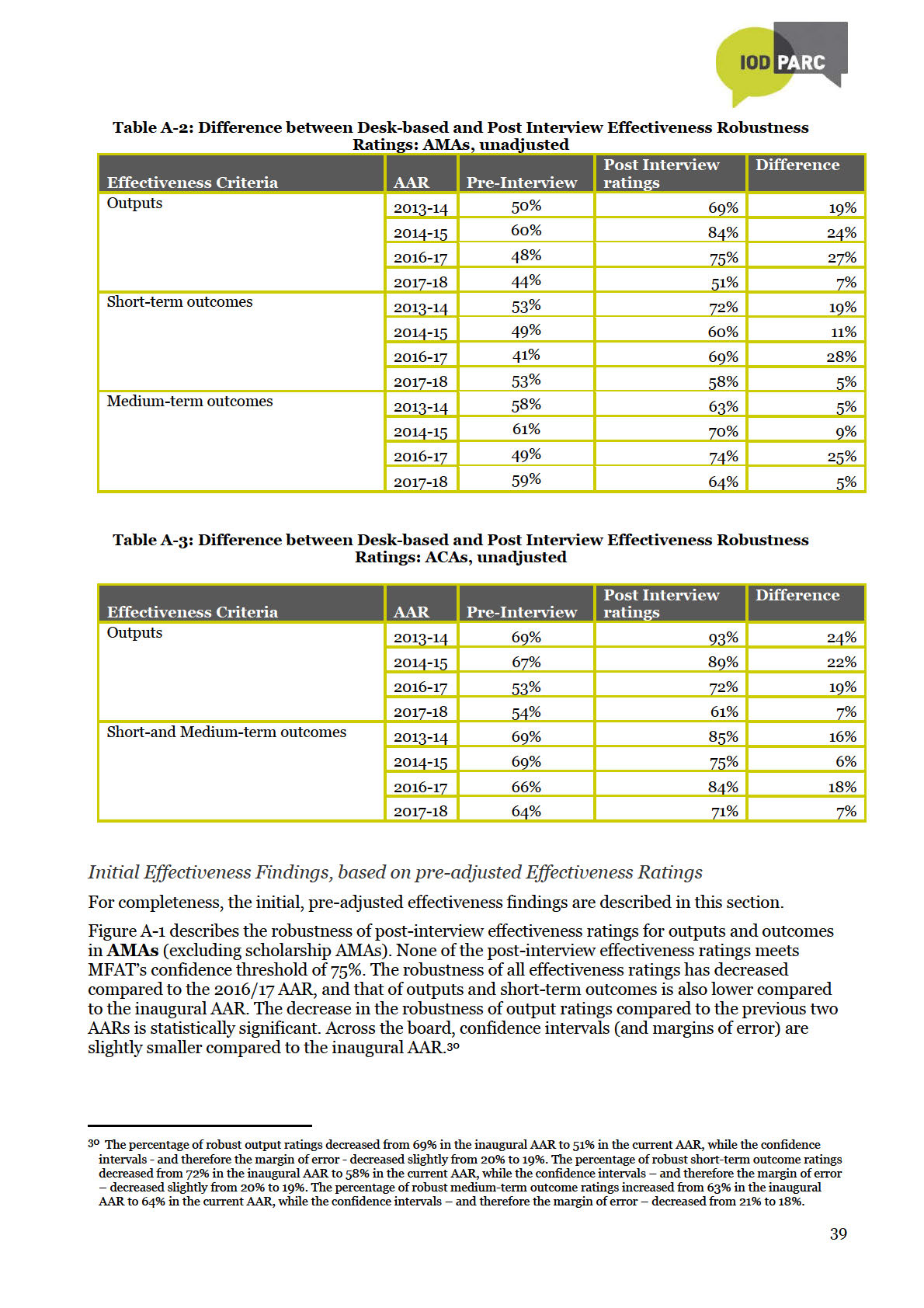
4 The adjustment for each result area is based on the average percentage change in post-interview robustness of effectiveness ratings
across the previous three AARs and applying it to the pre-interview rating in the current AAR. Both the initial post-interview robustness
ratings and the adjusted post-interview ratings have limitations. The initial post-interview ratings are not informed by a proportional
number of interviews compared to previous years and therefore are likely to be understated. The adjusted post-interview ratings are
indicative rather than definitive, but are likely to be closer to what the actual results may have been.
4

The robustness of output and medium-term outcomes ratings for AMAs in the current AAR is lower
compared to previous AARs, but the robustness of short-term outcome ratings is higher. However,
there has been no statistically significant changes in the robustness of AMA effectiveness ratings in
the current AAR compared to both the inaugural AAR and the 2016-17 AAR.5
Based on adjusted post-interview ratings, the robustness of short- and medium-term outcome ratings
in
ACAs, at 77%, exceeds MFAT’s confidence threshold, but the robustness of output ratings trails at
72% - compared to the inaugural AAR, the decrease in robustness of ACA output ratings is likely to be
statistically significant6. When an Activity ends, it is especially important to know whether it has
achieved its results or not. It is therefore encouraging that MFAT can be reasonably confident about
the robustness of short- and medium-term outcome ratings in ACAs.
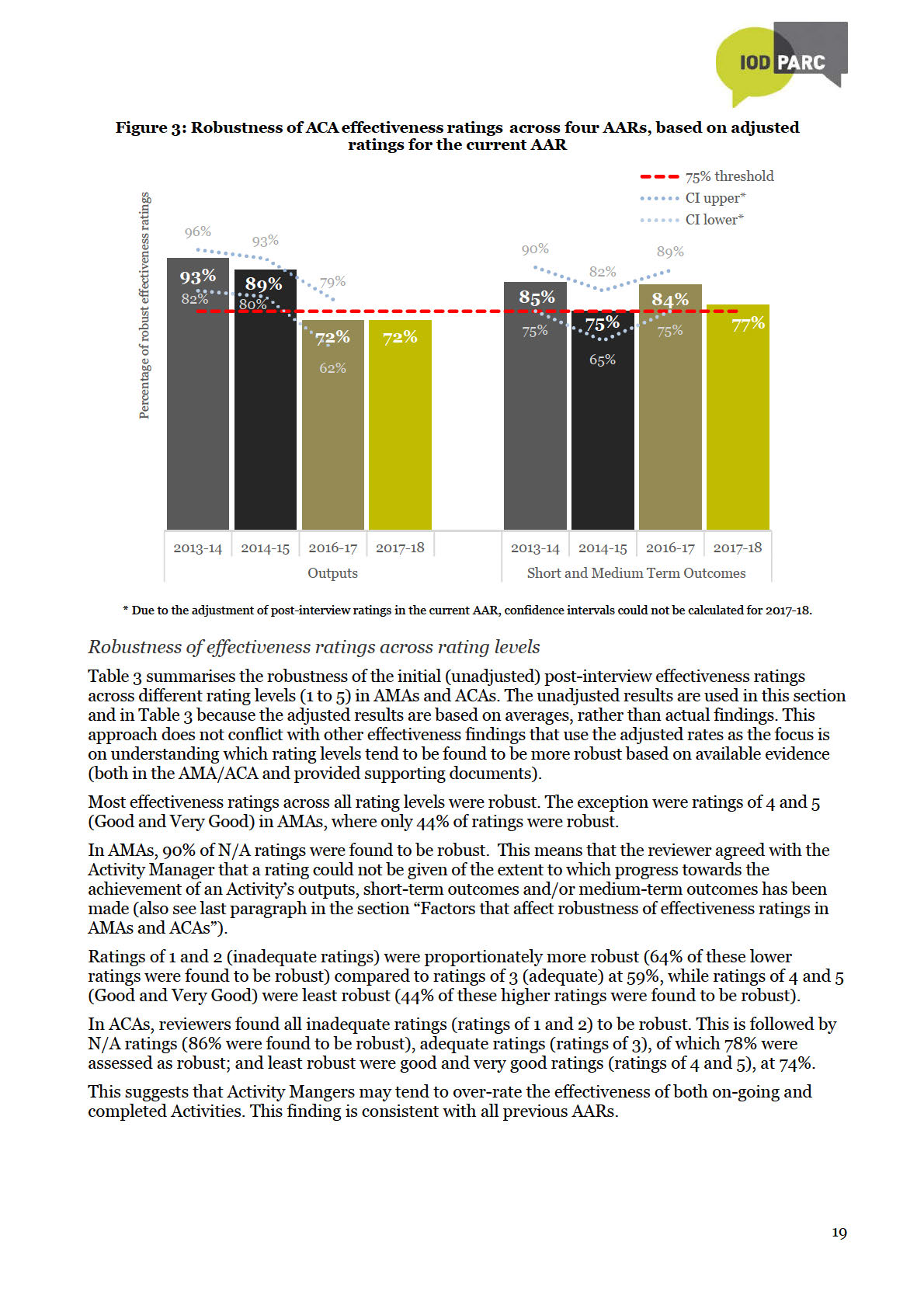
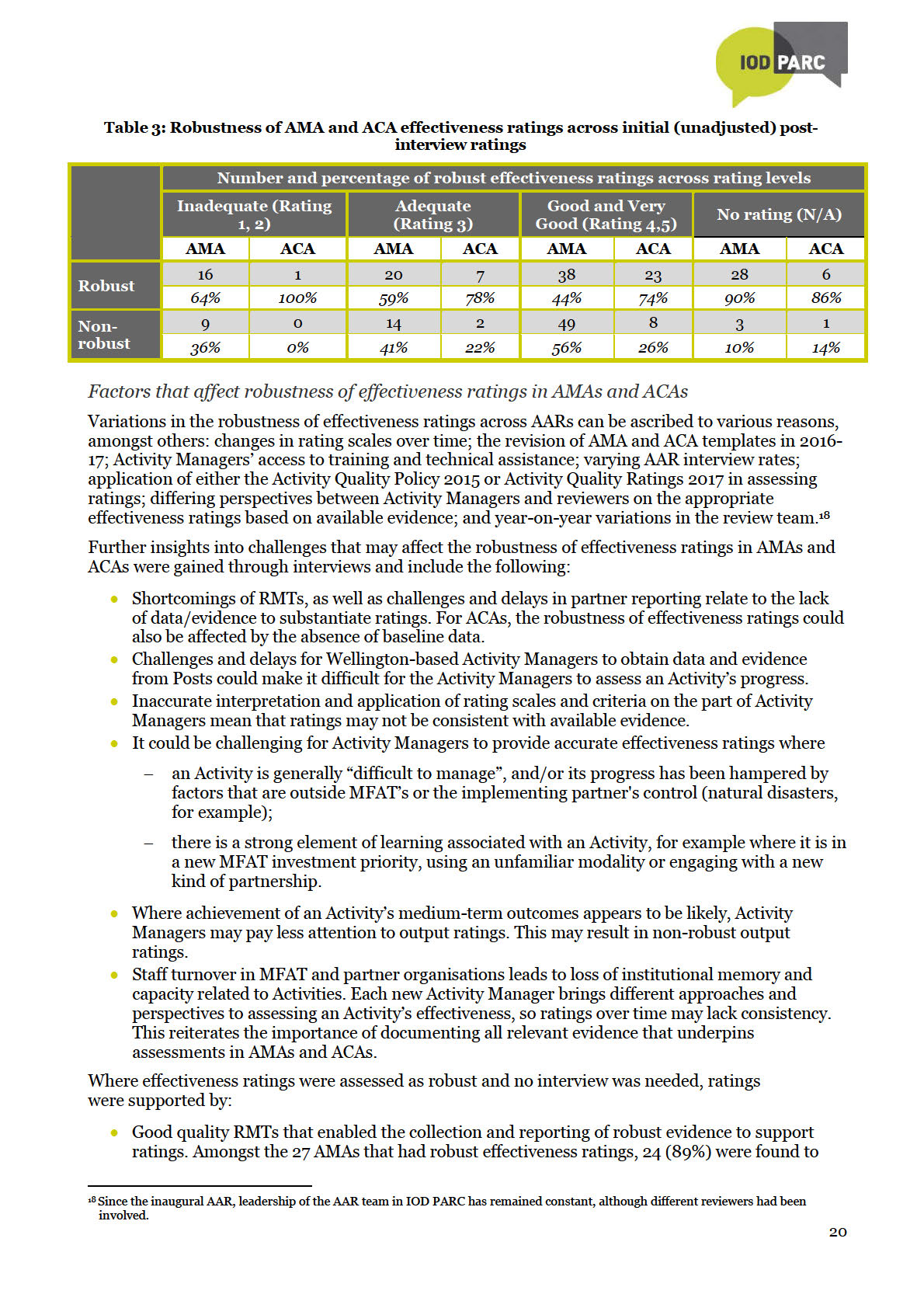
In both AMAs and ACAs, effectiveness ratings of 1 and 2 (inadequate ratings) are more robust
compared to ratings of 4 and 5 (good and very good ratings). This suggest that Activity Managers
may be inclined to over-rate effectiveness of Activities, which is consistent with all previous AARs.
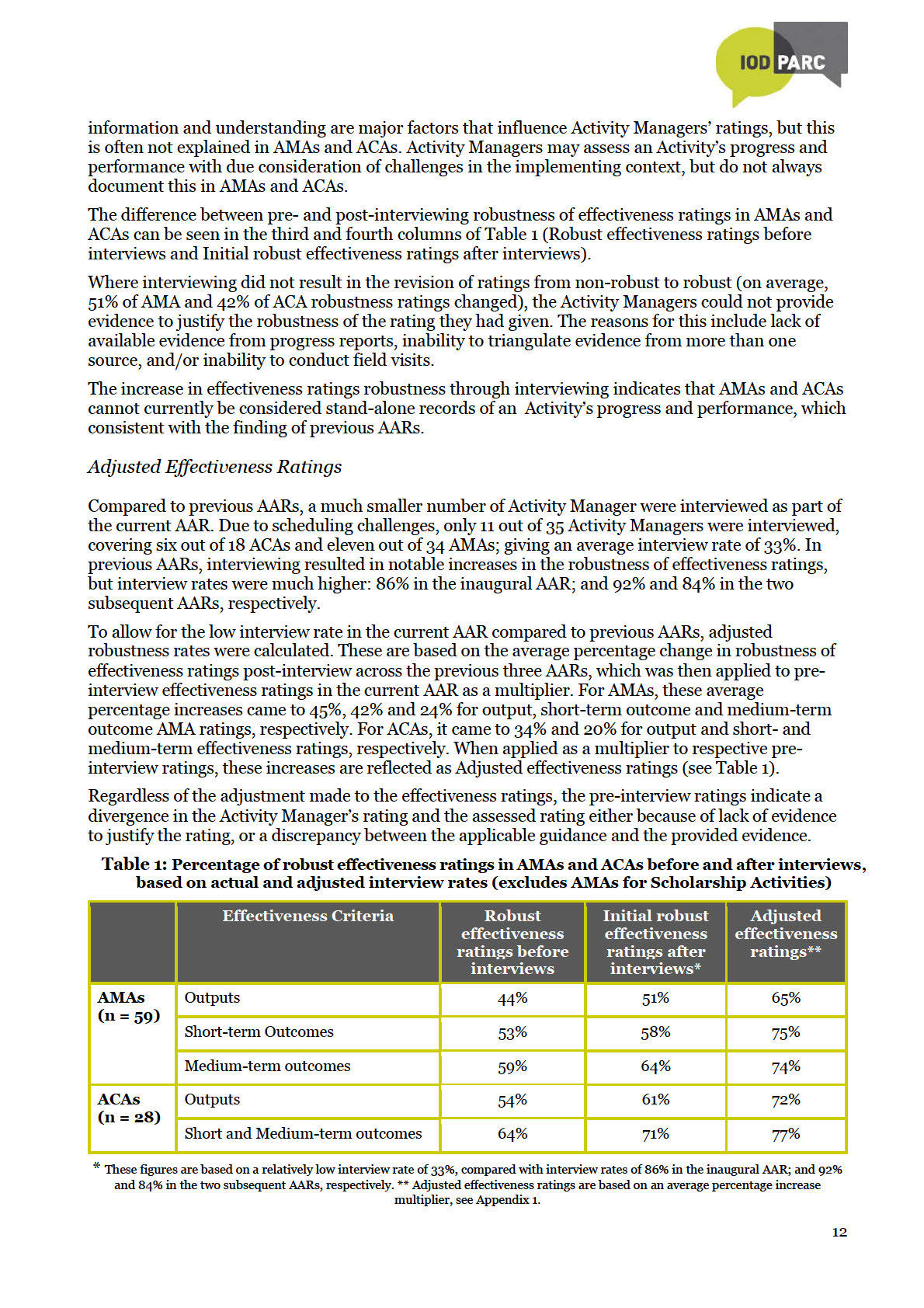
As in previous AARs, robustness of effectiveness ratings for both AMAs and ACAs increased
substantially after interviewing. The main reason is that Activity Managers may not document all the
evidence that informs ratings in the AMA or ACA. Contextual information and understanding are
the
major factors that influence Activity Managers’ ratings, but this is often not explained in AMAs and
ACAs. Activity Managers may assess an Activity’s progress and performance with due consideration
Act
of challenges in the implementing context, but do not always document this in AMAs and ACAs.
Therefore, many AMAs and ACAs still do not capture the evidence that supports effectiveness ratings
in sufficient detail to provide stand-alone records of an Activity’s effectiveness.
Quality of Results Management Tables and influence on Effectiveness Ratings
under
Based on references to Results Management Tables (RMTs) as sources of evidence for completing
AMAs and ACAs, Activity Managers are increasingly relying on RMTs to monitor and report
Activities’ progress. Ratings were often substantiated by references to movements in RMT indictors,
or progress in relation to baselines and targets. An increasing number of Activity Managers are also
proposing appropriate actions to address identified shortcomings of RMTs.
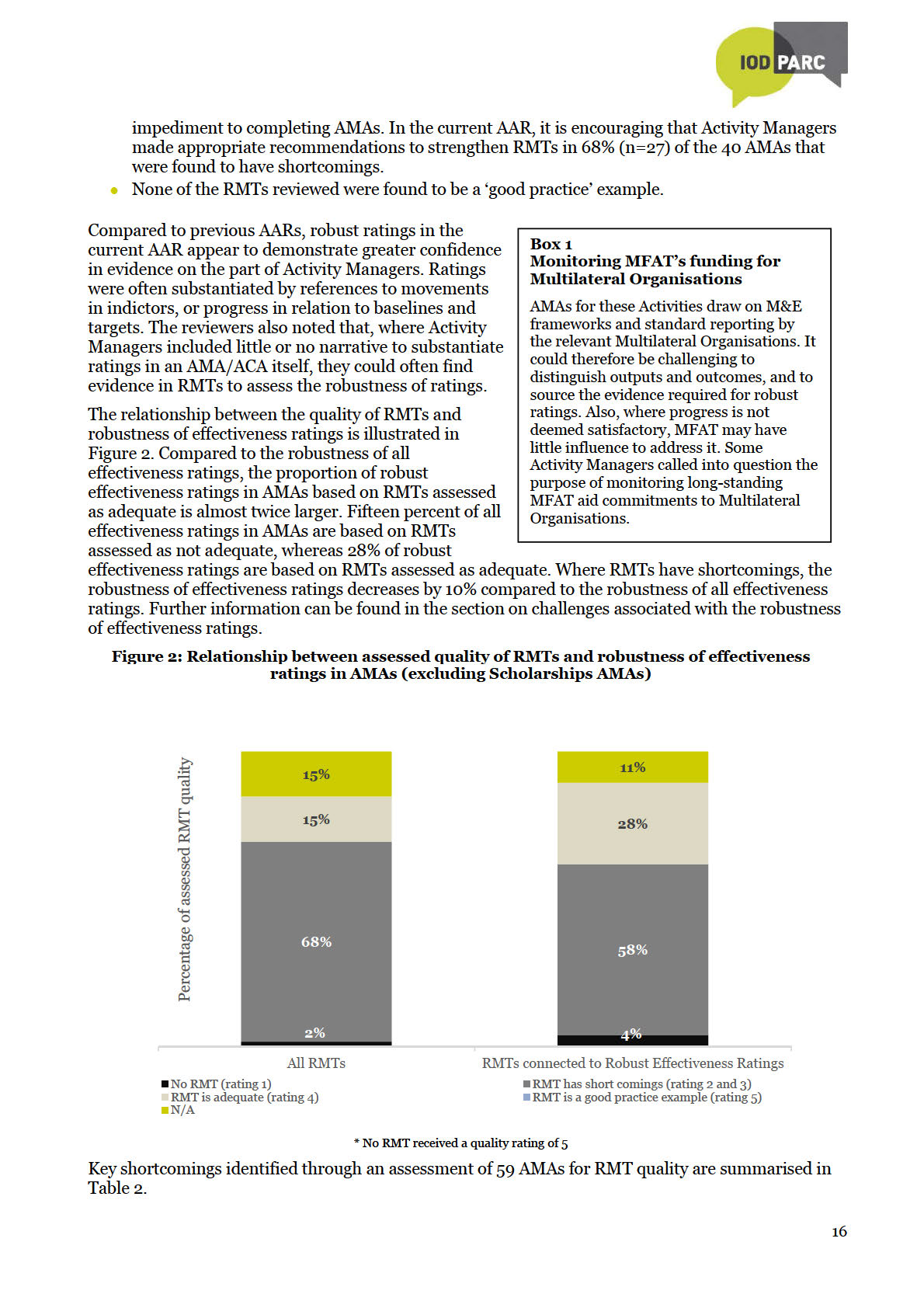
However, RMT shortcomings continue to impede the quality of AMAs and ACAs. In the current AAR,
15% of AMAs (n=9) were based on RMTs assessed as adequate, compared to 68% (n=40) where
RMTs were found to have shortcomings. Many RMTs are not updated regularly and may not reflect
Information
the evolving reality of dynamic Activities. Other major shortcomings of RMTs include the absence of
baselines, targets and data to monitor and report progress. It appears that completing AMAs and
ACAs for complex Activities, for example multi-county and multi-donor Activities, as well as
Activities funded through Budget support, could be challenging because RMTs for these Activities
Released
are not straight-forward. Per MFAT guidelines, AMAs for funding to Multilateral Organisations draw
on the Strategic Plans and annual reports of the organisations themselves. Their annual reporting is
therefore not based on an MFAT RMT and does not provide a clear-cut fit with AMA assessment
criteria.
Official
Robustness of other DAC Criteria ratings in ACAs
MFAT guidelines for the assessment of the DAC criteria of relevance, efficiency, impact and
sustainability were revised in 2017 and incorporated in AMA and ACA templates. However, the
reviewers based their assessment of the robustness of ratings on outdated guidelines in Annex 1 of
the 2015 Aid Quality Policy (AQP). With this limitation in mind, the robustness of DAC criteria
ratings in ACAs has predominantly improved compared to previous AARs but remains below the
75% confidence threshold. More specifically:
5 Assessment of statistical significance is limited by availability of detailed data from the inaugural AAR and the adjustment approach
applied in 2017/18.
6 Assessment of statistical significance is limited by availability of detailed data from the inaugural AAR and the adjustment approach
applied in 2017/18.
5

the robustness of relevance, efficiency and sustainability ratings has improved, following
almost consistent decreases over the previous three AARs.
the robustness of impact ratings is higher compared to the first two AARs but has decreased
slightly compared to the previous AAR. A key challenge in assessing an Activity’s impact at
completion appears to be the absence of baseline data.
Bearing in mind that that ratings of these criteria were not discussed during interviews, and
despite encouraging increases in robustness of sustainability and impact ratings, confidence in
these ratings would still be somewhat lacking.
Cross-Cutting Issues
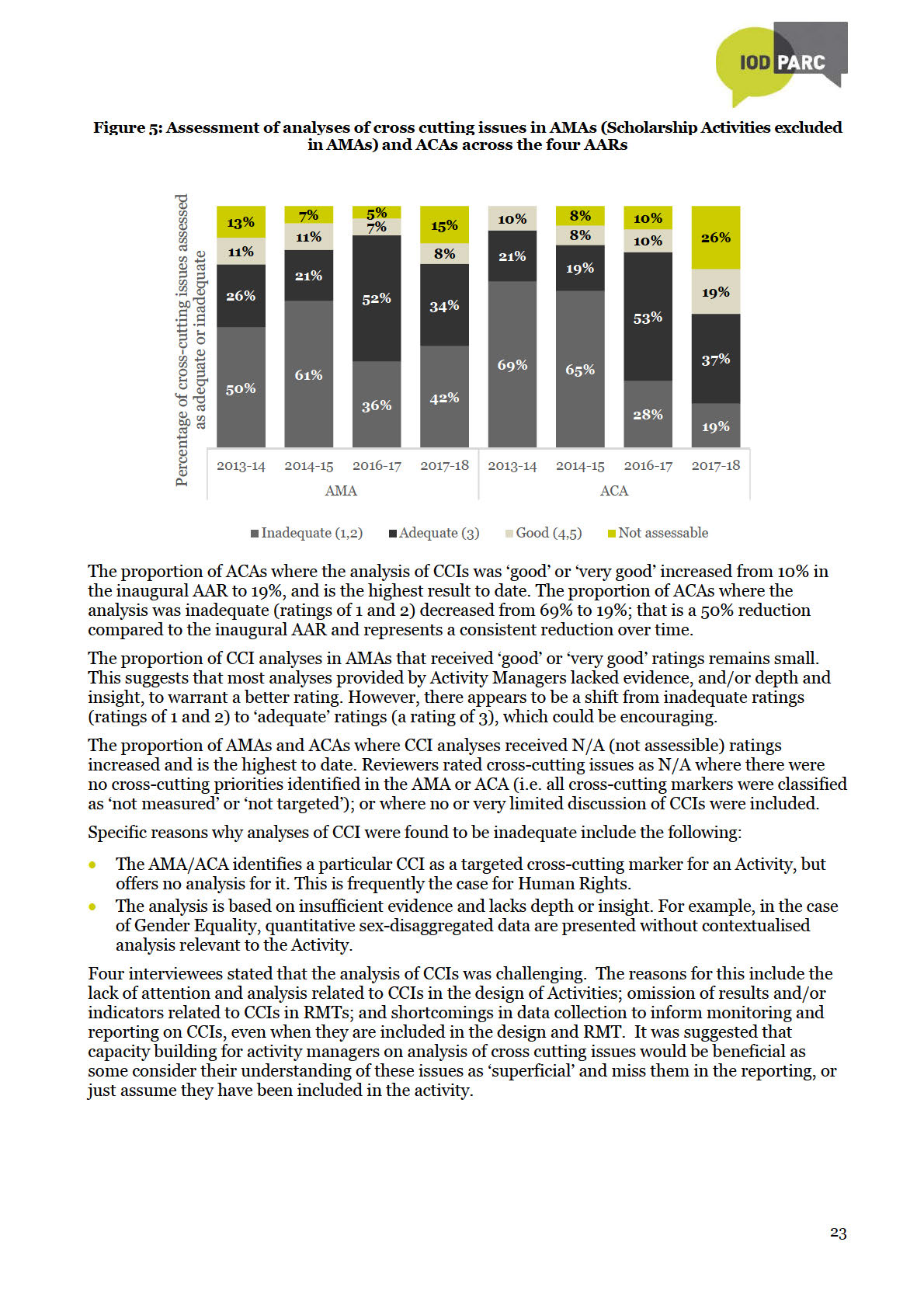
While the assessment of Cross-Cutting Issues (CCIs) remains a challenging aspect of AMAs and
ACAs, it is encouraging that the proportion of ACAs containing ‘adequate’
or better
analyses of CCIs
has increased substantially over time. However, the proportion of CCI analyses in AMAs that
received ‘good’ or ‘very good’ ratings remains small and has decreased since the previous AAR. This
suggests that analyses provided by Activity Managers may still lack evidence, and/or depth and
the
insight, to warrant high ratings.
Act
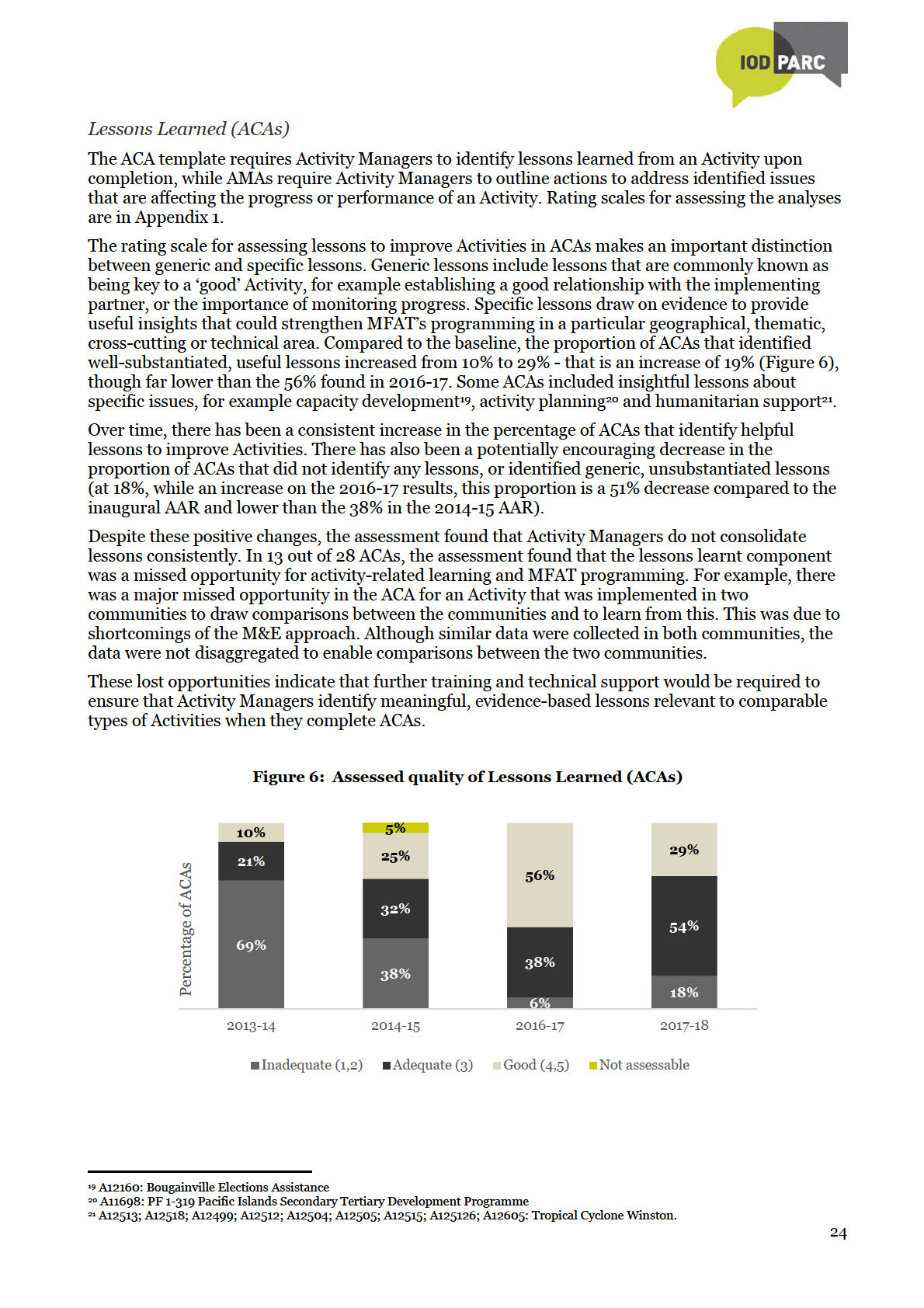
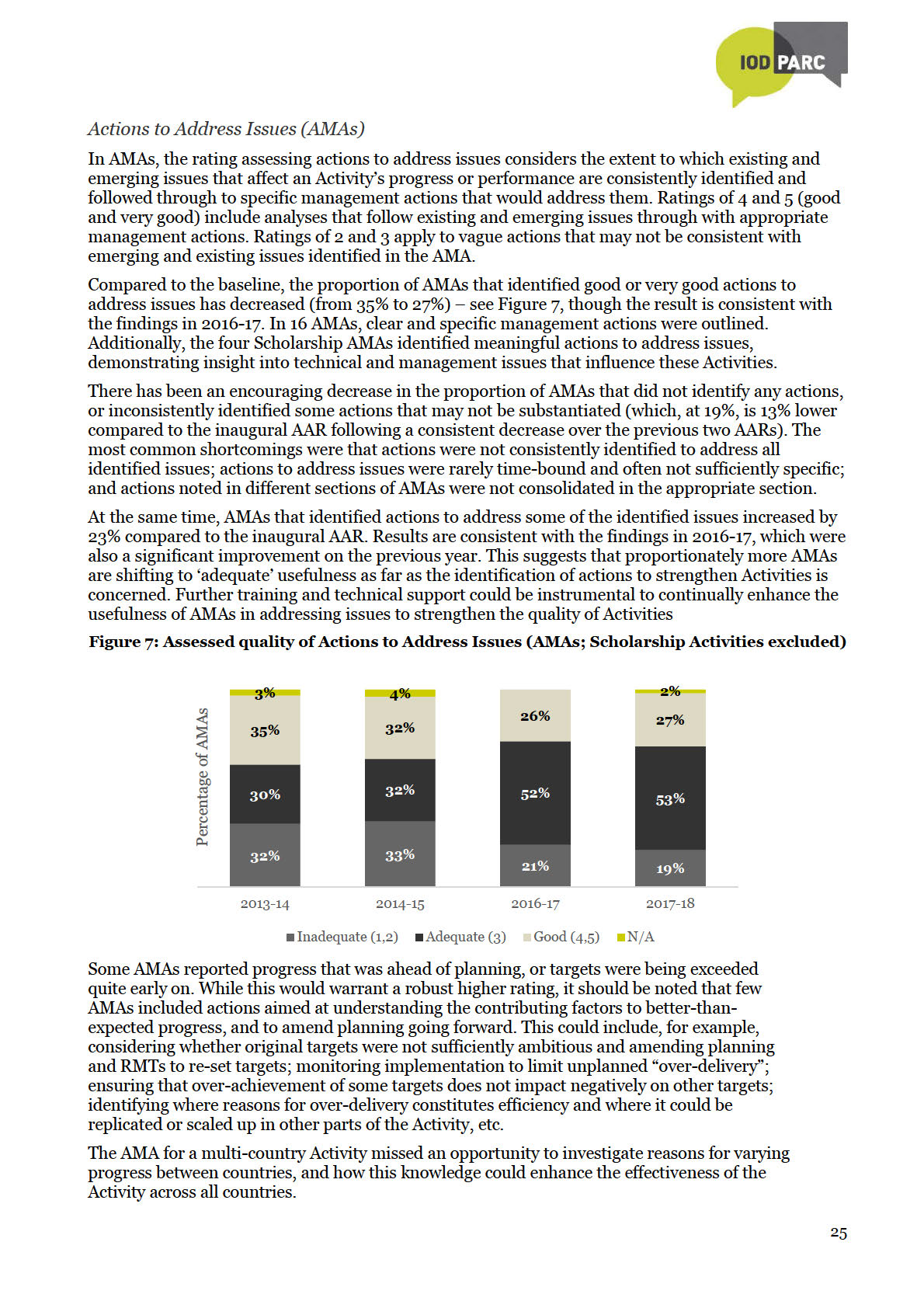
Actions to Address Issues (AMA) and Lessons Learned (ACAs)
In AMAs, the overall quality of proposed actions to enhance Activities’ performance has increased
over successive review periods. Compared to the inaugural AAR, the proportion of AMAs that
identified lessons assessed as inadequate decreased by 13%. At the same time, the proportion of
lessons assessed as ‘good’ or ‘very good’ has also decreased slightly (8% from baseline), suggesting
under
that actions to strengthen on-going Activities are pooling in the ‘adequate’ category.
In ACAs, lessons to inform future Activities remain of a relatively high quality – 82% of ACAs
identified meaningful, useful lessons to strengthen future activities. This is 19% more compared to the
inaugural AAR, but 14% less that the 2016-17 AAR. It is very encouraging that the proportion of ACAs
that did not identify any lessons, or identified generic, unsubstantiated lessons, has decreased by
51% compared to the inaugural AAR.
Drawing on AMAs and ACAs to improve Activities
Information
The extent to which AMAs and ACAs can be used to improve Activities considers whether they
articulate a plausible, evidence-based story of an Activity’s progress and performance, and then
identify key issues and helpful recommendations/lessons to strengthen the Activity (or Activities in
general) going forward. The assessment is based on different criteria to the effectiveness ratings and
Released
therefore results may diverge.
Despite some missed opportunities to identify actions or lessons that could improve Activities, MFAT
can be cautiously confident that both AMAs and ACAs can be drawn on to improve Activities.
Qualitative elements in the majority of AMAs and ACAs provide insightful assessments across a range
Official
of issues, and they identify meaningful actions and lessons to inform activity improvement.
The proportion of AMAs and ACAs that cannot be drawn on to improve activities has
decreased steadily, but so has the proportion that are considered highly informative. This
has resulted in a net increase the proportion that are considered ‘adequate’ in documenting
information that can be drawn on to improve Activities. Therefore, most AMAs and ACAs
contain helpful information that can be drawn on to improve Activities.
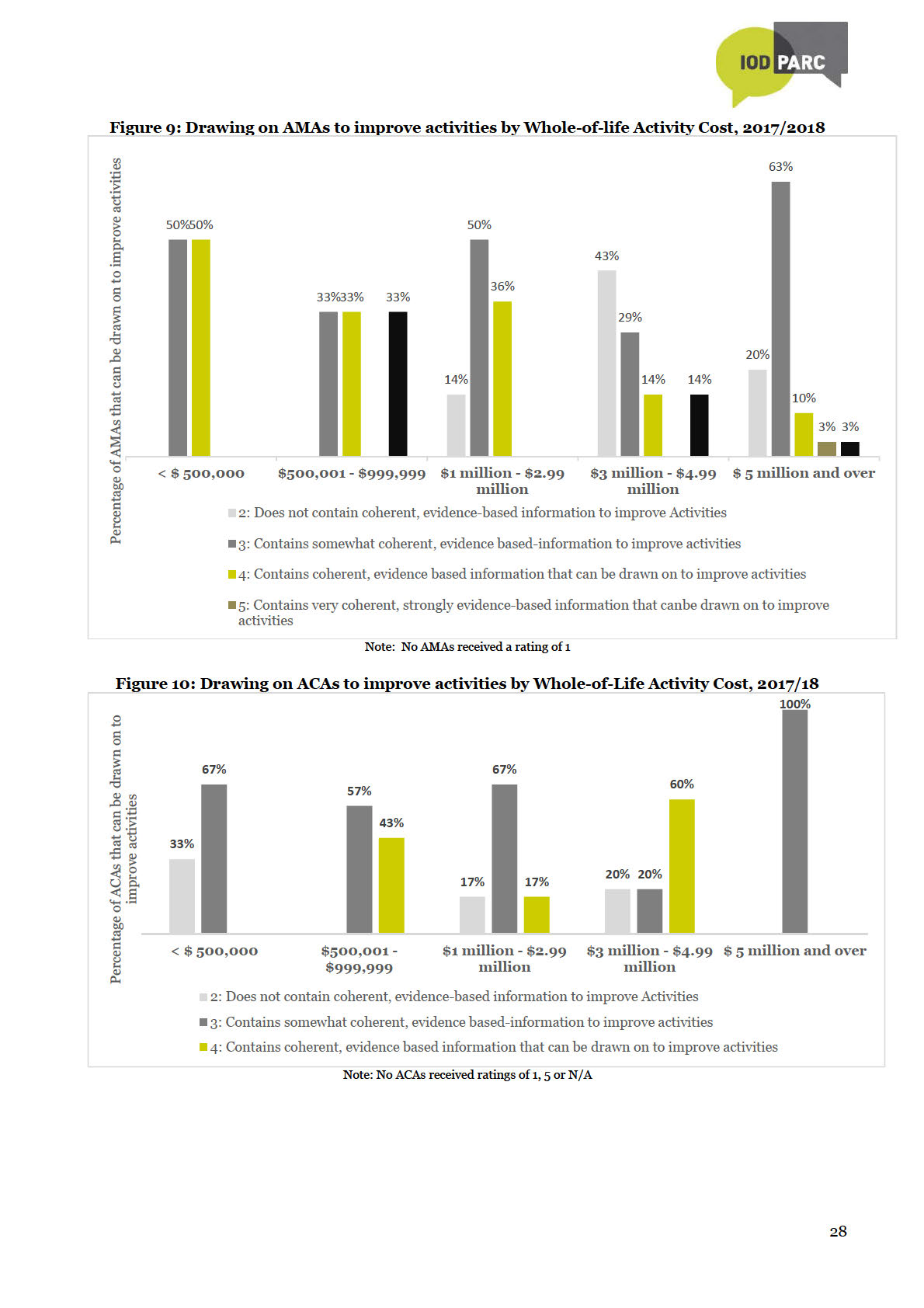
A relatively large proportion of AMAs (20%, or six AMAs) for Activities with large whole-of-
life costs ($5 million and more) did not provide helpful information to improve the
associated Activities. This can be ascribed partly to the fact that most complex Activities, as
well as funding of Multilateral Organisations, have large budgets but there is limited scope
for proposing ways within MFAT’s control to strengthen them.
6
 Conclusions
Conclusions
1. Despite improvements in qualitative aspects of reporting, AMAs and ACAs still do not provide
sufficiently comprehensive or stand-alone records of Activities’ progress. As in previous AARs,
Activity Managers draw on evidence from a range of sources to assess the effectiveness of
Activities but tend not to document all this evidence in AMAs and ACAs. If the evidence is not
comprehensively documented, the loss of institutional knowledge leaves substantial gaps,
especially where staff turnover is high. When these gaps build up year-on-year, new Activity
Managers might find it challenging to complete insightful AMAs and ACAs, thereby jeopardising
the robustness of AMAs and ACAs in the longer term.
2. Despite remaining challenges around the robustness of effectiveness ratings, AMAs and ACAs
generally include helpful information to improve Activities. Providing helpful information to
improve complex Activities, which often have high whole-of-life costs, are challenging since ways
to improve these Activities may not be within MFAT’s full control.
3. So far, AARs have not revealed major statistically significant results related to AMA and ACA
improvement over time. However, due to contextual factors such as the capacity and capability of
the
Activity Managers, incentives, etc. in an environment of relatively high staff turnover, MFAT
does not expect to see statistically significant linear improvements over time.
Act
Recommendations
1. AMAs and ACAs should remain as essential building blocks of the Aid Programme’s performance
management system. Activity Managers use AMAs and ACAs to reflect and assess the progress,
performance and challenges of Activities and they serve as important repositories of institutional
under
memory and continuity during Activity implementation. Increasingly insightful and usable
lessons and actions to address issues, if harnessed through a robust knowledge management
system, could also prove valuable in strengthening Activities.
2. Ongoing training and technical support would be important to ensure that gains made in the
robustness and usefulness of AMAs and ACAs are maintained and enhanced. Gradual
improvements are becoming evident, but it would be important to address known challenges and
strengthen capacity to maintain this positive momentum and to prevent the gains made from
being lost.
Information
Continue to provide training and guidance for Activity Managers in Wellington and at Post
(including locally-engaged staff) to ensure that they understand why and how to document the
evidence base for AMAs and ACAs fully, yet concisely, to increase the proportion of AMAs and
ACAs that provide stand-alone records of Activities’ progress and performance. This would be
Released
instrumental to lift the robustness and usefulness of AMAs and ACAs (and therefore their value
as essential building blocks of the Aid Programmes performance management system) to a
higher level.
Training and support in the following priority areas could be considered:
Official
Documenting consolidated evidence from several sources to justify effectiveness and
DAC criteria ratings.
RMT quality and wider socialisation of RMTs as foundations of Activity design,
monitoring and reporting, as well as dynamic tools for Activity improvement.
MERL expert assistance to support regular reviewing and updating of RMTs to ensure
that they remain relevant and up-to-date.
Strengthening RMTs and monitoring of complicated and complex Activities, for example
multi-donor and multi-country Activities, as well as Activities funded through budget
support.
Improving consistency and coherence in AMAs and ACAs, including identifying issues
that affect the progress and performance of Activities, and following this through into
7

meaningful, evidence-based actions to improve on-going activities (in AMAs), or lessons
relevant to comparable types of Activities when they complete ACAs.
3. Given the size of MFAT’s funding to Multilateral Organisations and the unique arrangements
around their monitoring, it could be beneficial to tailor guidance for the AMAs of these Activities.
4. Provide support to Activity Managers to identify and perceptively address appropriate Activity
cross-cutting markers:
Where a cross-cutting marker is identified as relevant, it should be dealt with
consistently and perceptively throughout the design, monitoring and reporting of the
activity, including in AMAs and ACAs.
Avoid including cross-cutting markers that are not relevant to an Activity in its
AMA/ACA.
5. AARs should continue to be conducted on a periodic basis to monitor the effect of known
enablers and constraints to the robustness and usefulness of AMAs and ACAs, as well as to
identify emerging challenges and actions for their continuous improvement. A larger database
will also enable meaningful trend analyses of the robustness and usefulness of AMAs/ACAs
the
across different sectors, programmes and budget levels.
Act
under
Information
Released
Official
8

1. Introduction
Background
New Zealand’s Overseas Development Assistance (ODA) is delivered through Activities administered
by the Ministry of Foreign Affairs and Trade (MFAT). AMAs and ACAs are internal assessments of the
Activities’ performance and provide forward-looking actions and lessons to improve Activities. They
form the building blocks of the Aid Programme’s Performance System.
AMAs are completed annually for Activities expending over $250,000 per annum, or
smaller Activities with a high-risk profile. They rate and describe effectiveness of on-going
Activities, and provide a descriptive assessment of performance against relevance,
efficiency, sustainability, cross-cutting issues, risk, Activity management and actions to
address identified issues.
On completion of activities with a total expenditure over $500,000 ACAs are completed,
the
ideally within one month of receiving the final Activity Completion Report from the
implementing partner. ACAs rate and provide a narrative assessment of an Activity’s
Act
performance in relation to five Development Assistance Committee (DAC) criteria, namely
relevance, effectiveness, efficiency, impact and sustainability; they also comment and
provide analyses on cross-cutting issues, risk and Activity management, and identify lessons
to improve future Activities.
Completion rates for AMAs and ACAs have increased since 2013/14. The completion rate for 2014/15
AMAs and ACAs was 79%, which was an increase of almost 20% from 2013/14. The completion rate
under
for 2016/17 AMAs and ACAs was 76%. AMAs and ACAs from 2017/18 had the highest completion rate
ever, namely 88%.
During interviewing, eight (of 11) Activity Managers noted that revisions of AMA and ACA templates
over the last five years have made their completion easier, more useful and less time consuming.
Three Activity Managers stated that they had completed training and knew where to access support
if they required assistance with the completion of AMAs/ACAs. Two Activity Managers – one based
at post and one in New Zealand – noted that some staff at Post were unaware/unable to access the
same level of training/support that is offered to Wellington-based staff. Both stated that this could
Information
be improved by increased promotion of available support at Post and including the information in
orientation training for locally-engaged staff, in particular.
Purpose of the AAR
Released
For many Activities, AMAs and ACAs completed by Activity Managers are the only formal MFAT
assessment of their progress and performance. Aggregated ratings data from AMAs and ACAs provide
a snapshot of the performance of New Zealand’s ODA. It is important to have confidence in the
robustness of these ratings. AARs assess the robustness of Activity Managers’ ratings of Activities’
effectiveness. It also assesses the overall usefulness of AMAs and ACAs, as well as the analysis of
Official
cross-cutting issues, actions proposed to address issues (AMAs), and of lessons learnt (ACAs)
presented by Activity Managers.
The purpose of the AAR is to:
assess the level of confidence that MFAT can have in the robustness of AMAs and ACAs
inform the Insights, Monitoring & Evaluation team’s efforts to strengthen the Aid Programme’s
Performance System
provide input to the Aid Programme Strategic Results Framework.7
7 Level 3 of the New Zealand Aid Programme Strategic Results Framework incorporates the following indicators pertaining to the
quality of AMAs and ACAs:
2.3 : Percentage of AMAs and ACAs rated 3 or higher on a scale of 1-5 reviewed against quality standards
2.4 : Percentage of AMAs and ACAs rated 3 or higher on a scale of 1-5 reviewed against quality standards for Cross-cutting issues
9

This is the fourth Annual Assessment of Results (AAR) that provides an independent quality
assurance of AMAs and ACAs. It was conducted for AMAs and ACAs completed between July 2017
and July 2018.8 It describes findings from a sample of 66 AMAs and 36 ACAs, drawn from a total of
141 AMAs and 55 ACAs. Of those selected, 63 AMAs and 28 ACAs were eventually reviewed.9
Effectiveness ratings in 34 AMAs and 18 ACAs were found to be inconsistent with documented
evidence and 35 Activity Managers10 were identified for interviewing to clarify these ratings.
Interviews were conducted with 11 Activity Managers, covering eleven AMAs and six ACAs. This
constitutes an overall interview rate of 33%, which is much lower compared to previous AARs, and
which is a major limitation of the current AAR.
Structure of the Report
The report starts with a brief overview of the AAR’s purpose (Section 1) and methodology, including
limitations (Section 2). Section 3.1 deals with the robustness of effectiveness ratings in AMAs and
ACAs, while Section 3.2 deals with the robustness of other rated criteria, namely relevance, efficiency,
sustainability and impact (ACAs only). Challenges to the robustness of effectiveness ratings are also
discussed, including the role of Results Management Tables (RMTs). Section 3.3 reflects on the
assessed quality of non-rated criteria, namely Actions to address Issues Identified (AMAs), Lessons
the
Learned (ACAs) and the overall usefulness of AMAs and ACAs. The analysis of Cross-Cutting Issues is
also discussed. The report ends with conclusions and recommendations in Sections 4 and 5
Act
respectively.
2. Methodology
under
The methodology for the AAR was developed in consultation with MFAT and has been refined over
four successive AARs. A summary is provided here, with more detail in Appendix 1.
Sampling
The AAR is based on a statistically representative sample of AMAs and ACAs that met the following
criteria:
it was submitted between July 2017 and July 2018
it was completed within 12 months after the assessment period ended.
Information
A total population of 141 AMAs and 55 ACAs met these criteria. A simple random sample of 66 AMAs
and 36 ACAs (95% confidence levels, 10% confidence intervals). Ultimately, the AMA sample was
reduced to 63 (that is 45% of AMAs) due to unavailability of information. To ensure consistency
with previous AARs, AMAs for Scholarship Activities were excluded from all comparative
Released
analyses, meaning that comparative analyses are based on an AMA sample of 59.11 The ACA
sample was reduced to 28 (51% of ACAs) for the same reason. The distribution of the samples
according to sectors, programme categories and Whole-of-Life Budget Programme Approvals is
illustrated in Appendix 3.
There were no major changes to the quality reporting system during the review period. The use of
Official
revised AMA and ACA templates, which were introduced in June 2017, is well-established. Most
AMAs (91% of AMAs) and ACAs (75% of ACAs) were completed in the revised templates. Due to
the small number of AMAs and ACAs that were completed in the old templates, an analysis of the
effect of template revisions on the robustness of AMAs and ACAs would not be meaningful.12
8 The previous three AARs were the inaugural AAR, conducted in 2015 for AMAs and ACAs completed between July 2013 and July 2014;
the AAR conducted in 2016 for AMAs and ACAs completed between July 2014 and July 2015, and the AAR conducted in 2018 for AMAs
and ACAs completed between July 2016 and July 2017.
9 The main reason for the differences between selected and reviewed totals is that Activity-related documents could not be provided in time
to be included in the review.
10 Some Activity Managers were responsible for more than one AMA or ACA.
11 The Scholarships Programme completed AMAs for the first time in 2014/15. Four Scholarship Activities were included in the 2016
AAR and eight were included in the previous AAR. The four scholarship activities included in the current AAR sample account for
3% of the AMA sample.
12 Five AMAs and seven ACAs were complete using the old templates.
10

As in previous AARs, AMAs for Scholarship Activities are excluded from the main analysis because
the robustness of scholarships AMAs have typically been significantly lower and have skewed overall
AMA robustness results. In previous AARs, AMAs were prepared for individual Scholarship
Activities. In the current AAR period, the approach to AMAs for the scholarship Activities have been
revised to have a few integrated AMAs focused at a more programmatic level. Therefore, there was
an over-arching AMA prepared for the Scholarship programme, as well as integrated AMAs for all
Scholarship Activities at a country level. There was consistency of assessments and issues across the
four integrated Scholarship AMAs that were reviewed. Therefore, compared to previous AARs, the
influence of scholarship AMAs on the robustness of effectiveness ratings in the current AAR would
have been less evident, but for consistency scholarships activities are excluded.
Assessments
Standard assessment templates for AMAs and ACAs were developed for the inaugural AAR and
slightly amended over previous AARs without compromising comparability with the inaugural AAR.
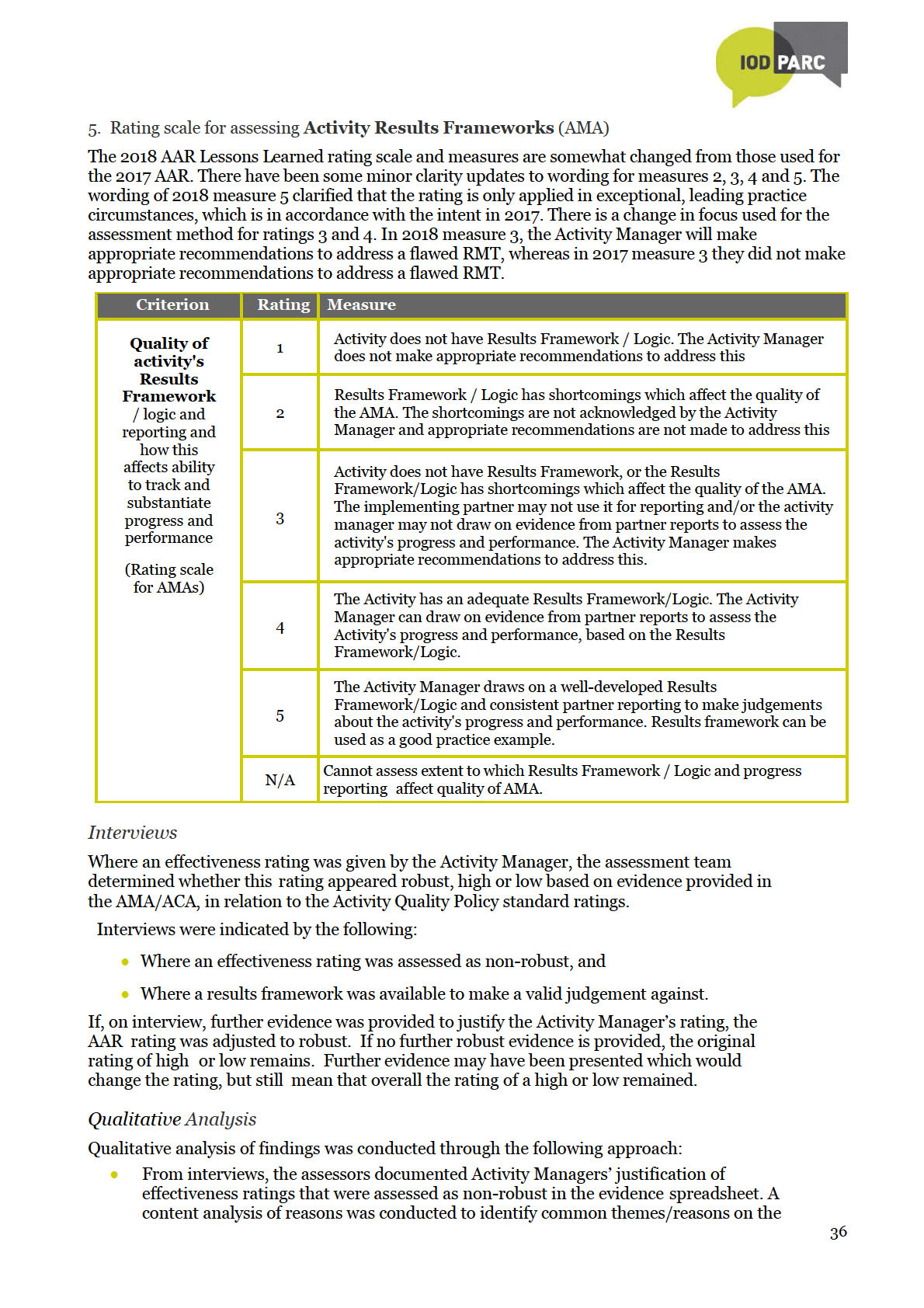
For the current AAR, two revisions were made to templates:
The rating scale for assessing RMTs in the AMA template was re-organised so that ratings
the
reflect a logical increase in quality from a rating of 1 to a rating of 5.
In previous AARs, an overall assessment of AMAs and ACAs focused on quality, based mainly
Act
on the robustness of evidence that informed the completion of the AMA/ACA. In the current
AAR, the overall assessment considered the robustness of evidence, report coherence and the
extent to which this evidence was used to propose helpful actions or lessons to improve
Activities. It considers coherence between identified issues and proposed actions/lessons to
address these issues.
A desk review of the sampled AMAs and ACAs, as well as accompanying partner progress reports,
under
completion reports and the reports of independent evaluations, was conducted to assess the robustness
of effectiveness ratings and, in ACAs, also the ratings for other DAC criteria. The assessment of
robustness is based on the extent to which Activity Managers’ ratings were substantiated by the
evidence and analysis presented in the AMA/ACA, as well as in supporting documentation provided to
reviewers, in accordance with guidance in the Activity Quality Policy (AQP) and in the new AMA and
ACA templates. To have confidence in the robustness of Activity Managers’ effectiveness ratings
across all AMAs and ACAs, MFAT would expect at least 75% of the assessed ratings to be robust.
Non-rated elements of AMAs and ACAs were subject to more qualitative assessments, based on
Information
tailored rating scales. These assessments are not subject to the 75% confident level.
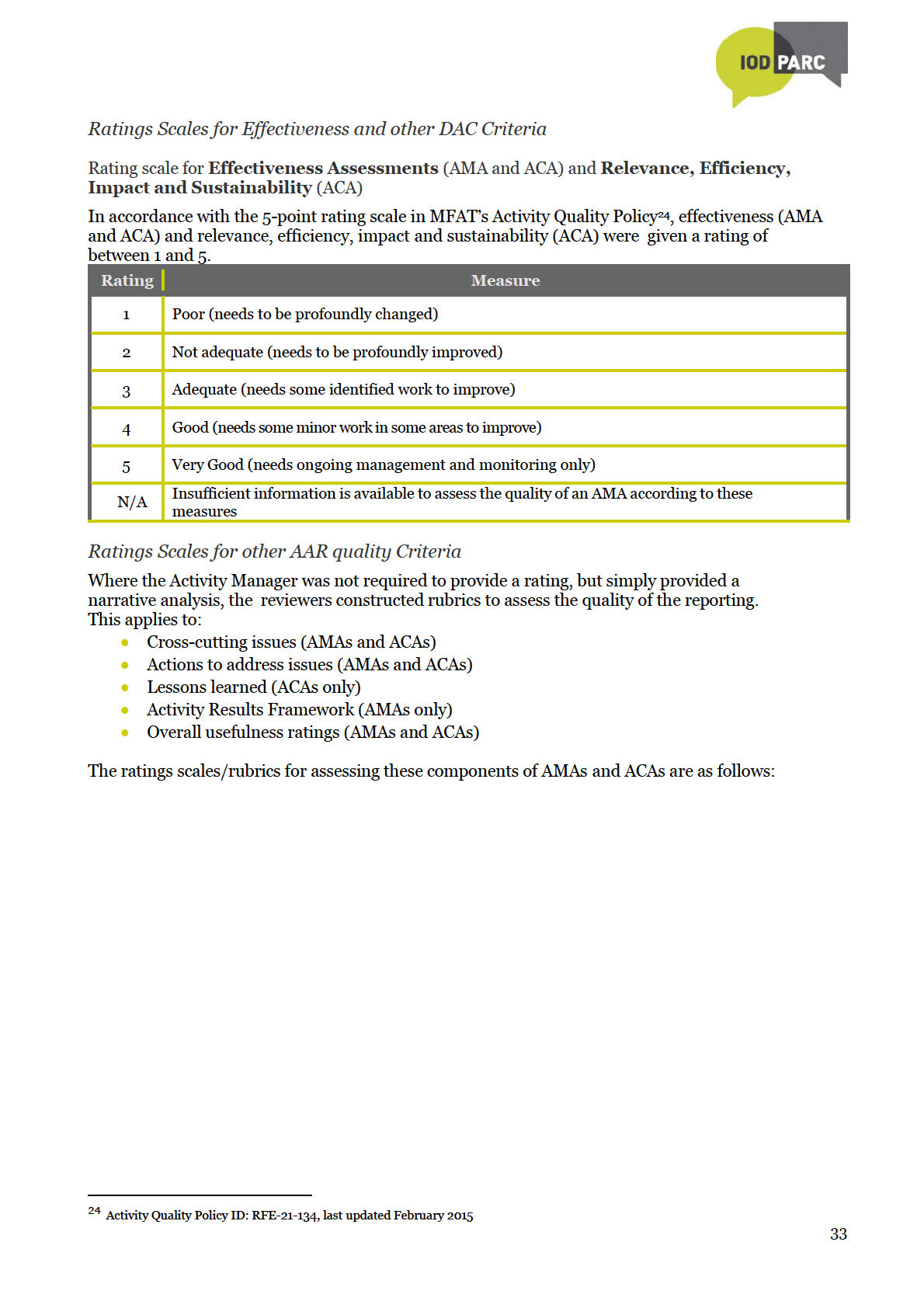
Ratings scales are in Appendix 1, while copies of the assessment templates are in Appendix 5.
Interviews
Released
Effectiveness ratings in 34 AMAs (52%) and 18 ACAs (50%) were initially assessed as non-robust.
Ideally, Activity Managers responsible for all these AMAs and ACAs should have been interviewed
telephonically to clarify the evidence base for the effectiveness ratings. However, only eleven Activity
Managers, covering only one-third of the identified AMAs and ACAs, were interviewed.13 Following
Official
interviews, a final assessment of the robustness of ratings was made.
Interviewing resulted in an increase in the robustness of all effectiveness ratings for both AMAs and
ACAs
(see Table 1). Compared to before interviewing, the percentage of outputs assessed as robust
after interviewing increased by 7% for AMAs and 7% for ACAs. After interviewing, the robustness of
both short-term and medium-term ratings in AMAs increased by 5%, while the robustness of
outcome ratings in ACAs increased by 7%.
Where non-robust ratings were revised to robust after interviewing, Activity Managers could provide
additional information or explanations to justify the ratings they had given. This evidence is not
systematically documented in AMAs or ACAs, for example judgements formed from project visits
and direct interaction with implementing partners and/or partner governments. Contextual
13 Of the 11 interviews that were conducted, four involved discussion of more than one AMA and/or ACA.
11
the Act
under
Information
Released
Official

Limitations of the AAR
1. The AAR is based on selected information on Activity performance. This includes AMAs, ACAs,
the partner report(s) corresponding to the completion dates of AMAs/ACAs, as well as reports of
independent evaluations, where available. Interviews with Activity Managers supplement the
information base for some assessments. Other information that may affect ratings is not
reviewed.
2. Comparisons of actual post-interview effectiveness ratings between the current and previous
AARs should be made with caution.
Both the initial post-interview robustness ratings and the adjusted post-interview ratings have
limitations. The initial post-interview ratings are not informed by a proportional number of
interviews compared to previous years and therefore likely presents and under-estimation of
robustness of effectiveness ratings. The adjusted post-interview ratings are indicative rather than
definitive, but are likely to be closer to what the actual results may have been had a similar
proportion of interviews compared to previous AARs been conducted.
3. The assessment of DAC criteria (including effectiveness) was based on Quality Criteria
the
Considerations outlined in Appendix one of MFAT’s 2015 Aid Quality Policy. However, Activity
Managers likely based their ratings on the AMA/ACA Guidelines revised in 2017. This includes
Act
simplified requirements for Effectiveness, Relevance, Impact, Sustainability and Efficiency, and
Cross-Cutting issues being addressed in the Effectiveness section rather than throughout all
DAC criteria. This could affect the comparability of assessed ratings in the current AAR with
those of previous AARs.
4. The sample size is a representative sample determined at 95% confidence level and a confidence
interval of 10. Decreasing the confidence interval will increase the sample size and reduce the
under
margin of error. This will enable more precise estimates of AAR findings.14 However, for the
2017-18 AAR, confidence intervals have only been calculated for the initial post-interview
ratings and not the adjusted post interview ratings due to potential limitations in the approach.
5. Keeping interviews to 30 minutes each means that they focus on non-robust effectiveness
ratings, as well as four process-related questions. Other non-robust ratings (e.g. for other DAC
criteria in ACAs), or the analyses of CCIs, Lessons and Actions can generally not be discussed
within the available time.
6. The AAR was carried out by two assessors, and pairs of assessors have also changed in
Information
subsequent AARs. Inter-assessor consistency is therefore a potential limitation. This was
mitigated through (1) In-depth orientation and induction of assessors by an experienced Team
Leader, who has been involved in all four AARs to date; (2) Assessor ‘calibration’ following the
assessment of two AMAs and one ACA; (3) Cross-checks and investigation of inconsistent
Released
findings compared to previous AARs; and (4) Independent quality assurance of selected AMAs
and ACAs completed by both assessors.
Official
14 Taking initial outputs ratings in Annex 1 as an example, this means that we can say with 95% certainty that between 41% and 60% of
AMAs will have effective output ratings, no matter how many different samples of the same size we draw form the total number of
AMAs. Another way of saying it is that 51% of AMAs have robust output ratings, with a 19% margin of error. If the sample size is
increased, the confidence interval (and margin of error) will become smaller.
13

3. Key findings
3.1 Robustness of effectiveness ratings
For AMAs, Activity Managers rate effectiveness of Activities separately for outputs, short-term
outcomes and medium-term outcomes. For ACAs, the effectiveness of Activities is rated for outputs,
while a combined rating is given for short- and medium-term outcomes.
The current AAR included an integrated AMA for multiple scholarship Activities, comprising
scholarships for New Zealand based tertiary, Commonwealth, Regional Development
Scholarships and In-Country English Language Training. It incorporated some, but not all the
AMAs in the other three selected scholarship Activities, namely scholarships for Commonwealth,
Regional Development, Pacific Development and Short-Term Training in Niue, Timor-Leste and
Tuvalu, respectively. Compared to the previous AAR, the influence of scholarship AMAs on the
robustness of effectiveness ratings in the current AAR has been similar, although less prominent.
When AMAs for scholarship Activities were excluded from analyses, the robustness of output and
the
short-term outcome ratings increased, while that of medium-term outcomes decreased, but not as
markedly as in the previous AAR.
Act
The quantitative analysis of results is based on the final, adjusted, post-interview assessment of the
robustness of ratings in AMAs and ACAs, excluding AMAs for Scholarship Activities. To be
confident in the robustness of effectiveness ratings, MFAT would expect at least 75% of these
ratings to be robust.
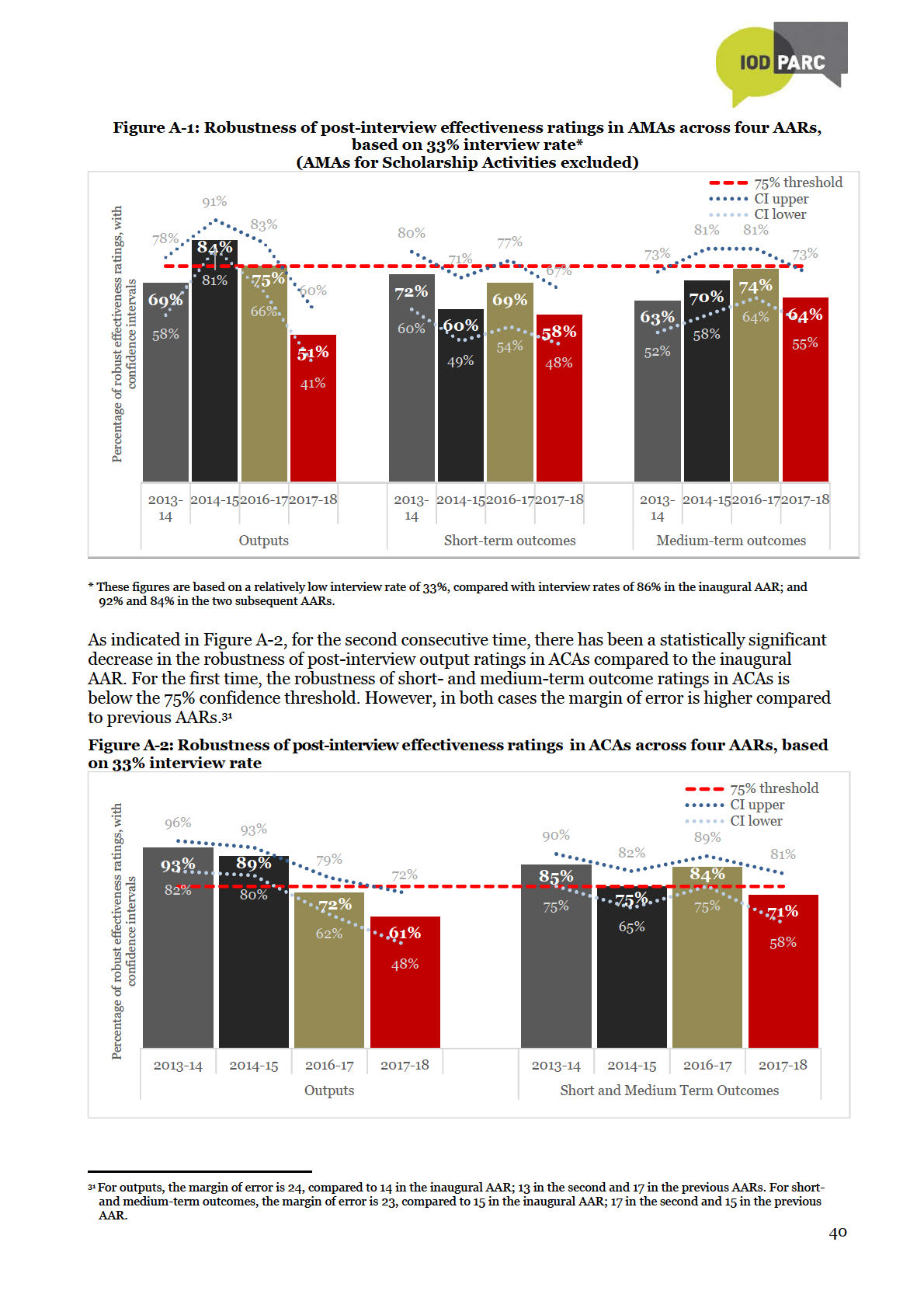
Robustness of effectiveness ratings: AMAs under
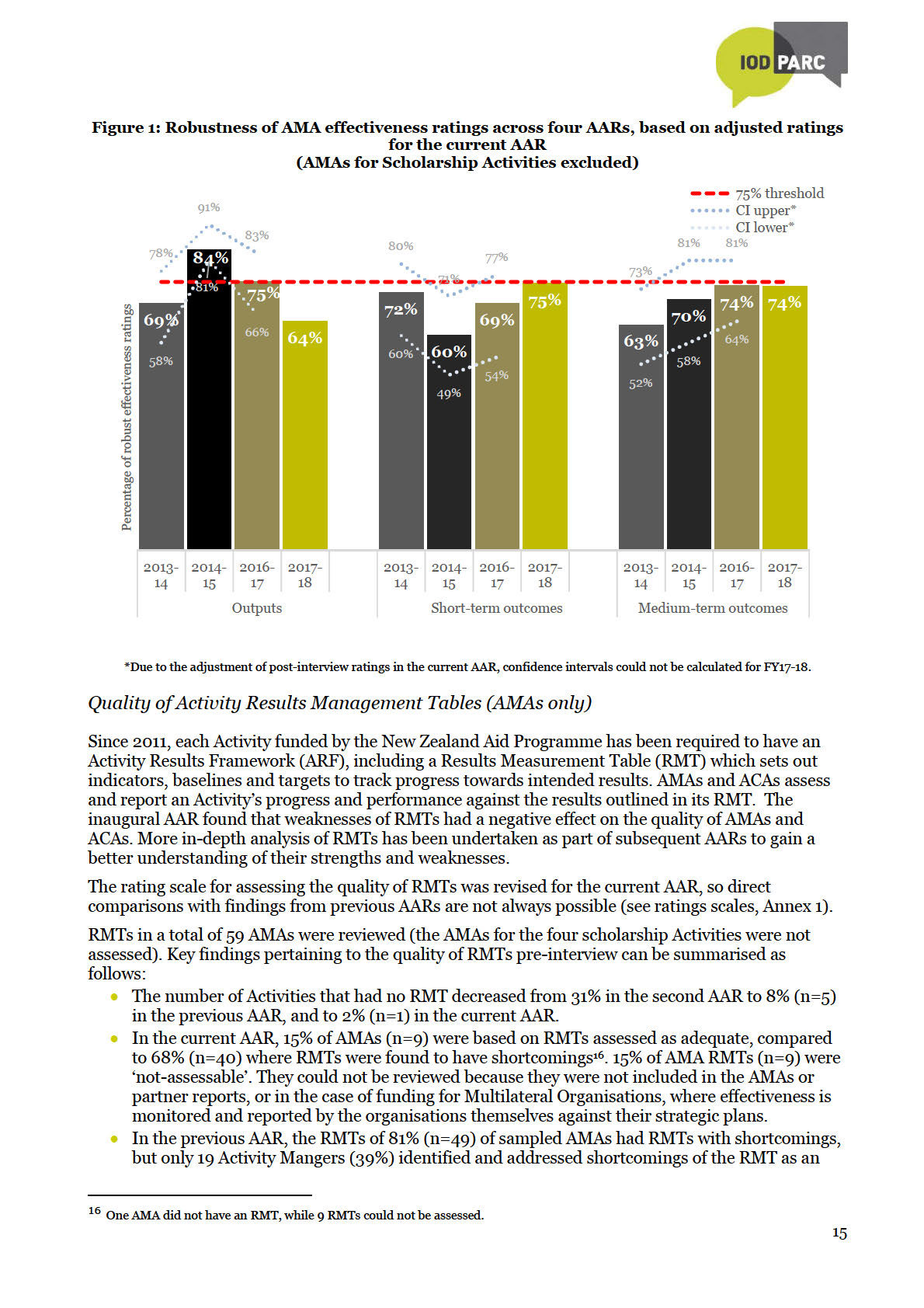
The robustness of output ratings in the current AAR remains below the 75% confidence threshold and
is also lower compared to previous AARs (Figure 1). The robustness of medium-term outcome ratings
would be just below the 75% threshold – higher than the baseline and similar to the previous AAR.
The robustness of short-term outcome ratings would be higher compared to the previous three AARs
and, for the first time, it would meet the 75% threshold.
Assessment of likely statistical significance between the adjusted 2017-18 results and both the
inaugural AAR and the 2016-17 results indicated no statistically significant changes. 15
Information
This suggests that MFAT can be reasonably confident in the robustness of AMA effectiveness ratings.
Released
Official
15 Assessment of statistical significance is limited by availability of detailed data from the inaugural AAR and the adjustment of ratings
applied in 2017-18.
14
the Act
under
Information
Released
Official
the Act
under
Information
Released
Official
the Act
under
Information
Released
Official

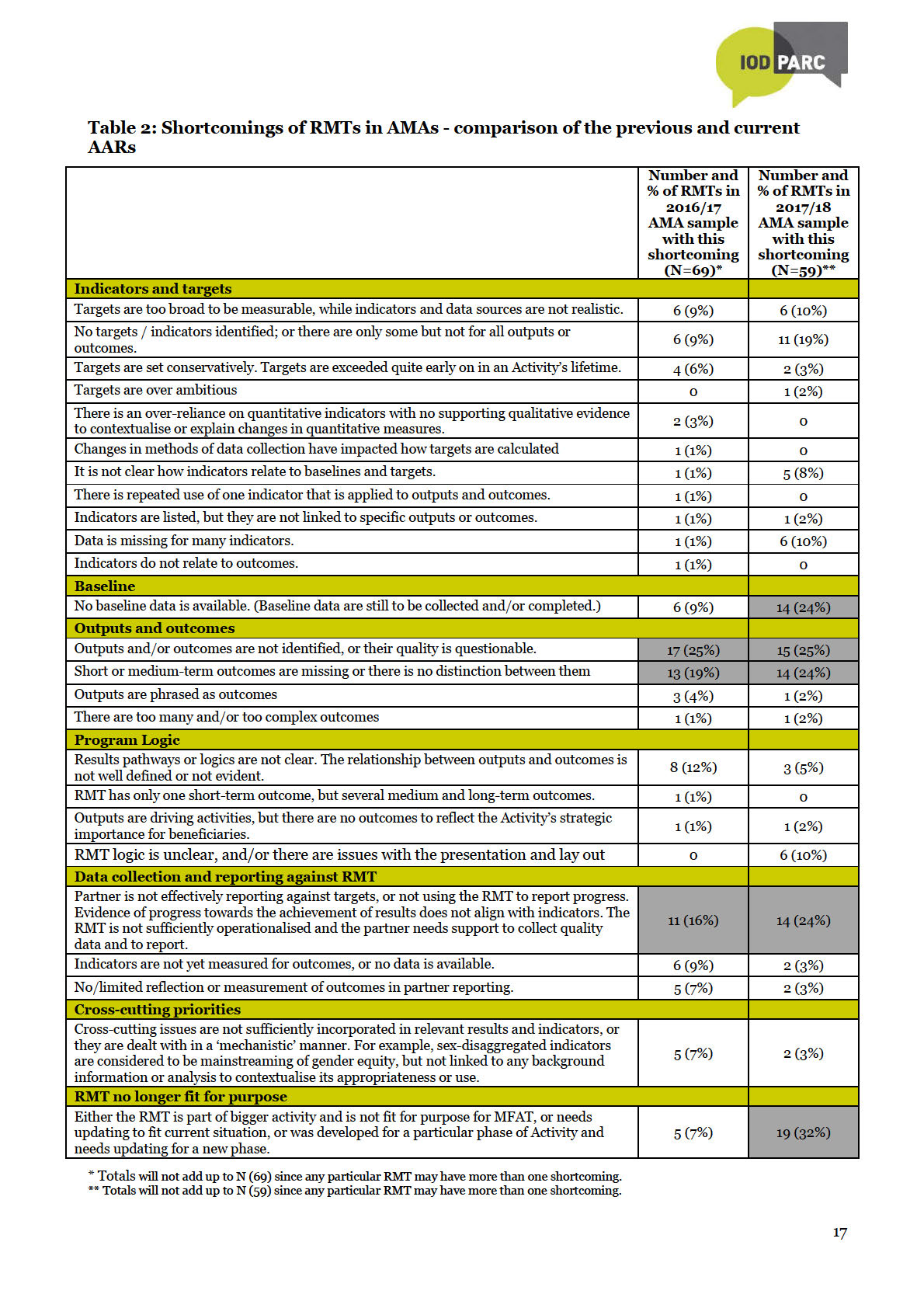
There are some differences in the shortcomings of RMTs found in the current AAR compared to the
previous AAR. In the previous AAR, shortcomings of RMTs were mainly related to Outputs and
Outcomes, e.g. outputs and outcomes were not clearly identified or distinguished; there were too
many, or they were too complex (34 out of 69 RMTs, that is almost half, had such shortcomings).
This was followed by challenges around Indicators and Targets (24 out of 69 RMTs, that is 35%),
with challenges around data collection and reporting against RMT also being common (22 out of 69
RMTs, that is 32%). In the current AAR, most shortcomings were also related to Indicators and
Targets (32 out of 59, that is 54%) and Outputs and Outcomes (31 out of 59, that is 53%). However,
compared to the previous AAR, substantially more challenges were associated with out-of-date
RMTs and RMTs that were no longer fir-for -purpose, as well as shortcomings related to data
collection and reporting. There has also been an increase in the number of RMTs where baseline
data were absent.
In the current AAR, the most common shortcomings relate to outdated RMTs, or RMTs that were no
longer fit-for-purpose (19 out of 59, that is 33%), followed by poorly identified outputs and/or
outcomes (15 out of 50 RMTs, that is 25%, had shortcomings in this regard). In the previous AAR,
the most common specific RMT shortcomings were poorly identified outputs and outcomes, and
poorly distinguished outputs and outcomes (17 out of 69, or 25%, and 13 out of 69, or 19%,
the
respectively). Additional shortcomings noted in the current AAR that were not found in the previous
AAR relate to targets being over-ambitious, lack of overall clarity and inadequate
Act
presentation/layout of the RMT, as well as inadequate accuracy of data/monitoring.
It appears that the development and updating of RMTs to ensure their relevance and use as dynamic
frameworks for monitoring and strengthening Activities on an on-going basis are becoming
increasingly challenging. Also, partner reporting against RMT indicators and targets is also falling
short by a substantial margin. However, it is encouraging that an increasing number of Activity
Managers are proposing appropriate actions to address the identified shortcomings of RMTs – of the
under
40 AMAs that had RMTs with identified shortcomings, 67% included appropriate recommendations
to revise and/or strengthen the Activity’s RMT. This could indicate that more Activity Managers are
realising the value of robust RMTs and are keen to ensure they have fit-for-purpose to monitor
Activities. More robust RMTs would be more useful as Activity monitoring tools and would likely
encourage more coherent partner reporting against expected results.
Training and technical assistance could be instrumental in enhancing the robustness of RMTs.
Special attention could be given to the development and socialisation of RMTs as foundations of
Activity design, as well as dynamic tools for Activity monitoring, reporting and improvement.
Information
Progress reporting for more complex Activities, or for Activities that do not require RMTs per MFAT
policy might require special attention.
Robustness of effectiveness ratings: ACAs
Released
Based on adjusted post-interview effectiveness ratings, the robustness of output ratings is 72% and
that of short-and medium-term outcomes is 77% (see Figure 3). This brings the robustness of output
ratings in line with the 2016-17 AAR (yet still lower compared to the baseline), while the robustness of
short- and medium-term results now exceeds the 75% confidence threshold (but is also still lower
compared to the baseline).
Official
Assessment of
likely statistical significance between the adjusted 2017-18 results and both the
inaugural AAR and the 2016-17 results indicates a potentially statistically significant decrease in the
robustness of output ratings between the inaugural AAR and the current AAR.17
When an Activity ends, it is especially important to know whether it has achieved its results or not. It
is therefore encouraging that MFAT can be reasonably confident about the robustness of short- and
medium-term outcome ratings in ACAs.
17 Assessment of statistical significance is limited by availability of detailed data from the inaugural AAR and the adjustment approach
applied in 2017-18.
18
the Act
under
Information
Released
Official
the Act
under
Information
Released
Official

have a robust RMT, which enabled ratings to be substantiated by reporting against clearly
identified results and indicators. The same applies to nine out of eleven ACAs (82%).
Compared to previous AARs, robust ratings in the current AAR appear to demonstrate greater
confidence in evidence on the part of Activity Managers. Ratings were often substantiated by
references to movements in indictors, or progress in relation to baselines and targets.
In 24 AMAs (excluding scholarship AMAs) and five ACAs, N/A effectiveness ratings were
assessed as robust – this means that the reviewers agreed that an Activity’s effectiveness could
not be rated. Reasons for this included:
Shortcomings of RMTs. In 17 AMAs (including AMAs for Activities involving Multilateral
Organisations and those funded through Budget Support, as well as multi-country and multi-
donor Activities) and two ACAs (including one Humanitarian Response Activity), the absence
or shortcomings of RMTs made it impossible to assess effectiveness.
In five of 24 AMAs (21%), it was too early to assess progress towards outcomes.
In seven of 24 AMAs (29%), there was no data/evidence available to assess effectiveness,
including three AMAs where baseline data were not yet available. Effectiveness in four ACAs
could not be assessed due to lack of data/evidence.
the
3.2 Robustness of other DAC criteria ratings (ACAs only)
Act
The assessed robustness ratings for the DAC criteria of relevance, efficiency, impact, sustainability in
ACAs is based on desk reviews, as interviews focused on effectiveness ratings. Had the DAC ratings
been discussed further at interview, there may have been some increase in their robustness in line
with increases seen in previous AARs, where the ratings of these criteria were discussed during
interviews.
under
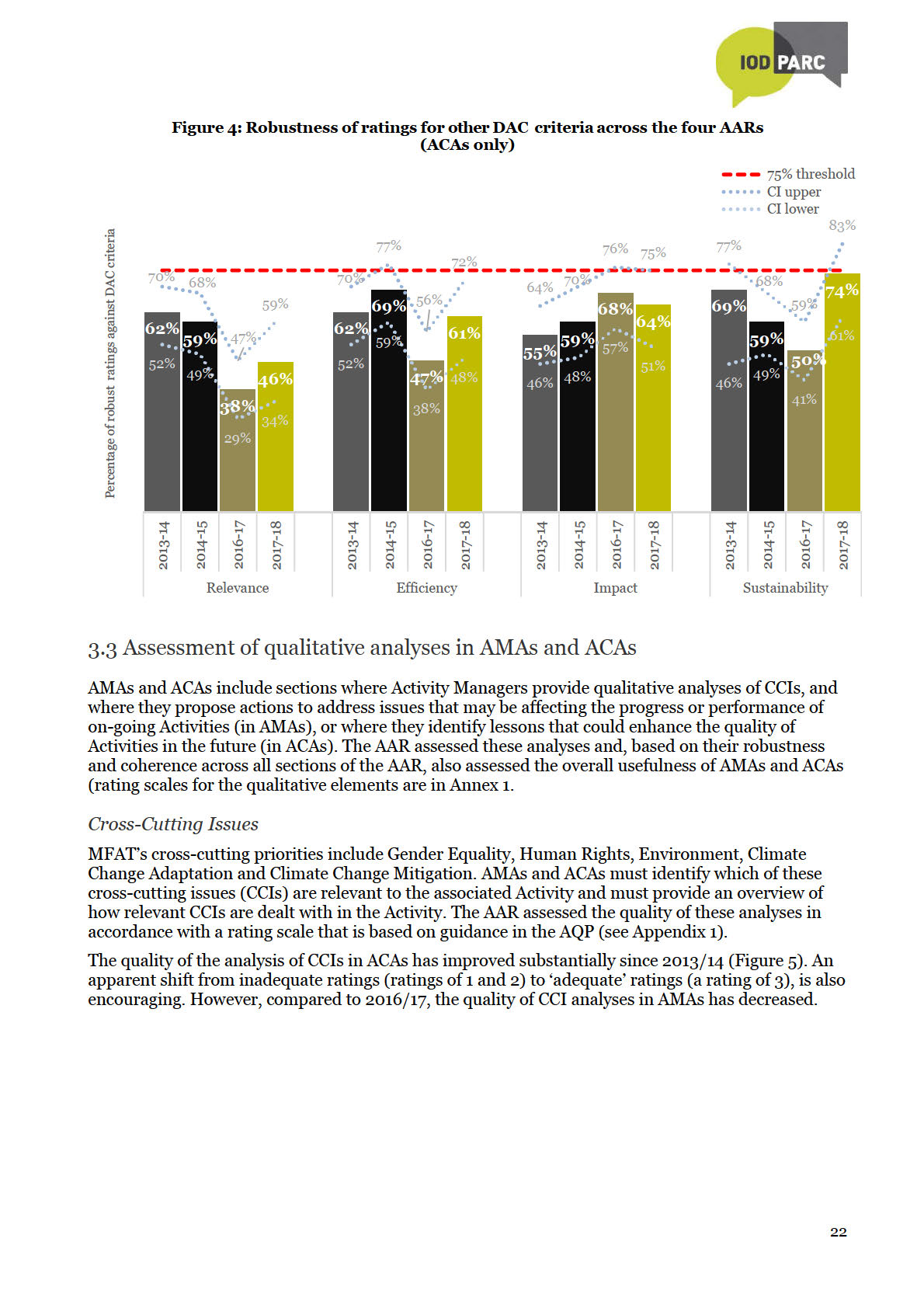
The comparative robustness of ratings for the DAC criteria across the four AARs is shown in Figure
4. Compared to the baseline (inaugural AARs), the robustness of sustainability and impact ratings
has increased. While that of efficiency has decreased by only one per cent, the robustness of
relevance ratings has decreased by 16%. No rating has yet reached the MFAT confidence level of
75%. Bearing in mind that that ratings of these criteria were not discussed during interviews, and
despite encouraging increases in robustness of sustainability and impact ratings, MFAT cannot use
the ratings of other DAC criteria in ACAs with confidence to inform decision-making.
The main reason for non-robust relevance ratings is that they do not address all considerations
Information
outlined in the 2015 AQP, against which they were assessed. However, MFAT staff may have,
appropriately, based their response on the AMA and ACA guideline
Activity Quality Ratings for
Completion Assessment revised in 2017, which is not consistent with the 2015 AQP. Key changes
include: simplified requirements for Relevance, Impact, Sustainability and Efficiency, and Cross-
Released
Cutting issues being addressed in the Effectiveness section rather than throughout all DAC criteria.
Therefore, aspects such as the relevance of modality and the mainstreaming of cross cutting issues
across all criteria, are of lesser importance.
A likely result of this would be an increase in the number (and proportion) or robust relevance,
efficiency, impact and sustainability ratings – and the robustness of sustainability ratings would
Official
likely exceed the 75% confidence threshold. Reviewers based their assessment of the robustness of
these ratings on a number of considerations that are no longer included in the revised guidance. Had
assessments been based on the revised guidance, more ratings may have been assessed as robust.
21
the Act
under
Information
Released
Official
the Act
under
Information
Released
Official
the Act
under
Information
Released
Official
the Act
under
Information
Released
Official
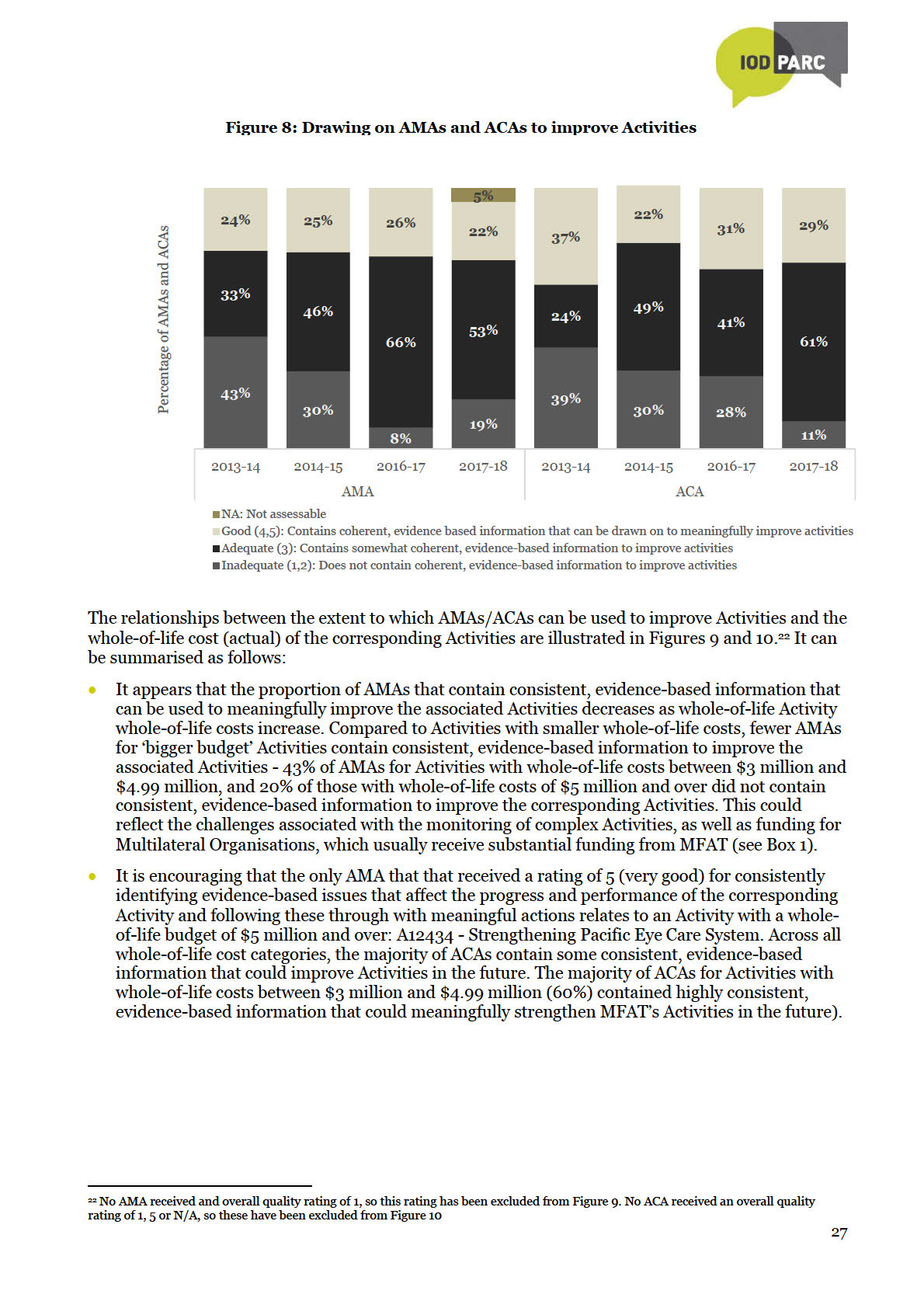
 Drawing on AMAs and ACAs to improve Activities
Drawing on AMAs and ACAs to improve Activities
The extent to which AMAs and ACAs can be drawn on to improve Activities depends on whether they
are based on evidence from more than one source (regardless of the robustness of effectiveness
ratings); whether they tell a coherent, evidence-based story of progress; and whether they
consistently identify meaningful actions (AMAs) or
Box 2
lessons (ACAs) to inform the improvement and future
2017/18 AMAs on strengthening
planning of Activities (rating scales are presented in
Scholarship Activities
Appendix 1).
When assessed separately, all four
Figure 8 suggests that there could be reason to be
scholarship AMAs in the current AAR
more confident in drawing on AMAs and ACAs to
refer to actions that could strengthen
improve Activities:
monitoring, reporting and AMAs for
scholarship Activities in the future. This
The percentage of AMAs that received an overall
includes the development of a revised
rating of 1 or 2 (meaning they do not contain
RMT for scholarship activities, which
consistent, evidence-based information to improve
was being undertaken as part of a
the associated Activity) decreased from 43% in the
strategic evaluation of the scholarship
inaugural AAR to 19% in the current AAR; that is a
programme. The evaluation was
the
decrease of 24%.
underway at the time the AMAs were
being drafted. The three country
Act
The percentage of AMAs that received overall
scholarship AMAs also refer to a tracer
ratings of 4 and 5 (meaning that they contain highly
study that was underway at the time the
consistent, evidence-based information to improve
AMAs were being drafted, as well as the
the associated Activity) shows small decreases
alumni strategy and a new Scholarships
across successive AARs. In the current AAR, 22% of
and Alumni Management System (SAM),
AMAs received a rating of 4 or 5, which is a
which are expected to strengthen
monitoring and reporting against
under
decrease of 2% compared to the inaugural AAR.
medium-term outcomes. It would be
This coincided with an increase of 20% in the
important to monitor the effect of these
proportion of AMAs that contain fairly consistent,
initiatives on the robustness and quality
evidence-based information to improve the
of scholarship AMAs in the future.
associated Activities increased by 20% - up from
33% in the inaugural AAR to 53% in the current
AAR. This indicates that the proportion of AMAs that cannot be drawn on to improve Activities is
decreasing in favour of those that can be drawn on to improve Activities, although there is room
for improvement.
Information
Over time, the proportion of ACAs that does not contain consistent, evidence-based information
to improve Activities has reduced substantially (from 39% in the inaugural AAR to 11% in the
current AAR – therefore a decrease of 28%), but the proportion provides highly consistent,
evidence-based information to improve Activities has also decreased somewhat (from 37% to
Released
29% - therefore a decrease of 8%). The proportion that provides fairly consistent, evidence-based
information to improve Activities has increased by 37% - up from 24% in the inaugural AAR to
61% in the current AAR. This indicates that the vast majority of ACAs contain some information
that could meaningfully be used to improve Activities in the future.
Official
26
the Act
under
Information
Released
Official
the Act
under
Information
Released
Official

4. Summary of Findings
1. Anecdotally, interviews with Activity Managers conducted as part of the current AAR revealed
that they have a positive attitude about AMAs and ACAs, as well as a good understanding and
appreciation of their value. Fewer Activity Managers regard the completion of AMAs and ACAs as
a compliance requirement and there was a clear sense that more Activity Managers view the
completion of AMAs and ACAs as important opportunities to reflect analytically on the progress,
performance and challenges of Activities and their on-going improvement. This is substantiated
by relatively high AMA and ACA completion rates.
2. Using the adjusted post-interview robustness ratings, in AMAs, the robustness of output and
medium-term outcomes ratings is lower compared to previous AARs, but the robustness of short-
term outcome ratings is higher, reaching the 75% confidence threshold. In ACAs, the robustness
of short- and medium-term outcomes is just above the 75% confidence threshold.
3. References to RMTs as sources of evidence for completing AMAs and ACAs are increasing,
indicating that Activity Managers are increasingly relying on RMTs to keep track of Activities’
the
progress. The quality of RMTs appears to be improving. However, shortcomings of RMTs
continue to hamper monitoring and reporting of results. Many RMTs are not updated and are no
Act
longer adequate to monitor progress of evolving Activities. Other major shortcomings of RMTs
include the absence of baselines, targets and data to monitor and report progress.
AMAs of funding for Multilateral Organisations appear to be especially challenging because the
results frameworks and progress reporting of these Organisations do not always correspond to
MFAT’s requirements. It appears that developing AMAs and ACAs for complex Activities, for
example multi-county and multi-donor Activities, as well as Activities funded through Budget
under
support could also be challenging because RMTs for these Activities are not straight-forward.
It is encouraging that an increasing number of Activity Managers are proposing appropriate
actions to address the identified shortcomings of RMTs.
4. The identification and analysis of Cross-Cutting Issues remain a challenge for Activity Managers.
Although the quality of analysis of CCIs in both AMAs and ACAs is showing improvement, the
proportion of these analyses that received ‘good’ or ‘very good’ ratings remains small. There was
also an increase in the proportion of AMAs and ACAs where CCI analyses received N/A ratings,
suggesting that there either were no cross-cutting priorities identified in the AMA or ACA (i.e. CCI
Information
is classified as ‘not measured’ or ‘not targeted’), or there was very limited or no further elaboration
on CCIs in the document..
5. Observed improvements in the quality of more analytical aspects of AMAs and ACAs are
Released
encouraging. Compared to the baseline, the proportion of ACAs that identified well-
substantiated, useful lessons increased by 19%, while proportionately more AMAs are shifting
from ‘inadequate’ to ‘adequate’ quality as far as the identification of actions to strengthen
Activities is concerned.
6. There is reason to be cautiously confident in the overall usefulness of AMAs and ACAs. The
Official
majority of AMAs and ACAs are of adequate usefulness. The proportions of AMAs and ACAs that
are of inadequate usefulness have decreases substantially compared to the baseline – by 24% in
the case of AMAs and by 20% in the case of ACAs. These appear to have shifted mainly from
‘inadequate’ to ‘adequate’ usefulness. However, a small proportion of AMAs and ACAs appear to
be slipping back from ‘good’ to ‘adequate’ usefulness.
5. Conclusions
1. Despite improvements in qualitative aspects of reporting, AMAs and ACAs still do not provide
sufficiently accurate, complete or stand-alone records of the activity. As in previous AARs,
Activity Managers draw on evidence from a range of sources to assess the effectives of Activities
but tend not to document all this evidence in AMAs and ACAs. If evidence is not comprehensively
29

documented, the loss of institutional knowledge leaves substantial gaps, especially where staff
turnover is high. When these gaps build up year-on-year, new Activity Managers might find it
challenging to complete insightful AMAs and ACAs, thereby jeopardising the robustness of AMAs
and ACAs in the longer term.
2. Despite remaining challenges around the robustness of effectiveness ratings, AMAs and ACAs
generally include some consistent, evidence-based information that could be drawn on to improve
Activities. Providing useful information to improve complex Activities, which often have high
whole-of-life costs, are challenging since ways that could improve these Activities may not be
within MFAT’s full control.
3. So far, AARs have not revealed major statistically significant results related to AMA and ACA
improvement over time. Some trends are beginning to emerge, while valuable lessons have
contributed to a much-refined methodology. While MFAT does not expect linear improvement
due to contextual factors such as organisational capacity and incentives, over a longer time period
statistically significant changes may become evident.
6. Recommendations
the Act
1. AMAs and ACAs should remain as essential building blocks of the Aid Programme’s performance
management system. Activity Managers use AMAs and ACAs to reflect and assess the progress,
performance and challenges of Activities and they serve as important repositories of institutional
memory and continuity during Activity implementation. Increasingly insightful and usable
lessons and actions to address issues, if harnessed through a robust knowledge management
system, could also prove valuable in strengthening Activities.
under
2. Ongoing training and technical support would be important to ensure that gains made in the
robustness and usefulness of AMAs and ACAs are maintained and enhanced. Gradual
improvements are becoming evident, but it would be important to address known challenges and
strengthen capacity to maintain this positive momentum and to prevent the gains made from
being lost.
Continue to provide training and guidance for Activity Managers in Wellington and at Post
(including locally-engaged staff) to ensure that they understand why and how to document the
evidence base for AMAs and ACAs fully, yet concisely, to increase the proportion of AMAs and
Information
ACAs that provide stand-alone records of Activities’ progress and performance. This would be
instrumental to lift the robustness and usefulness of AMAs and ACAs (and therefore their value
as essential building blocks of the Aid Programmes performance management system) to a
higher level. Released
Training and support in the following priority areas could be considered:
Documenting consolidated evidence from several sources to justify effectiveness and
DAC criteria ratings.
RMT quality and wider socialisation of RMTs as foundations of Activity design,
Official
monitoring and reporting, as well as dynamic tools for Activity improvement.
MERL expert assistance to support regular reviewing and updating of RMTs to ensure
that they remain relevant and up-to-date.
Strengthening RMTs and monitoring of complicated and complex Activities, for example
multi-donor and multi-country Activities, as well as Activities funded through budget
support.
Improving consistency and coherence in AMAs and ACAs, including identifying issues
that affect the progress and performance of Activities, and following this through into
meaningful, evidence-based issues to improve on-going activities (in AMAs), or lessons
relevant to comparable types of Activities when they complete ACAs.
30

3. Given the size of MFAT’s funding to Multilateral Organisations and the unique arrangements
around their monitoring, it could be beneficial to tailor guidance for the AMAs of these Activities.
4. Provide support to Activity Managers to identify and perceptively address appropriate Activity
cross-cutting markers:
Where a cross-cutting marker is identified as relevant, it should be dealt with
consistently and perceptively throughout the design, monitoring and reporting of the
activity, including in AMAs and ACAs.
Avoid including cross-cutting markers that are not relevant to an Activity in its
AMA/ACA.
5. AARs should continue to be conducted on a periodic basis to monitor the effect of known
enablers and constraints to the robustness and usefulness of AMAs and ACAs, as well as to
identify emerging challenges and actions for their continuous improvement. A larger database
will also enable meaningful trend analyses of the robustness and usefulness of AMAs/ACAs
across different sectors, programmes and budget levels.
the
Act
under
Information
Released
Official
31
the Act
under
Information
Released
Official
the Act
under
Information
Released
Official
the Act
under
Information
Released
Official
the Act
under
Information
Released
Official
the Act
under
Information
Released
Official

basis of which the final rating was decided. Each reason was then coded to a common
theme/reason and a frequency analysis of theses/reasons was conducted.
Information on Activity’s Managers’ process when completing AMAs/ACAs, their
opinion of the AMA/ACA templates and guidance, their view of the robustness of
evidence available to inform the completion of AMAs and ACAs, as well as which
aspects of AMAs/ACAs they found especially challenging (and why) was documented. A
content analysis of the documented information was conducted to identify
commonalities and emerging themes.
Sample Revision for AAR Quantitative Analysis
Quantitative Analysis
Comparative assessments of results between the four AARs was completed. Robustness of
effectiveness ratings at output, short term outcome, medium term outcome for AMAs and ACAs
as well as relevance, efficiency, impact and sustainability for ACAs was compared and presented
in charts. For the remaining criteria (Cross-cutting issues (AMAs and ACAs) , Overall quality
ratings (AMAs and ACAs), Actions to address issues (AMAs only), Activity Results Framework
the
(AMAs only), and Lessons learned (ACAs only)), the assessed ratings were compared by
Act
percentage and presented in charts for inadequate (rating of 1 or 2), adequate (rating of 3) and
good (rating of 4 or 5).
N/A Ratings
N/A ratings were removed from the observed proportion to enable the calculation of robustness.
Scholarships Programme
under
Scholarships Activities were introduced to the AAR process in 2016 (AMAs for 2014-15) and have a
notable influence on the overall robustness of AMA effectiveness ratings. For purposes of
comparability across all four AARs, assessments of the robustness of AMAs in this report
consistently exclude Scholarship Activities unless noted otherwise.
Statistical Analysis of results
The Wilson score method was used to construct initial confidence intervals26:
Information
In this calculation n is the sample size, p is the observed proportion, q=1‐p and z is the quintile of the
standard normal distribution which depends on the desired level of confidence. For 95% confidence
Released
intervals, as is the case in this instance, z is 1.96. Using the same formulas as in previous AARs27,
these were the adjusted using the ‘finite population correction’ method referenced by Burstein28 to
construct confidence intervals with more accurate coverage probability given the small population
sizes. This approach enables the nominal coverage of 95% to be maintained while narrowing the
confidence intervals.
Official
To determine
statistical significance of differences in findings between the inaugural and 2017-
18 AAR and the 2016-17 and 2017-18 AAR, the Z test based on normal approximation in two finite
populations was used29. It was possible to conduct statistical analyses when a rating was applied by
26 Newcombe, R.G. (1998) Two‐sided confidence intervals for the single proportion: comparison of seven methods. Stat. Med. 17, 857‐872.
27 Wilson’s method alone was used for the inaugural 2015 AAR report (2013-14 results). The 2016 AAR report (2014-15 results) used the current
combination of Wilson overlaid with the FPC method referenced in Burstein; the 2013-14 results were revised accordingly for comparison. See 2016
AAR Report for further detail.
28 Burstein. H (1975), Finite Population Correction for Binomial Confidence Limits, Journal of the American Statistical Association, Vol. 70, No.
349 (Mar., 1975), pp. 67- 69; Rosenblum, M, van der Lann. M.J (2009) Confidence Intervals for the Population Mean Tailored to Small Sample
Sizes, with Applications to Survey Sampling, Int. J Biostat 5(1):4
29 Krishnamoorthy K and Thomson J. Hypothesis Testing About Proportions of Two Finite Populations. The American Statistician, Vol 56, No 3
(August 2002), pp 215-222.
37
the Act
under
Information
Released
Official
the Act
under
Information
Released
Official
the Act
under
Information
Released
Official
the Act
under
Information
Released
Official
the Act
under
Information
Released
Official

Appendix 3: Distribution of sample
The following figures profile some of the key descriptors for the AMA and ACA samples:
Number of AMAs by Sector
Agriculture/Forestry/Fishing
15
Government & Civil Society
7
Education
5
Economic Governance
5
Agriculture
5
Transport & Storage
4
Health
3
Water Supply & Sanitation
2
the
Unspecified / Multi
2
Act
Reconstruction relief and rehabilitation
2
Other multisector
2
Law and Justice
2
Humanitarian Response
2
Trade / Tourism
1
Resilience
1
under
Popuation Policies/Programmes &…
1
Emergency Assistance
1
Communications
1
Business & Other Services
1
Banking & Financial Services
1
Information
Number of ACAs by Sector
Health
4
Released
Resilience
3
Agriulture/Forestry/Fisheries
1
Agriculture
4
Other Multisectoral
2
Governance
2
Official
Education
2
Banking & Financial Services
2
Water Supply & Sanitation
1
Trade and Labour Mobility
1
Renewable Energy
1
Humanitarian Response
1
Environment
1
Economic Governance
1
Business & Other Services
1
43
 Number of AMAs by Programme
Number of AMAs by Programme
Solomon Islands
6
ASEAN Regional
6
Multilateral Agencies
5
Kiribati
5
Scholarships
4
Vanuatu
3
Partnerships and Funds
3
Pacific Human Development
3
Pacific Economic
3
Niue
3
Indonesia
3
Fiji
3
Papua New Guinea
2
Pacific Regional Agencies
2
Latin America and the Caribbean
2
Humanitarian & Disaster Management
2
Tonga
1
the
Tokelau
1
Timor Leste
1
Act
Pacific Transformation Fund
1
Pacific Energy & Infrastructure
1
Myanmar
1
Economic Development - ED
1
Africa
1
under
Number of ACAs by Programme
Partnerships and Funds (contestable)
6
Latin America & the Caribbean
3
Papua New Guinea
2
Other Asia
2
Information
Niue
2
Multilateral Agencies
2
Fiji
2
Released
Tonga
1
Vanuatu
1
Solomon Islands
1
Samoa
1
Pacific Human Development
1
Official
Pacific Economic Development
1
Humanitarian & Disaster Management
1
Economic Development - ED
1
Africa Regional
1
44
 Number of AMAs and ACAs according to Whole-of-Life Budget Programme Approval*
Number of AMAs and ACAs according to Whole-of-Life Budget Programme Approval*
AMAs
ACAs
$ 5 million and over
31
$ 5 million and over
6
$3 million - $4.99
$3 million - $4.99
8
5
million
million
$1 million - $2.99
$1 million - $2.99
16
6
million
million
$500,001 - $999,999
3
$500,001 - $999,999
7
the
< $ 500,000
3
< $ 500,000
3 Act
*The Whole-of-Life Budget Programme Approvals for three AMAs and one ACA were not available
under
Information
Released
Official
45
the Act
under
Information
Released
Official
the Act
under
Information
Released
Official
the Act
under
Information
Released
Official
Appendix 6: Interviewing script
INTRODUCTORY SCRIPT - MFAT Annual Assessment of Results (AAR) 2018
Thank you for agreeing to speak with me today.
As you will have been advised by the Development Strategy and Effectiveness team, I have been
involved in a review of a sample of AMAs and ACAs to determine the robustness of self-assessed
performance ratings in these reports. This year my colleague and I are reviewing 66 AMAs and 36
ACAs (102 in total) that were randomly selected from a total of 196 AMAs and ACAs submitted
between July 2017 and July 2018.
We would specifically like to discuss the ratings given against the effectiveness criteria – these are
the ratings provided for achievement of outputs, short-term outcomes and medium-term outcomes.
We will aim to keep the interview to 30 minutes (longer if more than one AMA or ACA will be
the
discussed). Time allowing, we may also briefly discuss assessments and ratings provided for other
performance criteria, as well as your experience of the tools, guidance and support available to
Act
complete AMAs and ACAs.
The primary documents reviewed for our analysis are the AMAs/ACAs themselves, as well as the
corresponding partner report. We assessed whether or not the effectiveness ratings given appear
‘robust’ on the basis of the evidence and analysis presented in the AMA/ACA and the partner report.
Where further information and clarification are required, we have the option to speak with Report
under
Authors (Activity Managers) and/or Deputy Directors in order to gain further insight into the
evidence and considerations underlying the given ratings.
I asked to speak with you today because I need a deeper understanding of how you arrived at some
of the ratings in the following report/s (list here)
Before we begin the discussion, I would like to assure you that the discussion will be
Information
Strictly confidential. Individual AMA/ACA reports will not be identifiable in the Annual
Assessments of Results (AAR) report. All findings will be presented as percentages of the
sample, and aggregated for smaller programs. Any comments from interviewees that are
included in the report will be anonymous. Assessment and interview records will be stored
securely by the Development Strategy and Effectiveness team and it will not be used for any
Released
purpose other than do inform the AAR.
The AAR process will not result in a change to the original ratings in the MFAT system. The
assessors are not tasked to recommend any changes to the ratings in individual AMAs/ACAs.
Our main aim is to understand the process and quality of evidence that informed the ratings.
Official
At the end of the interview, feedback on the independent assessment can be provided to Program
Managers/Activity Managers by the interviewers, if required/requested. This feedback will be
provided in general terms, that is, indicating the strengths/weaknesses of the AMA/ACA against a
suite of agreed criteria against which it was assessed.
Now, to confirm, we are discussing (Activity number and name – if more than one, take them one at
a time)
Questions on criteria:
To be inserted by interviewer based on desk assessment.
Focus on effectiveness ratings that were assessed as non-robust. Time allowing, then discuss
ratings for other criteria that were also assessed as non-robust.
49
Clarify evidence and interpretation of evidence to understand whether original rating is
robust or not.
In a separate row directly below the original assessment in the assessment template, indicate
what the assessed rating is after interviewing and motivate why, if it has changed from the
rating given at the time of the desk assessment (e.g. “The Activity Manager conducted a site
visit and provided information from this visit to justify the original rating. This information
was not documented in the AMA/ACA. Based on this information, the reviewer agrees with
the Activity Manager’s original rating – it is robust”).
If the Activity Manager cannot justify his/her original rating based on all available
information, then you may want to ask about his/her interpretation of the evidence which led
you to assess the original rating as non-robust. This is not about defending your assessment.
It is about allowing the Activity Manager to contextualise and explain that information,
which may lead you to reconsider your assessment of the original rating, or not. This is not to
be debated with the Activity Manager. Simply record your final rating and the justification for
it, and move on to the next item.
Questions on Process for completing AMAs/ACAs:
the
Can you describe the process you went through to develop the AMA/ACA? Act
Do you find the guidance and templates helpful? Any suggestions to improve them?
Did you receive any training or support from the Insights, Monitoring & Evaluation team on
how to complete AMAs/ACA? Did you find it helpful? Any suggestions to improve it?
In your view, do you have sufficient robust evidence/data to inform the AMA/ACA process?
(You could prompt about the timeliness and quality of partner reports; opportunities for site
visits, etc.)
under
Are there any particular aspects of AMAs and ACAs that you find especially challenging?
What are they? Why do you find them challenging? (Prompt for specific aspects, e.g.
mainstreaming of cross-cutting issues, VFM)
Information
Released
Official
50