Document One
Terms of Reference –
COVID-19 Testing
Technical Advisory Group
under the Official Information Act 1982
25 August 2021
Released
Document One
Contents
Introduction ..................................................................................................................................................................................... 3
Context ............................................................................................................................................................................................... 3
Purpose and Function .................................................................................................................................................................. 4
Membership ..................................................................................................................................................................................... 5
Duties and Responsibilities ........................................................................................................................................................ 6
Meeting protocols ......................................................................................................................................................................... 8
Fees framework ................................................................................................................................................................... ... ... 9
Review of Membership ........................................................................................................................................... . ............... 9
under the Official Information Act 1982
Released
Document One
Introduction
The Ministry of Health (the Ministry) is the kaitiaki of the health and disability system in Aotearoa New Zealand and the
principal health advisor to Government. We do this by providing a fair, effective, and sustainable system and advice that
people can trust. The Ministry is responsible for providing active stewardship and leadership across the health and
disability system to ensure it provides people with the highest level of care, regardless of who they are or where they
live.
The COVID-19 pandemic has rapidly evolved internationally and in Aotearoa New Zealand. Responding to COVID 19 in a
very rapidly changing environment is a significant ongoing challenge.
The Government's overall public health strategy in respect of the COVID-19 pandemic affecting New Zealand is
elimination. That is, to apply a range of control measures to stop the transmission of COVID-19 in Aotearoa New Zealand.
There are four pillars to our elimination strategy, these are:
• Keep it out (pre- and border settings, managed isolation and quarantine)
• Prepare for it (robust case detection and surveillance, and public health measures)
• Stamp it out (effective contact tracing and case management, and stronger public health measures)
• Manage the impact (health system readiness and resilience)
The Ministry has established the COVID-19 Health System Response Directorate (the Directorate) to give effect to the
elimination strategy. The Ministry is working to ensure the response to COVID-19:
• is evidence-based
• is consumer-centred
• is equity-focussed and guided by the Treaty of Waitangi
• effectively manages clinical and public health issues and risks
• supports an open and transparent culture
• has a continuous quality improvement and safety focus
• monitors and reviews clinical processes and outcomes
• guides the development of the Ministry and All of Government strategies to address COVID-19.
Context under the Official Information Act 1982
On 24 June 2021, Sir David Skegg, Chair of the Strategic Public Health Advisory Group recommended that the
government establish an expert committee to advise on the suitability of the current approach to COVID-19 testing
within New Zealand and how this approach should evolve in response to new testing technologies, where appropriate.
In particular, the approach to reconnecting Aotearoa New Zealand, will pose new paradigms, which will require the
Released
broad range of expertise obtained through engagement with the COVID-19 Testing Technical Advisory Group.
Document One
Purpose and Function
The COVID-19 Testing Technical Advisory Group (CT TAG) will provide rapid, independent, and practical advice to the
Director-General of Health on testing technologies and paradigms, to inform New Zealand’s COVID-19 response and the
work to reconnect Aotearoa New Zealand to the world. CT TAG members will be asked to advise and give expert
oversight on:
a)
assessment of the benefits and limitations of new testing technologies and paradigms for New Zealand,
including the suitability of new technologies in different settings and scenarios
b)
comparison of new technologies to those currently in use
c)
technical guidance on the expected timeframe for adopting a new technology
d)
horizon-scanning to identify technologies being developed locally and overseas
e)
the application of new technologies to assist in reconnecting New Zealand, including their use in border
management, and managed isolation and quarantine settings
The group’s advice will assist the Ministry and Government to:
a)
Ensure that the COVID-19 surveillance strategy and testing guidance is fit-for-purpose for the goals of the
elimination strategy or any future pandemic response strategy as it may be adopted.
b)
Ensure that the COVID-19 surveillance strategy and testing guidance be appropriately reviewed in light of
the Reconnecting New Zealanders work programme.
c)
ensure that a decision to use any COVID-19 testing strategy is honouring the Crown’s obligation under Te
Tiriti o Waitangi
d)
position equity at the centre of choices about which testing technologies and strategies should be used
e)
consider implementation including validation and scale-up of new technologies
f)
consider the suitability of new testing strategies or technologies for whānau, hapū, iwi, Māori
communities
CT TAG may convene appropriate subgroups to meet and provide specialist advice when requested by the Ministry. A
under the Official Information Act 1982
Chair will be nominated for each of these subgroups.
CT TAG does not hold decision-making authority or responsibility for the acceptance or application of advice provided.
The scientific and technical advice and recommendations from CT TAG are provided to the Director-General and the
Ministry to inform and contribute to advice to Ministers, decisions, operations, guidelines, and policy required in the
management of COVID-19 and reconnecting Aotearoa New Zealand to the world.
The Ministry may receive advice on testing and other COVID-19 matters from a variety of sources other than CT TAG. CT
Released
TAG should maintain awareness of how it’s advice compliments advice to the Ministry from other Ministry technical
advisory groups.
Document One
CT TAG is guided by Te Tiriti o Waitangi principles as they apply to the health and disability sector; tino rangatiratanga,
equity, active protection, options, and partnership. This involves ensuring advice is evidence-based and aimed at
achieving equity of outcomes, and contributing to wellbeing for all, including Māori and Pacific peoples.
Membership
In order to contribute to the delivery of the Group’s functions, members are selected to bring multi-disciplinary
expertise on the latest scientific, clinical, technical and equity evidence relating to COVID-19 testing technologies and
paradigms.
Membership are expected to understand the systems, structures, stakeholders, and to hold in-depth specialist
knowledge in their respective disciplines.
Members will focus on the core scientific, technical, and/or clinical basis for advice, referenc ng the evidence base
alongside the rationale for advice in the context of operational limitations and/or precedent.
CT TAG will have a standing membership comprised of technical experts from disciplines relevant to the matters the
Group is asked to advise on.
The Chair and members of CT TAG will be appointed by the Director-General of Health in consultation with the
Associate Minister of Health, Hon Dr Ayesha Verrall.
Co-opted Advisors
With the agreement of the DCE COVID-19 Directorate, the Chairperson may invite Ministry Technical experts to be
advisors to the Group.
Members of CT TAG agree:
•
to keep all information provided to them strictly confidential and, except as expressly permitted, not share,
publish, copy in whole or in part or modify or adapt any confidential information in any way without the
Ministry’s prior written consent which may be given or withheld in its absolute discretion.
•
not to use any confidential information for any purpose other than participating in CT TAG activities without
the Ministry’s prior written consent which may be given or withheld in its absolute discretion.
under the Official Information Act 1982
• that whe e the CT TAG Member wishes to use the information provided for research purposes, a detailed
letter seeking permission to use the data, and describing how the data will be used including the ethical
safeguards that will be used to protect the integrity of the data, must be submitted to the Chief Science
Advisor for approval, prior to any research occurring. The Ministry may put conditions on the use of data,
including acknowledgements as appropriate.
• that pre-existing intellectual property rights relating to the provision of advice remain the property of their
current owner. New intellectual property rights in work created for the Ministry as part of CT TAG become the
Released
property of the Ministry when they are created unless otherwise agreed in writing.
•
to declare any real or perceived Conflicts of Interest - CT TAG Members should perform their functions in
good faith, honestly, fairly, impartially, responsibly and avoid situations that might compromise their integrity
Document One
or otherwise lead to conflicts of interest. The Conflict of Interest form provided by the Ministry must be
completed, returned toS9(2)(a)
• inform the Ministry upon becoming aware of the existence of the possibility of a conflict arising after
completing the form. A register of Conflict of Interest will be recorded and addressed through the processes
outlined above.
• that they are
not authorised to make statements on behalf of the COVID-19 Testing Technical Advisory Group
or the Ministry. The Ministry has strict protocols for managing media enquiries and all such requests should be
directed to S9(2)(a)
and copied to the STA email S9(2)(a)
.govt nz.
• they have the right to comment to the media on any matter in their professional capacity, as long as they do
not attribute the comment to CT TAG or imply that they are speaking on behalf of CT TAG or wider Ministry. If
a Member is forewarned of being asked to comment to the media, they should advise the STA ac ordingly. If a
Member is not forewarned, they should advise the STA immediately after making comment to the media.
• they are not authorised to commit COVID-19 Testing Technical Advisory Group, any Members of it, or the
Ministry to any financial or legal commitments or to otherwise purport to act as agents for the Ministry.
Membership of CT TAG will be for a period of 12 months with the option for a further extension as agreed by the
Director-General.
A register of membership of CT TAG is maintained and kept within the STA filing system within the Ministry and
accessible to Ministry staff. Names of CT TAG Members and any other information provided by Members are subject to
the Official Information Act 1982 and the Ministry will be required to release such information on request under that
Act unless there are valid reasons for withholding the information under the Act.
Duties and Responsibilities
Duties and responsibilities of the Chairperson of COVID-19 Testing Technical Advisory Group
The Chairperson agrees to:
• provide leadership and ensure the group retains a focus on its scope as defined in this Terms of Reference and
priorities as determined by the Ministry
• determine suitability of CT TAG as the recipient of requests for advice, work to be commissioned, tasks, and
under the Official Information Act 1982
facilitators of consultation
• ensure meetings are duly convened and that a quorum of Members is present each meeting
• ensure meetings are conducted in an efficient, effective, and focused manner
• ensure the group has the required information to permit provision of advice and to make recommendations
• consider the principles of Te Tiriti o Waitangi in every action, through ensuring CT TAG is supported to interact
and act with equity as a key consideration, and provides advice that is congruent with these obligations
• appoint Members to CT TAG based on scientific and technical expertise and the need for effective
representation and tino-rangatiratanga (self-determination and autonomy) of Māori and Pacific peoples
Released
• facilitate communications internally and externally, including; with other key stakeholders as appropriate;
presenting advice and recommendations to decision makers after each meeting; and summarising any aspects
of discussion or advice that should or should not be communicated by Members
Document One
• ensure minutes are taken during meetings and approval given for the minutes as an accurate record of the
summary of the meeting.
• ensure actions and recommendations are noted and actioned within agreed timeframes
• act as a key contact point for agenda items, responses, absences, and delegations to the meeting, and will be
informed of all activities requested of and undertaken by CT TAG.
Duties and responsibilities of a Member of COVID-19 Testing Technical Advisory Group
CT TAG Members are not employees of the Ministry. They agree to:
• familiarise themselves with background material (if any) sent prior to and after meetings
• actively participate in meetings or provide feedback and/or comments as required
• undertake additional activities agreed by the group (such as commenting on advice or guidance, providing
research material, or contacts), and to alert the Chairperson to limitations on availability and interim
delegation arrangements
• share expert knowledge and engage constructively in discussions, acting only in the role they are representing
and within their scope of expertise
• individually ensure familiarity with, and provide advice that is congruent with the principles and obligations of
Te Tiriti o Waitangi in ensuring the active protection of Māori health, achieving equity across access, quality of
care and outcomes
• ensure that all activity and advice is undertaken with consideration of and respect for equity of outcomes
across all peoples of Aotearoa New Zealand, including but not limited to; ethnicity, dis/ability, geographic
location, age, health, gender and socioeconomic position living and working conditions
• lead/facilitate the completion of respectively owned action items within the agreed timeframes
• assume collective responsibility for advice through; working together in a collegial manner; seeking consensus
on provision of advice wherever possible; and noting any unresolved differences of opinion, limitations of
evidence or opportunity for consultation, or concessions made due to time or logistical constraints
• exercise all due professional care and diligence in the performance of their obligations under these Terms of
Reference in accordance with the standards of skill, care, and diligence normally practised by suitably qualified
and experienced persons in performing services of a similar nature.
• to make themselves available for meetings convened for the purpose of providing advice to the Ministry as
described above.
Duties and responsibilities of Co-opted Advisors to the COVID-19 Testing Technical Advisory Group
Co-opted Advisors are employees of the Ministry. They agree to:
under the Official Information Act 1982
• represent the Ministry by presenting requests for advice or commissioned pieces of work and providing
relevant background information, context, and communications to support the Members in providing advice
which is shaped for the question or issue at hand
• familiarise themselves with background material (if any) sent prior to meetings
• share expert knowledge and engage constructively in discussions, acting only in the role they are representing
and within their scope of expertise
• communicate relevant information, activities, decisions, and issues of interest from the Ministry to CT TAG,
Released
and vice versa, through endorsed communication channels and methods
• individually ensure familiarity with and provide advice congruent with the principles and obligations of Te Tiriti
o Waitangi in ensuring the active protection of Māori health and achieve equity across access, quality of care
and outcomes
Document One
• ensure that all activity and advice is undertaken with consideration of and respect for equity of outcomes
across all peoples of Aotearoa New Zealand, including but not limited to; ethnicity, dis/ability, geographic
location, age, gender, health, and socioeconomic position, living and working conditions.
Secretariat of COVID-19 Testing Technical Advisory Group
The Secretariat is not a Member of CT TAG. The Secretariat supports the group and the Chairperson with:
• disseminating information required for each meeting
• writing-up the agenda as directed by the Chairperson
• writing the minutes and disseminating these within the group
• update any new Members or additional Members with the Terms of Reference
• receive and store the Conflict of Interest declarations
• receive fee claims and organise fees payments
• assist the Chairperson with the onboarding arrangements with Members.
Meeting protocols
Secretariat
The Ministry will ensure adequate secretariat support and other support as may be required from time to time, for CT
TAG to carry out their mandate efficiently and effectively.
Meeting coordination
Coordination of the meetings will be managed by the Secretariat under direction of the Chairperson. This will include all
the logistics, documentation, and administration. Members will receive relevant documentation through email or other
digital tools used within the Ministry.
Members must have regular access to electronic and digital tools in which CT TAG meetings are conducted. Meetings
conducted in workplaces must remain confidential and not visual or audible to workplace colleagues.
Delegates
Members will attend all meetings whenever reasonably possible and delegates are not permitted. Apologies must be in
writing (email) to the Chairperson and Secretariat prior to the meeting.
under the Official Information Act 1982
Other attendees
Guests with relevant expertise may be invited to discuss specific issues and when attending the whole meeting will
abide by the same Terms of Reference.
Non Members may only attend by invitation of the Chairperson.
Quorum
Released
A meeting quorum for CT TAG requires 50% of standing external Members, including the Chairperson.
The quorum for a meeting is the minimum number of Members required to make the meeting valid. If a meeting is
inquorate, it cannot make recommendations on behalf of the group. It can hold discussions and make
recommendations for later confirmation or rejection by the group.
Document One
Official Information Act requests
All agendas, emails and other communication and information relating to the Network are subject to the Official
Information Act 1982, and the Ministry may be required to release such information on request unless there are valid
reasons for withholding the information under the Act.
Fees framework
The daily rate has been set in accordance with the Ministry’s Fees Framework and has been approved by the Director-
General of Health and may be paid to Members who are self-employed or privately employed.
Members who are paid for their time/employed through the wider state sector (eg they work for Universities, District
Health Boards, Government departments and State agencies) are not personally eligible for a fee, although on the
production of an invoice, the Ministry can reimburse a government funded agency employing organisation for the
Member’s time.
The membership register will indicate those Members that are eligible to claim a fee under the Fees Framework and the
level of the fee, based on the above declaration.
A working day of eight hours is the basis of the daily fee is calculation, with hourly pro-rata rates calculated accordingly.
A working day of longer than eight hours does not attract extra payment beyond the daily fee. The daily fee applies to
all work, including the work performed outside of meetings that is required for the group to carry out its role (e.g.
preparation, representing the group at other forums or administrative work).
All fees and expenses (where agreed) are to be submi ted either on a Ministry claim form or as an invoice. Reasonable
expenses are to be agreed in writing in advance and should be supported by tax invoices and/or receipts.
Payments will be made in accordance with the Ministry’s accounts payable guidelines.
Work outside of meetings that has been formally commissioned by the Ministry will be formally described in a written
request with anticipated days or hours of work required and the fee rate, which the individual or group may accept or
decline. Additional days or hours of work required must be agreed in writing with the Manager of STA prior to
commencement of the hours worked.
under the Official Information Act 1982
Guidance on organisations that form part of the wider state sector can be found on the SSC website.
For more information, please refer to the Cabinet Fees Framework.
Review of Membership
Released
The Deputy Chief Executive, COVID-19 Directorate will advise the Director-General on a review of membership of the
COVID-19 Testing Technical Advisory Group by the end of December 2021.

Document Two
Briefing
COVID-19 Testing Technical Advisory Group Membership and Terms of
Reference
Date due to MO: 25 August 2021
Action required by:
25 August 2021
Security level:
IN CONFIDENCE
Health Report number: 20211861
To:
Hon Dr Ayesha Verrall, Associate Minister of Health
Contact for telephone discussion
Name
Position
Telephone
Dr Ashley Bloomfield
Director-General of Health
S9(2)(a)
Minister’s office to complete:
☐ Approved
☐ Decline
☐ Noted
☐ Needs change
☐ Seen
☐ Overtaken by events
☐ See Minister’s Notes
☐ Withdrawn
Comment:
under the Official Information Act 1982
Released
Document Two
COVID-19 Testing Technical Advisory
Group Membership and Terms of
Reference
Security level:
IN CONFIDENCE
Date:
25 August 2021
To:
Hon Dr Ayesha Verrall, Associate Minister of Health
Purpose of report
1.
This report provides the proposed membership and Terms of Reference for the COVID-19
Testing Technical Advisory Group (CT TAG) for your consideration and approval.
Recommendations
We recommend you:
a)
note our intention to establish the COVID-19 Testing Technical Advisory Group.
b)
approve the draft Terms of Reference in Appendix A.
Yes/No
c)
approve the proposed members listed in Appendix B for the COVID-19 Testing
Yes/No
Technical Advisory Group
under the Official Information Act 1982
Dr Ashley Bloomfield
Hon Dr Ayesha Verrall
Director-General of Health
Associate Minister of Health
Released
Date:
Date:
Briefing: HR20211861
1
Document Two
COVID-19 Testing Technical Advisory
Group Membership and Terms of
Reference
Background and context
2.
On 24 June 2021, Sir David Skegg, Chair of the Strategic Public Health Advisory Group,
recommended to Hon Dr Ayesha Verrall, Associate Minister of Health, that the government
establish an expert committee to advise on laboratory testing issues that should arise over
the next eighteen months.
3.
As the Ministry’s response to COVID-19 has continued to mature and evolve, a commitment
to continuous learning and improvement has been fundamental to delivering a quality
response to COVID-19 and keeping New Zealand safe. In particular, significant effort has
been placed into strengthening the scientific and technical advisory capabilities within the
Ministry of Health.
4.
The Ministry’s current advisory groups have continued to provide sufficient robust scientific
and technical advice to support the Ministry’s COVID-19 Response. However, the rise of
problematic variants such as the Delta variant, which has increased transmission and the
potential to cause more severe disease, and the focus on strategies to safely reconnect New
Zealanders to the world, has raised the need to further elevate our technical advisory
capability with regards to testing technology It is anticipated that an additional expert
advisory group with a focus on testing technologies will strengthen our response to COVID-
19.
Purpose and function of the Group
5.
The COVID-19 Testing Technical Advisory Group (CT TAG) will provide expert, multi-
disciplinary advice on testing based on the latest scientific, clinical and technical evidence.
6.
The scientific and technical advice and recommendations from CT TAG will be provided to
the Director-General and the Ministry to inform and contribute advice to Ministers,
decisions, operations, guidelines, and policy required in the management of COVID-19 and
reconnecting Aotearoa New Zealand to the world.
7.
under the Official Information Act 1982
The Terms of Reference for CT TAG are attached as Appendix 1 and the proposed
membership list is attached as Appendix 2.
Expertise
8.
The group will comprise of a Chair and members with expertise in relevant areas, including:
a) Microbiology
b) Epidemiology
Released
c) Immunology
d) Clinical diagnostic testing review and development
e) Operational implementation and management
Briefing: HR20211861
2
Document Two
f)
Primary care
Function
9.
CT TAG members will be asked to advise and give expert oversight on:
a) assessment of the benefits and limitations of new testing technologies and paradigms
for New Zealand, including the suitability of new technologies in different settings and
scenarios
b) comparison of new technologies to those currently in use
c) technical guidance on the expected timeframe for adopting a new technology
d) horizon-scanning to identify technologies being developed locally and overseas
e) the application of new technologies to assist in reconnecting New Zealand, including
their use in border management, and managed isolation and quarantine settings
10. The group’s advice will assist the Ministry and Government to:
a) Ensure that the COVID-19 surveillance strategy and testing guidance is fit-for-purpose
for the goals of the elimination strategy or any future pandemic response strategy as it
may be adopted.
b) Ensure that the COVID-19 surveillance strategy and testing guidance be appropriately
reviewed in light of the Reconnecting New Zealanders work programme.
c) ensure that a decision to use any COVID-19 testing strategy is honouring the Crown’s
obligation under Te Tiriti o Waitangi
d) position equity at the centre of choice about which testing technologies and
strategies should be used
e) consider implementation including validation and scale-up of new technologies
f)
consider the suitability of new testing strategies or technologies for whānau, hapū, iwi,
Māori communities
Next steps
11. The Ministry of Health will complete the process to appoint external members to the Group
and schedule the first meeting at the earliest opportunity. We will keep you informed of
progress. under the Official Information Act 1982
ENDS.
Released
Briefing: HR20211861
3

Document Two
Appendix A - Proposed Terms of Reference
Terms of Reference – Act 1982
COVID-19 Testing
Technical Advisory Group
under the Official Informat
10 August 2021
Released
Briefing: HR20211861
4
Document Two
Contents
Introduction ..................................................................................................................................................................................... 6
Context ............................................................................................................................................................................................... 6
Purpose and Function .................................................................................................................................................................. 7
Membership ..................................................................................................................................................................................... 8
Duties and Responsibilities ........................................................................................................................................................ 9
Meeting protocols ...................................................................................................................................................................... 11
Fees framework ................................................................................................................................................................... ... 12
Review of Membership ............................................................................................................................................................. 13
Act 1982
under the Official Informat
Released
Briefing: HR20211861
5
Document Two
Introduction
The Ministry of Health (the Ministry) is the kaitiaki of the health and disability system in Aotearoa New Zealand and the
principal health advisor to Government. We do this by providing a fair, effective, and sustainable system and advice that
people can trust. The Ministry is responsible for providing active stewardship and leadership across the health and
disability system to ensure it provides people with the highest level of care, regardless of who they are or where they
live.
The COVID-19 pandemic has rapidly evolved internationally and in Aotearoa New Zealand. Responding to COVID-19 in a
very rapidly changing environment is a significant ongoing challenge.
Act 1982
The Government's overall public health strategy in respect of the COVID-19 pandemic affecting New Zealand is
elimination. That is, to apply a range of control measures to stop the transmission of COVID-19 in Aotearoa New Zealand.
There are four pillars to our elimination strategy, these are:
• Keep it out (pre- and border settings, managed isolation and quarantine)
• Prepare for it (robust case detection and surveillance, and public health measures)
• Stamp it out (effective contact tracing and case management, and stronger public health measures)
• Manage the impact (health system readiness and resilience)
The Ministry has established the COVID-19 Health System Response Directorate (the Directorate) to give effect to the
elimination strategy. The Ministry is working to ensure the response to COVID-19:
• is evidence-based
• is consumer-centred
• is equity-focussed and guided by the Treaty of Waitangi
• effectively manages clinical and public health issues and risks
• supports an open and transparent culture
• has a continuous quality improvement and safety focus
• monitors and reviews clinical processes and outcomes
• guides the development of the Ministry and All of Government strategies to address COVID-19.
Context under the Official Informat
On 24 June 2021, Sir David Skegg, Chair of the Strategic Public Health Advisory Group recommended that the
government establish an expert committee to advise on the suitability of the current approach to COVID-19 testing
within New Zealand and how this approach should evolve in response to new testing technologies, where appropriate.
In particular, the approach to reconnecting Aotearoa New Zealand, will pose new paradigms, which will require the
broad range of expertise obtained through engagement with the COVID-19 Testing Technical Advisory Group.
Released
Briefing: HR20211861
6
Document Two
Purpose and Function
The COVID-19 Testing Technical Advisory Group (CT TAG) will provide rapid, independent, and practical advice to the
Director-General of Health on testing technologies and paradigms, to inform New Zealand’s COVID-19 response and the
work to reconnect Aotearoa New Zealand to the world. CT TAG members will be asked to advise and give expert
oversight on:
a)
assessment of the benefits and limitations of new testing technologies and paradigms for New Zealand,
including the suitability of new technologies in different settings and scenarios
b)
comparison of new technologies to those currently in use
Act 1982
c)
technical guidance on the expected timeframe for adopting a new technology
d)
horizon-scanning to identify technologies being developed locally and overseas
e)
the application of new technologies to assist in reconnecting New Zealand, including their use in border
management, and managed isolation and quarantine settings
The group’s advice will assist the Ministry and Government to:
g)
Ensure that the COVID-19 surveillance strategy and testing guidance is fit-for-purpose for the goals of the
elimination strategy or any future pandemic response strategy as it may be adopted.
h)
Ensure that the COVID-19 surveillance strategy and testing guidance be appropriately reviewed in light of
the Reconnecting New Zealanders work programme.
i)
ensure that a decision to use any COVID-19 testing strategy is honouring the Crown’s obligation under Te
Tiriti o Waitangi
j)
position equity at the centre of choices about which testing technologies and strategies should be used
k)
consider implementation including validation and scale-up of new technologies
l)
consider the suitability of new testing strategies or technologies for whānau, hapū, iwi, Māori
communities
CT TAG may convene appropriate subgroups to meet and provide specialist advice when requested by the Ministry. A
under the Official Informat
Chair will be nominated for each of these subgroups.
CT TAG does not hold decision-making authority or responsibility for the acceptance or application of advice provided.
The scientific and technical advice and recommendations from CT TAG are provided to the Director-General and the
Ministry to inform and contribute to advice to Ministers, decisions, operations, guidelines, and policy required in the
management of COVID-19 and reconnecting Aotearoa New Zealand to the world.
The Ministry may receive advice on testing and other COVID-19 matters from a variety of sources other than CT TAG. CT
Released
TAG should maintain awareness of how it’s advice compliments advice to the Ministry from other Ministry technical
advisory groups.
Briefing: HR20211861
7
Document Two
CT TAG is guided by Te Tiriti o Waitangi principles as they apply to the health and disability sector; tino rangatiratanga,
equity, active protection, options, and partnership. This involves ensuring advice is evidence-based and aimed at
achieving equity of outcomes, and contributing to wellbeing for all, including Māori and Pacific peoples.
Membership
Act 1982
In order to contribute to the delivery of the Group’s functions, members are selected to bring multi-disciplinary
expertise on the latest scientific, clinical, technical and equity evidence relating to COVID-19 testing technologies and
paradigms.
Membership are expected to understand the systems, structures, stakeholders, and to hold in-depth specialist
knowledge in their respective disciplines.
Members will focus on the core scientific, technical, and/or clinical basis for advice, referencing the evidence base
alongside the rationale for advice in the context of operational limitations and/or precedent.
CT TAG will have a standing membership comprised of technical experts from disciplines relevant to the matters the
Group is asked to advise on.
The Chair and members of CT TAG will be appointed by the Director-General of Health in consultation with the
Associate Minister of Health, Hon Dr Ayesha Verrall
Co-opted Advisors
With the agreement of the DCE COVID 19 Directorate, the Chairperson may invite Ministry Technical experts to be
advisors to the Group.
Members of CT TAG agree:
•
to keep all information provided to them strictly confidential and, except as expressly permitted, not share,
publish, copy in whole or in part or modify or adapt any confidential information in any way without the
under the Official Informat
Ministry’s prior written consent which may be given or withheld in its absolute discretion.
•
not o use any confidential information for any purpose other than participating in CT TAG activities without
the Ministry’s prior written consent which may be given or withheld in its absolute discretion.
• that where the CT TAG Member wishes to use the information provided for research purposes, a detailed
letter seeking permission to use the data, and describing how the data will be used including the ethical
safeguards that will be used to protect the integrity of the data, must be submitted to the Chief Science
Advisor for approval, prior to any research occurring. The Ministry may put conditions on the use of data,
Released
including acknowledgements as appropriate.
Briefing: HR20211861
8
Document Two
• that pre-existing intellectual property rights relating to the provision of advice remain the property of their
current owner. New intellectual property rights in work created for the Ministry as part of CT TAG become the
property of the Ministry when they are created unless otherwise agreed in writing.
•
to declare any real or perceived Conflicts of Interest - CT TAG Members should perform their functions in
good faith, honestly, fairly, impartially, responsibly and avoid situations that might compromise their integrity
or otherwise lead to conflicts of interest. The Conflict of Interest form provided by the Ministry must be
completed, returned to Out of Scope, S9(2)(a)
• inform the Ministry upon becoming aware of the existence of the possibility of a conflict arising after
completing the form. A register of Conflict of Interest will be recorded and addressed through the processes
outlined above.
• that they are
not authorised to make statements on behalf of the COVID-19 Testing Technical Advisory Group
Act 1982
or the Ministry. The Ministry has strict protocols for managing media enquiries and all such requests should be
directed to S9(2)(a)
and copied to the STA email S9(2)(a)
• they have the right to comment to the media on any matter in their professional capacity, as long as they do
not attribute the comment to CT TAG or imply that they are speaking on behalf o CT TAG or wider Ministry. If
a Member is forewarned of being asked to comment to the media, they should advise the STA accordingly. If a
Member is not forewarned, they should advise the STA immediately after making comment to the media.
• they are not authorised to commit COVID-19 Testing Technical Advisory Group, any Members of it, or the
Ministry to any financial or legal commitments or to otherwise purport to act as agents for the Ministry.
Membership of CT TAG will be for a period of 12 months with the option for a further extension as agreed by the
Director-General.
A register of membership of CT TAG is maintained and kept within the STA filing system within the Ministry and
accessible to Ministry staff. Names of CT TAG Members and any other information provided by Members are subject to
the Official Information Act 1982 and the Ministry will be required to release such information on request under that
Act unless there are valid reasons for withholding the information under the Act.
Duties and Responsibilities
Duties and responsibili ies of the Chairperson of COVID-19 Testing Technical Advisory Group
under the Official Informat
The Chairperson agrees to:
• provide leadership and ensure the group retains a focus on its scope as defined in this Terms of Reference and
priorities as determined by the Ministry
• determine suitability of CT TAG as the recipient of requests for advice, work to be commissioned, tasks, and
facilitators of consultation
• ensure meetings are duly convened and that a quorum of Members is present each meeting
Released
• ensure meetings are conducted in an efficient, effective, and focused manner
• ensure the group has the required information to permit provision of advice and to make recommendations
• consider the principles of Te Tiriti o Waitangi in every action, through ensuring CT TAG is supported to interact
and act with equity as a key consideration, and provides advice that is congruent with these obligations
Briefing: HR20211861
9
Document Two
• appoint Members to CT TAG based on scientific and technical expertise and the need for effective
representation and tino-rangatiratanga (self-determination and autonomy) of Māori and Pacific peoples
• facilitate communications internally and externally, including; with other key stakeholders as appropriate;
presenting advice and recommendations to decision makers after each meeting; and summarising any aspects
of discussion or advice that should or should not be communicated by Members
• ensure minutes are taken during meetings and approval given for the minutes as an accurate record of the
summary of the meeting.
• ensure actions and recommendations are noted and actioned within agreed timeframes
• act as a key contact point for agenda items, responses, absences, and delegations to the meeting, and will be
informed of all activities requested of and undertaken by CT TAG.
Duties and responsibilities of a Member of COVID-19 Testing Technical Advisory Group
Act 1982
CT TAG Members are not employees of the Ministry. They agree to:
• familiarise themselves with background material (if any) sent prior to and after meetings
• actively participate in meetings or provide feedback and/or comments as required
• undertake additional activities agreed by the group (such as commenting on advice or guidance, providing
research material, or contacts), and to alert the Chairperson to limitations on availability and interim
delegation arrangements
• share expert knowledge and engage constructively in discussions, acting only in the role they are representing
and within their scope of expertise
• individually ensure familiarity with, and provide advice that is congruent with the principles and obligations of
Te Tiriti o Waitangi in ensuring the active protection of Māori health, achieving equity across access, quality of
care and outcomes
• ensure that all activity and advice is undertaken with consideration of and respect for equity of outcomes
across all peoples of Aotearoa New Zea and, ncluding but not limited to; ethnicity, dis/ability, geographic
location, age, health, gender and socioeconomic position, living and working conditions
• lead/facilitate the completion of re pectively owned action items within the agreed timeframes
• assume collective responsibility for advice through; working together in a collegial manner; seeking consensus
on provision of advice wherever possible; and noting any unresolved differences of opinion, limitations of
evidence or opportunity for consultation, or concessions made due to time or logistical constraints
• exercise all due professional care and diligence in the performance of their obligations under these Terms of
Reference in accordance with the standards of skill, care, and diligence normally practised by suitably qualified
and experienced persons in performing services of a similar nature.
under the Official Informat
• to make themselves available for meetings convened for the purpose of providing advice to the Ministry as
described above.
Duties and responsibilities of Co-opted Advisors to the COVID-19 Testing Technical Advisory Group
Co opted Advisors are employees of the Ministry. They agree to:
• represent the Ministry by presenting requests for advice or commissioned pieces of work and providing
relevant background information, context, and communications to support the Members in providing advice
Released
which is shaped for the question or issue at hand
• familiarise themselves with background material (if any) sent prior to meetings
• share expert knowledge and engage constructively in discussions, acting only in the role they are representing
and within their scope of expertise
Briefing: HR20211861
10
Document Two
• communicate relevant information, activities, decisions, and issues of interest from the Ministry to CT TAG,
and vice versa, through endorsed communication channels and methods
• individually ensure familiarity with and provide advice congruent with the principles and obligations of Te Tiriti
o Waitangi in ensuring the active protection of Māori health and achieve equity across access, quality of care
and outcomes
• ensure that all activity and advice is undertaken with consideration of and respect for equity of outcomes
across all peoples of Aotearoa New Zealand, including but not limited to; ethnicity, dis/ability, geographic
location, age, gender, health, and socioeconomic position, living and working conditions.
Secretariat of COVID-19 Testing Technical Advisory Group
The Secretariat is not a Member of CT TAG. The Secretariat supports the group and the Chairperson with:
• disseminating information required for each meeting
Act 1982
• writing-up the agenda as directed by the Chairperson
• writing the minutes and disseminating these within the group
• update any new Members or additional Members with the Terms of Reference
• receive and store the Conflict of Interest declarations
• receive fee claims and organise fees payments
• assist the Chairperson with the onboarding arrangements with Members.
Meeting protocols
Secretariat
The Ministry will ensure adequate secretariat support and other support as may be required from time to time, for CT
TAG to carry out their mandate efficiently and effectively.
Meetings coordination
Coordination of the meetings will be managed by the Secretariat under direction of the Chairperson. This will include all
the logistics, documentation, and administration. Members will receive relevant documentation through email or other
digital tools used within the Ministry.
Members must have regular access to electronic and digital tools in which CT TAG meetings are conducted. Meetings
conducted in workplaces must remain confidential and not visual or audible to workplace colleagues.
under the Official Informat
Delegates
Members will attend all meetings whenever reasonably possible and delegates are not permitted. Apologies must be in
writing (email) to the Chairperson and Secretariat prior to the meeting.
Other attendees
Guests with relevant expertise may be invited to discuss specific issues and when attending the whole meeting will
Released
abide by the same Terms of Reference.
Non-Members may only attend by invitation of the Chairperson.
Quorum
Briefing: HR20211861
11
Document Two
A meeting quorum for CT TAG requires 50% of standing external Members, including the Chairperson.
The quorum for a meeting is the minimum number of Members required to make the meeting valid. If a meeting is
inquorate, it cannot make recommendations on behalf of the group. It can hold discussions and make
recommendations for later confirmation or rejection by the group.
Official Information Act requests
All agendas, emails and other communication and information relating to the Network are subject to the Official
Information Act 1982, and the Ministry may be required to release such information on request unless there are valid
reasons for withholding the information under the Act.
Act 1982
Fees framework
The daily rate has been set in accordance with the Ministry’s Fees Framework and has been approved by the Director-
General of Health and may be paid to Members who are self-employed or privately employed.
Members who are paid for their time/employed through the wider state sector (eg they work for Universities, District
Health Boards, Government departments and State agencies) are not personally eligible for a fee, although on the
production of an invoice, the Ministry can reimburse a government funded agency employing organisation for the
Member’s time.
The membership register will indicate those Members that are eligible to claim a fee under the Fees Framework and the
level of the fee, based on the above declaration.
A working day of eight hours is the basis of the daily fee is calculation, with hourly pro-rata rates calculated accordingly.
A working day of longer than eight hours does not attract extra payment beyond the daily fee. The daily fee applies to
all work, including the work performed outside of meetings that is required for the group to carry out its role (e.g.
preparation, representing the group at other forums, or administrative work).
All fees and expenses (where agreed) are to be submitted either on a Ministry claim form or as an invoice. Reasonable
expenses are to be agreed in writing in advance and should be supported by tax invoices and/or receipts.
under the Official Informat
Payments will be made in accordance with the Ministry’s accounts payable guidelines.
Work outside of meetings that has been formally commissioned by the Ministry will be formally described in a written
request with anticipated days or hours of work required and the fee rate, which the individual or group may accept or
decline. Additional days or hours of work required must be agreed in writing with the Manager of STA prior to
commencement of the hours worked.
Guidance on organisations that form part of the wider state sector can be found on the SSC website.
Released
For more information, please refer to the Cabinet Fees Framework.
Briefing: HR20211861
12
Document Two
Review of Membership
The Deputy Chief Executive, COVID-19 Directorate will advise the Director-General on a review of membership of the
COVID-19 Testing Technical Advisory Group by the end of December 2021.
Act 1982
under the Official Informat
Released
Briefing: HR20211861
13
Document Two
Appendix B - Proposed Membership List
Role
Incumbent
Chair (and Microbiology expertise)
Professor David Murdoch, Dean and Head of Campus,
University of Otago, Christchurch; and Vice Chancellor
Designate, University of Otago
Clinical Immunology and diagnostic expertise
Dr Maia Brewerton, Lead Clinician, Immunology, WDHB
Microbiology and Infectious Diseases expertise and
Dr Susan Morpeth, Chair of the Microbiology Network
Act 1982
leadership
Aotearoa New Zealand; and Clinical Microbiologist,
Counties Manukau Health Laboratory Services
Microbiology and Infectious Diseases expertise
Dr Tim Blackmore, CCDHB, We lington
Infectious Diseases Epidemiology, Public Health
Professor Patricia Priest, University of Otago
Medical Laboratory Science expertise and Laboratory
Kirsten Beynon, General Manager, Canterbury Health
Leadership
Laboratories and West Coast DHB Laboratory
Pacific representative and behavioural insights
Pisi a Fanolua, Clinical Nurse Manager, Sebel and
Waipuna MIFs
Co-opted Ministry employees likely to be regular attendees
Chief Science Officer (Ministry of Health)
Dr Ian Town or delegate
GM Data and Digital
Jon Herries
GM Logistics and Inventory, COVID-19 Vaccine and
Ian Costello
Immunisation Programme
under the Official Informat
GM COVID-19 Testing and Supply
Darryl Carpenter or delegate
Released
Briefing: HR20211861
14

Document Three
Memo
Surveillance of Healthcare workers during an outbreak of COVID-19 in
Aotearoa New Zealand – COVID-19 Testing Technical Advisory Group
recommendations
Date:
27 August 2021
To:
Ashely Bloomfield, Director-General, Ministry of Health
From:
David Murdoch, Chair of COVID-19 Testing Technical Advisory Group (CT TAG)
Cc:
Ian Town, Chief Science Advisor
Darryl Carpenter, Group Manager, COVID-19 Testing and Supply
For your:
Consideration
Purpose of report
1.
To summarise the COVID-19 Testing Technical Advisory Group’s recommendations on the
Surveillance of Healthcare workers during an outbreak of COVID-19 in Aotearoa New
Zealand.
Context
2.
Currently, those caring for patients with COVID-19 within a healthcare setting are offered
participation in voluntary surveillance testing. As this is a voluntary programme, the uptake is
not currently recorded by the Ministry of Health but has been reported anecdotally as low.
3.
As part of the public health response within the elimination strategy against COVID-19 the
identification of contacts of cases and strict adherence to isolation and testing is essential.
4.
In the setting of a community outbreak of COVID-19, as we are currently experiencing in
August 2021, a single case of COVID-19 presenting in a healthcare setting who has a number
under the Official Information Act 1982
of contacts and the outcome being that entire units and departments may need to be
isolated and tested under the legal direction of Section 70 notification, significantly impacting
on the delivery of healthcare to New Zealanders.
5.
While this has been particularly evident in Auckland-based hospitals, this dilemma is
recognised as a potential risk to any healthcare setting in areas where there is uncontrolled
community transmission.
6.
An intensified surveillance strategy has been suggested for healthcare workers, similar to that
required of border workers, whereby surveillance testing is both routine and potentially
Released
mandatory.
7.
Such an increase in testing could out-strip current capacity. Options other than
nasopharyngeal swab PCR testing need to be considered. Two options were proposed for CT
TAG to consider:
Page 1 of 2


Document Three
a. Expansion of saliva-based PCR testing to include healthcare workers, noting the ability
for self-sampling, self-delivery to the lab, and increased tolerability of regular testing
as advantages over nasopharyngeal or oropharyngeal based RT-PCR.
b. Adoption of rapid antigen tests for healthcare workers, although potentially can
return a result on the spot, are only currently approved in New Zealand detection of
symptomatic cases.
Recommendations 8.
CT TAG noted that within the current outbreak there may not be a current need to
intensify surveillance testing as the impacts on health care workers appear to be
manageable.
9.
However the opportunity should be taken to act and prepare for situations where there
would be a need to intensify the surveillance strategy in response to a new outbreak of
COVID-19.
10.
With regards to testing modalities to deliver this strategy, CT TAG proposed:
a. That when a more intense surveillance strategy for healthcare workers is required,
consideration should be given to making the testing mandatory.
b. Healthcare workers should be given the opportunity to choose their preferred sample
type for RT-PCR testing; either nasopharyngeal swab, anterior nasal / oropharyngeal
swab or saliva, with the intent that such choice should improve adherence to the
testing schedule.
c. Noting the current operational onstraints (volume, supply chain and turnaround
time) affecting the current provider of saliva-based PCR testing, consideration should
be given to alternative solutions to deliver this strategy as saliva-based PCR is likely to
be a popular option.
d. Rapid antigen tests may have a role in this situation in future, however they require
further assessment and field trials prior to their implementation within Aotearoa New
Zealand.
under the Official Information Act 1982
Professor David Murdoch
Chair CT TAG
Released
Page 2 of 2




Document Six
6.0 Next Steps/Decisions Pending
All
Verbal
7.0 Agenda Items for Next Meeting
Chair
Verbal
under the Official Information Act 1982
Released


Document Eight
4.0
Rapid review of COVID-19 laboratory diagnostic activities and systems
The purpose of the rapid review is to ensure the ongoing and efficient delivery of high-quality, equitable,
scalable and adaptable COVID-19 diagnostic testing to support the objectives of New Zealand’s pandemic
response and reconnection plan. This wil be done by:
1. Reviewing, evaluating and making recommendations on the coordination of COVID-19
laboratory activities/workstreams and requirements.
2. Identifying potential challenges, constraints, gaps and unrecognised opportunities to ensure
ongoing sustainable and fit for purpose COVID-19 testing within New Zealand
• Government requests the report to be delivered by Friday 1 October 2021.
• Tentative schedule is to have interviews Friday afternoon, al day Monday, and Tuesday morning.
Monday meetings wil be face-to-face and Chair wil be travelling to Wel ington. A debrief and
writing of the report wil occur Tuesday and Wednesday with a plan to delive a draft to the DG by
Thursday.
• Chair wil attend al meetings. It was requested Testing TAG members also join each interview but
schedules may be difficult to align.
• It was noted several representative groups would like to be scheduled for Monday afternoon. STA
is working on the logistics and wil do its best to accommodate the various groups.
• There is a desire to have the perspective of laboratory IT and data management. There is little
regulation on what data is provided and what level of detail for data is required. It was recognised
this is an important consideration and a group wil be organised for an interview for their input into
the review.
• There are 15 interview times set aside at the moment. It was requested that because there are so
many groups and limited time, that bullet points or key points are shared with each group when
sending invites.
• Due to the time constraints, it was suggested that contributors write to the Chair if they are unable
to attend an interview.
• A member asked about confidentiality and what wil be discoverable. It was noted individuals wil
not be identified but the report can be OIA if requested. Since the report is systems focused, there
should be no concerns. If minutes are OIA, members wil be notified.
• A concern was raised that during interviews there may be some people who feel they cannot
speak freely because of others in attendance. The Chair wil be sure to express anyone can
contact him directly if they want to be confidential.
under the Official Information Act 1982
• A member asked if the representatives from POC should be interviewed. It was agreed this is an
important perspective. The member wil send a list of individuals from POC to STA to contact.
• A question was raised whether commercial companies should be interviewed and if there was
value there because at the moment none were on the list to be interviewed.
o It was suggested to get written feedback from them instead of setting aside interview time.
o It was suggested the Chair contact them separate from the rapid review and not engage in
a formal context.
Released o A member noted the Terms of Reference (TOR) need to be clear so that they are fulfiled
and a boundary put in place on the scope. Commercial entities may not have much to add
to the TOR.

Document Nine
MINUTES: COVID-19 Testing Technical Advisory Group
Date:
09 September 2021
Time:
2:30pm to 3:30pm
Location:
Out of Scope
Chair:
David Murdoch
Members:
Kirsten Beynon, Maia Brewerton, Patricia Priest, Pisila Fanolua, Susan Morpeth,
Tim Blackmore
Ministry of Health Attendees: Christian Marchello, Christina Bir, Daniel Bernal, Ian Town, Jon Herries, Kelsey
Bilek, Mark Ayson
Guests:
Apologies:
Darryl Carpenter, Ian Costel o
1.0
Welcome and Previous Minutes
Professor David Murdoch welcomed all members and attendees in his capacity as Chair of the COVID-19
Testing Technical Advisory Group.
Minutes of the last meeting (26 August 2021) were accepted, subject to the fol owing changes (marked in
in red) on item
3.0 Surveil ance Test ng for the Auckland Healthcare Workforce
• Turnaround time (TAT) would decrease increase substantially if all healthcare workers were
tested. The system is already at capacity testing in the community, especially with the growing
number of LOI.
2.0
Where Ministry Testing and Supply gets advice from and how decisions are made
• Chair expressed the desire to understand where the Ministry’s COVID-19 Testing and Supply has
gotten advice from previously and how decisions are made based on that advice in order to set a
work programme for Testing TAG.
under the Official Information Act 1982
• Testing and Supply seeks advice from a number of sources, examples include, but not limited to:
Ministry Science and Insights, New Zealand Microbiology Network, ESR, NZ POC TAG, Saliva
Testing Clinical Governance Group, and individuals within and outside the Ministry.
• A member expressed a visualisation document would be helpful to view the advice network.
• A document that charted the timing of advice and decisions made about saliva testing was
requested and was agreed to be shared with the TAG by Testing and Supply.
• Several members commented and agreed that there needs to be a clearer sense about what
Released happens to TAG advice and clarity on the decision-making process. There needs to be an
understanding of the trajectory for where the advice goes, who listens to the advice, and what
results come from the advice.
Document Nine
• It was outlined that TAG advice wil be especial y useful in understanding testing technology and
how it can support Aotearoa New Zealand with reconnecting. Advice may be provide support for
ministries, or provide detail if ministers require knowledge and insights on certain tests. It was
noted the minutes of Testing TAG are subject to OIA.
• A concern was raised that messaging and communications have centred on a single sample type
(saliva), which is often discussed out of context.
• It was noted some laboratory workers needed a test but were unable to self-administer and did not
have any information on performing collection of the samples. It would helpful if Ministry put out a
video or animation similar to the vaccine programme to explain how COVID-19 samples are
collected.
3.0
Surveil ance Testing for the Auckland Healthcare Workforce - Update
Update
• Advice was provided to the 3 DHBs in Auckland and all 3 have onsite surveil ance testing available
for healthcare workers. They can also visit a CTC if needed. Approximately 3,000 staff have had a
surveil ance test in addition to staff testing already in place. There was not a breakdown of who
was getting a test for surveil ance, for being a contact, or for being symptomatic. DHBs were
instructed healthcare workers should be tested weekly.
TAG feedback
• It was not clear from those familiar with the DHBs and hospitals that this process had been put in
place. It was also unclear whether this surveil ance testing was strongly
recommended/encouraged or mandatory. It was noted the testing was voluntary, but options were
being considered for making it a requirement.
• Knowing the number of tests is not helpful without knowing which were part of regular surveil ance
or were people getting tested for other reasons.
• A member commented there has not been any communications or promotion of the surveil ance
testing.
• Legal aspects are also important to consider, especial y with regards to health and safety
assessments of the workplace.
• The feedback was welcomed, and Testing and Supply wil take the comments back to the
appropriate people.
4.0
Testing TAG Work Programme
Background under the Official Information Act 1982
• The Work Programme provided was a rough draft from various discussions among members.
• The proposed Work Programme had 5 key points:
o Saliva testing
o Reconnecting New Zealand
o Community testing
Released o New Zealand initiatives
o Standard operating procedures for obtaining operational advice
Document Nine
• A member noted there is pressure to get ahead of the curve and the benefits of the Testing Tag
would be getting proper advice on these key points and how technology and commercial
developments can be used.
• Chair opened the floor for discussion.
TAG Feedback on Work Programme
• A concern was raised about lab capacity and resources. Advanced notice is needed to scale up.
• An authoritative statement on the role of saliva from this group would be helpful in easing
concerns about the sample type.
• A member said laboratories need leadership for what is needed from them now and in the future.
How many tests wil be run, how sensitive those tests need to be, wil testing be done on anyone
with common colds, what is the scale of testing, wil laboratories be expected to pay or wil there
be public funding. Individual laboratories wil not want to invest in high throughpu equipment if it is
not clear that it is needed. Planning is needed for how testing wil work under the elimination
strategy and moving forward through the reconnecting NZ phases.
• It was requested that a paper by an outside member on laboratory investments could be made in
the short to medium term to highlight issues for the agenda.
• It was noted that Testing TAG should prioritise advice on lower sensitive POC tests so that advice
can be given quickly when it is requested. An interest in testing later in disease, such as
inflammatory T-cell tests, was noted so TAG was more forward looking.
• A member raised concern about relying on one type of laboratory test wil increase the likelihood
of failure and diversity of testing is preferred.
• There are now borders in place within the country for Auckland Level 4 and the rest of the country
at Level 2. A question was raised about testing being different in Auckland versus for someone
outside the border as well as those crossing the border.
• Member noted that operational guidance should be irrespective of test type and more on delivery,
scaling, and capacity during each reconnecting NZ phases. That is, categorising different phases
and responding with the right test scenarios is needed.
• It was suggested that the maximum testing capacity that is achievable be considered first and
work back from there so that it is understood what can and cannot be done.
• The topic of having a statement from Testing TAG on saliva was raised again:
o Useful to develop and keep for when needed. Can write up and deliver so that the
decision to be used would be on Ministers.
o NZMN wil have a statement and is in advanced draft. Member wil try to secure the
under the Official Information Act 1982
statement and share with the group.
• No action is needed for MBIE document. MBIE plans to do continue work on briefing paper to fill in
further information on testing technologies. When questions arise, they wil be brought back to the
group.
• The different phases and scenarios for reconnecting NZ and the tests being considered wil be
brought to the group for feedback and input by Testing and Supply.
• It was noted that pilot studies and informed consent for new tests limits the ability to consider new
specimens and assays. A process such as a verbal informed consent and collecting 2 samples at
Released the same time could speed up the process.
• Wastewater testing was also addressed as a surveil ance tool that is within the scope of the
Testing TAG and valuable to have on board.

Document Nine
which tests might be most
helpful.
Secure NZMN draft statement
3
Testing TAG Work
Programme
on saliva testing to share with
Susan Morpeth
09/09 – Action raised
the group
Engage with Members to
4
Testing TAG Work
Programme
develop CT TAG work
Chair
09/09 – Action raised
programme
under the Official Information Act 1982
Released

Document Ten
MINUTES: COVID-19 Testing Technical Advisory Group
Date:
26 August 2021
Time:
2:30pm to 3:30pm
Location:
Out of Scope
Chair:
David Murdoch
Members:
Kirsten Beynon, Maia Brewerton, Patricia Priest, Pisila Fanolua, Susan Morpeth,
Tim Blackmore
Ministry of Health Attendees: Dan Bernal, Darryl Carpenter, Helena Woods, Ian Town, Jon Herries, Christian
Marchello, Kelsey Bilek, Mark Ayson, Chris Hedlund
Guests:
Apologies:
Christina Bir, Ian Costello
1.0
Welcome and Previous Minutes
Professor David Murdoch welcomed all members and attendees in his capacity as Chair of the
COVID-19 Testing Technical Advis ry Group.
The Chair thanked the group for coming together with urgency as we manage the current the
outbreak.
2.0
Group membership, Terms of Reference and Meeting Frequency
The Chair welcomed feedback for the Terms of Reference
• The purpose of the group is to provide oversight to some of the testing issues for COVID-
19.
• A member inquired about the expectation and need to utilise personal networks and
contacts to inform advice that is brought to the TAG. Al members agree this is essential for
providing best advice but as long as it is done with consideration for confidentiality and
under the Official Information Act 1982
abides by the Terms of Reference.
• Regularly scheduled CT TAG meetings wil be fortnightly. Agenda items wil be circulated
prior to meetings with the aim to have specific questions for the group to answer.
3.0
Surveil ance Testing for the Auckland Healthcare Workforce
Background and context
• Currently healthcare workers are asked to present for testing in the same way as other
members of the public through the CTCs, CBACs, and GPs network if they are
Released symptomatic or close contacts of cases.
• If anyone in the healthcare workforce is a close contact or the hospital where they work is
a location of interest (LOI) then the potential loss of capability and capacity in the hospital
setting is significant.
• Questions posed to TAG group:
Document Ten
o Is surveil ance testing of healthcare workforce and workers across greater DHBs
justified and appropriate?
o If testing surveil ance is appropriate, should nasopharyngeal (NP) swabs, saliva, or
rapid antigen tests (RAT) be used?
• CT TAG is not to consider operationalising the proposed surveil ance methods, only if it is
appropriate and what testing method to use if so.
• It was noted there is currently an Expression of Interest (EOI) received to perform saliva
testing.
Feedback from CT TAG
• A question was posed asking what is currently happening for testing border workers
o Border workers can choose saliva to replace NP as of 12/08/2021. If they choose
to do so, the workers need to provide a series of 2 saliva tests at least 2 days
apart over a 7-day period as part of the mandatory testing requirement
• Member noted that the question brought to CT TAG on the appropriateness of surveil ance
should be considered by a broader group, including Ministry’s Science and Insights, and
ODPH. Once advice is provided by those groups, CT TAG can advise on testing methods.
• A concern was raised that doing surveil ance testing on healthcare workers not directly
caring for COVID-19 patients would undermine standard IPC
• A question was asked about how many border workers have selected taking a saliva test
over NP. Based on the Border Operations survey, it is believed approximately 25% of the
border workforce wil opt-in to saliva.
• It was noted that this requested advice from CT TAG is specific to the current outbreak.
The EOI for saliva testing is for the duration of the outbreak for Auckland healthcare
workers.
• A member expressed that the situation is very dynamic. Today, next week, and 3 months
from now could be different. Member does not believe surveil ance is needed today but
may be needed next week or down the road. Preparations should begin now to be able
implement immediately when needed.
• Turnaround time (TAT) would decrease substantial y if all healthcare workers were tested.
The system is already at capacity testing in the community, especial y with the growing
number of LOI.
• Member noted that if surveil ance testing is already occurring among border workers, we
should be testing other critical services as wel .
• It was noted that the document proposing the 3 testing options (NP, saliva, and RAT) did
not consider point of care (POC) NAAT such as RT-LAMP. These more sensitive methods
could be produced rapidly and test a large number of people if enough machines were put
in place.
• Most data on POC RAT are pre-Delta. The Ct values with Delta might change RAT
assumptions. RAT was discounted initial y and might be more sensitive now.
under the Official Information Act 1982
o Limitations of RAT were noted, sensitivity in asymptomatic is unknown and using
RAT would be off label for asymptomatic screening by Medsafe.
o Limitations less of an issue if you can increase frequency of doing a RAT.
o RAT likely wil not work because a swab is stil needed.
• Three hospitals in Auckland have set up testing col ection sites for workers so they do not
have to travel to a CTC/CBAC. It was noted that some healthcare workers may be lost if
testing was made mandatory.
• A member noted that not all LOI are the same, referring to exposure risk. Without
Released additional information, it was driving a surge in testing in the community.
• Member agreed with the limitations of RAT and suggested saliva as the appropriate testing
method. Saliva could be done at home by the worker and dropped off.
Document Ten
• Member noted that we need to be flexible and that giving people a choice may help. We
should be prepared to consider al options. A combination of tests (e.g., offering the worker
either NP or saliva) is the best approach.
• From the clinical side, it was addressed that many healthcare workers are used to having
NP swabs and continuing this approach would also not be a bad idea.
• It was expressed that saliva has an ‘image problem’, that even though it is not inferior to
NP, many still believe it is.
• We need to be able to stand up healthcare testing surveil ance quickly and not just in
Auckland. A plan is needed to be able to do this anywhere in Aotearoa New Zealand.
• It was noted ‘healthcare’ needs to mean every worker at the facility (e.g., not just doctors
and nurses, but al staff). This meeting is discussing implications for hospitals at the
moment, but advice can be adapted to GPs and other DHB staff.
• Member expressed concern about EOI on saliva to not be over-reliant on one supplier.
There are global shortages and could pose a significant problem later.
Main takeaways
• Within the current outbreak there may not be a current need to intensify surveil ance
testing as the impacts on health care workers appear to be manageable.
• The opportunity should be taken to act and prepare for situations where there would be a
need to intensify the surveil ance strategy in response to a new outbreak of COVID-19.
• Healthcare workers should be given the opportunity to choose their preferred sample type
for RT-PCR testing; either nasopharyngeal swab anterior nasal / oropharyngeal swab or
saliva, with the intent that such choice should mprove adherence to the testing schedule.
• Noting the current operational constraints (volume, supply chain and turnaround time)
affecting the current provider of saliva-based PCR testing, consideration should be given to
alternative solutions to deliver this strategy as saliva-based PCR is likely to be a popular
option.
• Rapid antigen tests may have a role in this situation in future, however they require further
assessment and field trials prior to their implementation within Aotearoa New Zealand
4.0
Testing Update as Background
• Members to review on own time and provide feedback directly to the Chair or Science &
Technical Advisory after the meeting.
5.0
Any Other Business
None noted
6.0
Agenda Items for Next Meeting
None noted
under the Official Information Act 1982
7.0
New Action Items Raised During Meeting
None noted
Meeting closed at
3:41pm Next meeting
09 September 2021
Released

Document Eleven
1982
Terms of Reference –
COVID-19
Therapeutics Technical
Advisory Group
under the Official Information Ac
Released
27 August 2021
1
Document Eleven
Contents
Introduction ............................................................................................................................... 3
Purpose and Function ............................................................................................................................. 3
Membership ........................................................................................................................................... 4
Duties and Responsibilities ..................................................................................................................... 6
1982
Advice and Other Requests .................................................................................................................... 9
Meeting protocols .............................................................................................................................. . 9
Fees framework ......................................................................................................................... ... ..... 10
Review of Membership.................................................................................................... .... ..... ......... 11
under the Official Information Ac
Released
2
Document Eleven
Introduction
The Ministry of Health (the Ministry) is the kaitiaki of the health and disability system in Aotearoa New Zealand.
We do this by providing a fair, effective and sustainable system that people trust. The Ministry is responsible for
providing active stewardship and leadership across the health and disability system to ensure it provides people
with the highest level of care, regardless of who they are or where they live.
1982
The COVID-19 pandemic has rapidly evolved internationally and in Aotearoa New Zealand. Responding to COVID-
19 in a very rapidly changing environment is a significant ongoing challenge.
The Government's overall public health strategy in respect of the COVID-19 pandemic affecting New Zealand is
elimination. That is, to apply a range of control measures in order to stop the transmission of COVID-19 in Aotearoa
New Zealand.
There are four pillars to our elimination strategy, these are:
• border controls
• robust case detection and surveillance
• effective contact tracing and quarantine
• strong community support of control measures
The Ministry has established the COVID-19 Health System Response Directorate (the Directorate) to give effect
to the elimination strategy. The Ministry is working to ensure the response to COVID-19:
• is evidence-based
• is consumer-centred
• is equity-focused and guided by the Treaty of Waitangi
• effectively manages clinical and public health issues and risks
• supports an open and transparent culture
• has a continuous quality improvement and safety focus
• monitors and reviews clinical processes and outcomes
• guides the development of the Ministry and All of Government strategies to address COVID-19.
under the Official Information Ac
Purpose and Function
The COVID-19 Therapeutics Technical Advisory Group (Therapeutics TAG) comprises a standing membership of
Released
external expert advisors who will provide expert technical advice on therapeutics for use for patients with
COVID-19 including but not limited to:
• Identifying therapeutics which may be beneficial in the management of COVID-19
• Enabling the acquisition of these agents for clinical use in New Zealand
3
Document Eleven
• Developing appropriate guidelines for clinical use.
Therapeutics TAG has been established as part of the Ministry’s response to COVID-19 and will provide expert
technical advice to the Ministry during the response to COVID-19 pandemic.
Therapeutics TAG does not hold decision-making authority or responsibility for the acceptance or application of
advice provided. The scientific and technical advice and recommendations from Therapeutics TAG are provided
to the Ministry to inform and contribute to decisions, operations, guidelines and policy required in the
1982
management of COVID-19. The Ministry receives advice from a variety of sources including but not limited to
Therapeutics TAG.
Therapeutics TAG is guided by Te Tiriti o Waitangi principles as they apply to the health and disability sector; tino
rangatiratanga, equity, active protection, options, and partnership. This involves the managing of the response
to COVID-19 pandemic through evidence-based approaches with the aim of achieving equity of outcomes, and
contributing to wellbeing for all, including Māori and Pacific peoples.
These Therapeutics TAG Terms of Reference replace any previous terms of reference agreed by Members for
Therapeutics TAG.
Membership
The Therapeutics Technical Advisory Group is to p ovide expert, multi-disciplinary expertise on the latest
scientific, clinical and technical evidence-based, expert advice on COVID-19.
Members of the Therapeutics TAG will be asked to:
• provide the Ministry with rapid advice based on the most up to date clinical, scientific and technical
evidence on therapeutics for the treatment of COVID-19
• identify emerging scientific, clinical or technical issues and inform the Ministry on ways this advice could
be used to design the response to COVID-19 pandemic within Aotearoa New Zealand
under the Official Information Ac
• suggest approaches and actions to enact the principles of Te Tiriti o Waitangi and achieve equity for
Māori
• advise on ways to reduce inequalities for groups in society negatively impacted by COVID-19, including
but not limited to; ethnicity, dis/ability, geographic location, age, gender, health status, socioeconomic
position, living and working conditions
• identify areas requiring further research, and/or reviews to inform ongoing response.
Released
The appointment of Members of Therapeutics TAG is based on their personal, technical and specialist expertise.
This includes acknowledgement of Member’s understanding of the systems, structures, stakeholders, and in-
depth specialist knowledge in their respective disciplines, with a view to supporting the effective development
and application of technical advice.
4
Document Eleven
Members will focus on the core scientific, technical, and/or clinical basis for advice, referencing the evidence
base alongside the rationale for advice in the context of operational limitations and/or precedent. Therapeutics
TAG will comprise equitable Māori representation, alongside representation from Pacific and the disability
sector.
Membership of Therapeutics TAG will be confirmed through an appointment letter from the Chairperson and a
confirmation response from the Member.
Chairperson
1982
Therapeutics TAG will be led by the Chairperson who can be a Ministry employee.
Members
Therapeutics TAG has a standing membership comprised of external (main job is not Ministry employee)
technical experts from disciplines relevant to the response required in the phases and alert levels of the COVID-
19 pandemic. The membership also comprises of equitable Māori representation, alongside representation
from Pacific and the disability sector.
Ex Officio Advisors
Technical experts within the Ministry can also have membership within the group in the capacity of Ex Officio
Advisors as invited by the Chairperson.
Members of Therapeutics TAG must agree:
•
to keep all information provided to them strictly confidential and, except as expressly permitted, not
share, publish, copy in whole or in part or modify or adapt any confidential information in any way without
the Ministry’s prior written consent which may be given or withheld in its absolute discretion.
•
not to use any confidential information for any purpose other than participating in Therapeutics TAG
activities without the Ministry’s prior written consent which may be given or withheld in its absolute
discretion.
Where the Therapeutics TAG Member wishes to use the information provided for research purposes, a
under the Official Information Ac
detailed letter seeking permission to use the data, and describing how the data will be used including the
ethical safeguards that will be used to protect the integrity of the data, must be submitted to the Chief
Science Advisor for approval, prior to any research occurring. The Ministry may put conditions on the use
of data, including acknowledgements as appropriate.
Pre-existing intellectual property rights relating to the provision of advice remain the property of their
current owner. New intellectual property rights in work created for the Ministry as part of Therapeutics
TAG become the property of the Ministry when they are created unless otherwise agreed in writing.
Released
•
to declare any real or perceived Conflicts of Interest - Therapeutics TAG Members should perform their
functions in good faith, honestly, fairly, impartially, responsibly and avoid situations that might compromise
5
Document Eleven
their integrity or otherwise lead to conflicts of interest. The Conflict of Interest form provided by the
Ministry must be completed, returned to S9(2)(a)
The Member must inform the Ministry upon becoming aware of the existence of the possibility of a conflict
arising after completing the form. A register of Conflict of Interest will be recorded and addressed through
the processes outlined above.
• Members of Therapeutics TAG are
not authorised to make statements on behalf of Therapeutics TAG or
the Ministry. The Ministry has strict protocols for managing media enquiries and all such requests should be
S9(2)(a)
S9(2)
1982
directed to
and copied to the Science & Technical Advisory (STA) email
Members have the right to comment to the media on any matter in their professional capacity, as long as
they do not attribute the comment to Therapeutics TAG or imply that they are speaking on behalf of
Therapeutics TAG or wider Ministry. If a Member is forewarned of being asked to comment to the media,
they should advise the STA accordingly. If a Member is not forewarned, they should advise the STA
immediately after making comment to the media.
• Members are not authorised to commit Therapeutics TAG, any Members of it, or the Ministry to any
financial or legal commitments or to otherwise purport to act as agents for the Ministry.
Membership of Therapeutics TAG will be for a period of 12 months with the option for a further extension
as offered by the Ministry.
A register of membership of Therapeutics TAG is maintained and kept within the STA filing system within
the Ministry and accessible to Ministry staff. Names of Therapeutics TAG Members and any other
information provided by Members are subject to the Official Information Act 1982 and the Ministry will be
required to release such information on request under that Act unless there are valid reasons for
withholding the information under the Act.
Duties and Responsibilities
under the Official Information Ac
The duties and responsibilities for the Chairperson, Members and Ex Officio advisors are outlined below.
Duties and responsibilities of the Chairperson of Therapeutics TAG
The Chairperson agrees to:
• provide leadership and ensure the group retains a focus on its scope as defined in this Terms of
Reference and priorities as determined by the Ministry
Released
• determine suitability of Therapeutics TAG as the recipient of requests for advice, work to be
commissioned, tasks, and facilitators of consultation
• ensure meetings are duly convened and that a quorum of Members is present each meeting
• ensure meetings are conducted in an efficient, effective and focused manner
6
Document Eleven
• ensure the group has the required information to permit provision of advice and to make
recommendations
• consider the principles of Te Tiriti o Waitangi in every action, through ensuring Therapeutics TAG is
supported to interact and act with equity as a key consideration, and provides advice that is congruent
with these obligations
• appoint Members to Therapeutics TAG based on scientific and technical expertise and the need for
effective representation and tino-rangatiratanga (self-determination and autonomy) of Māori and Pacific
peoples
• facilitate communications internally and externally, including: with other key stakeholders as
appropriate; presenting advice and recommendations to decision makers after each meeting; and
summarising any aspects of discussion or advice that should or should not be communicated by
Members
• ensure minutes are taken during meetings and approval given for the minutes as an accurate record of
the summary of the meeting.
• ensure actions and recommendations are noted and actioned within agreed timeframes
• act as a key contact point for agenda items, responses, absences, and delegations to the meeting, and
will be informed of all activities requested of and undertaken by Therapeutics TAG.
Duties and responsibilities of a Member of Therapeutics TAG
Therapeutics TAG Members are not employees of the Ministry. They agree to:
• familiarise themselves with background material (if any) sent prior to and after meetings
• actively participate in meetings or provide feedback and/or comments as required
• undertake additional activities agreed by the group (such as commenting on advice or guidance,
providing research material, or contacts), and to alert the Chairperson to limitations on availability and
interim delegation arrangements
• share expert knowledge and engage constructively in discussions, acting only in the role they are
representing and within their scope of expertise
under the Official Information Act 1982
• individually ensure familiarity with, and provide advice that is congruent with the principles and
obligations of Te Tiriti o Waitangi in ensuring the active protection of Māori health, achieving equity
across access, quality of care and outcomes
• ensure that all activity and advice is undertaken with consideration of and respect for equity of
outcomes across all peoples of Aotearoa New Zealand, including but not limited to; ethnicity, dis/ability,
geographic location, age, health, gender and socioeconomic position, living and working conditions
Released
• lead/facilitate the completion of respectively owned action items within the agreed timeframes
• assume collective responsibility for advice through; working together in a collegial manner; seeking
consensus on provision of advice wherever possible; and noting any unresolved differences of opinion,
7
Document Eleven
limitations of evidence or opportunity for consultation, or concessions made due to time or logistical
constraints
• exercise all due professional care and diligence in the performance of their obligations under these
Terms of Reference in accordance with the standards of skill, care, and diligence normally practised by
suitably qualified and experienced persons in performing services of a similar nature.
• to make themselves available for meetings convened for the purpose of providing advice to the Ministry
as described above.
Duties and responsibilities of an Ex Officio Advisors of Therapeutics TAG
Therapeutics TAG Ex Officio Advisors are employees of the Ministry who hold specialist technical positions in a
relevant field. The Ex Officio Advisors are appointed by the Chairperson.
The Ex Officio Advisors agree to:
• represent the Ministry by presenting requests for advice or commissioned pieces of work and providing
relevant background information, context, and communications to support the Members in providing
advice which is shaped for the question or issue at hand
• familiarise themselves with background material (if any) sent prior to meetings
• share expert knowledge and engage constructively in discussions, acting only in the role they are
representing and within their scope of expertise
• communicate relevant information, activities, decisions, and issues of interest from the Ministry to
Therapeutics TAG, and vice versa, th ough endorsed communication channels and methods
• individually ensure familiarity with and provide advice congruent with the principles and obligations of
Te Tiriti o Waitangi in ensuring the active protection of Māori health and achieve equity across access,
quality of care and outcomes
• ensure that all activity and advice is undertaken with consideration of and respect for equity of
outcomes across all peoples of Aotearoa New Zealand, including but not limited to; ethnicity, dis/ability,
geographic location, age, gender, health, and socioeconomic position, living and working conditions.
under the Official Information Act 1982
Secretariat of Therapeutics TAG
The Secretariat is not a Member of Therapeutics TAG but supports the group and the Chairperson with
secretariat duties including
• disseminating information required for each meeting
• writing-up the agenda as directed by the Chairperson
Released
• writing the minutes and disseminating these within the group
• updating any new Members or additional Members with the Terms of Reference
• receiving and storing the Conflict of Interest declarations
8
Document Eleven
• receiving fee claims and organising fees payments
• assisting the Chairperson with the onboarding arrangements with Members.
Advice and Other Requests
On occasion, Therapeutics TAG Members may be asked to complete a distinct piece of strategic or proactive
work in an area of expertise.
Any work requested from the Therapeutics TAG Members will be formally commissioned by the COVID-19
Health System Response Directorate of the Ministry.
Requests for Advice can come from sources across the Ministry and from external agencies, and these will be:
• triaged by STA for suitability of input from the Therapeutics TAG
• formatted in a standardised manner, detailing the topic, any backg ound information or context, and
specific questions for the advice being sought.
In order to develop robust advice that is fit for purpose, the Ministry may seek wider consultation or peer review
of technical, clinical, scientific advice provided by Members of the Therapeutics TAG.
Therapeutics TAG Members may be asked to recommend experts with appropriate specialist health or technical
expertise who could be invited to comment or review Therapeutics TAG advice. Additional targeted consultation
with Māori will be resourced and utilised in conjunction with Māori advisors and the Manager of STA.
All other targeted consultation will be facilitated by the Ministry. A register of Therapeutics TAG meeting
reports, requests for advice, commissioned work, activity progress, and advice will be maintained by STA staff.
Meeting Protocols
under the Official Information Act 1982
Secretariat
The Ministry will ensure adequate secretariat support and other support as may be required from time to time,
for Therapeutics TAG to carry out their mandate efficiently and effectively.
Meetings logistics
Released
Coordination of the meetings will be managed by the Secretariat through direction of the Chairperson. This will
include all the logistics, documentation, and administration. Members will receive relevant documentation
through email or other digital tools used within the Ministry.
9
Document Eleven
Members must have regular access to electronic and digital tools in which Therapeutics TAG meetings are
conducted. Meetings conducted in workplaces must remain confidential and not visual or audible to workplace
colleagues.
Delegates
Members will attend all meetings whenever reasonably possible and delegates are not permitted. Apologies
must be in writing (email) to the Chairperson and Secretariat prior to the meeting.
Other attendees
Guests with relevant expertise may be invited to discuss specific issues and when attending the whole meeting
will abide by the same Terms of Reference.
Non-Members may only attend by invitation of the Chairperson.
Quorum
A meeting quorum for Therapeutics TAG requires 50% of standing external Members, including the Chairperson.
The quorum for a meeting is the minimum number of Members required to make the meeting valid. If a meeting
is inquorate, it cannot make recommendations on behalf of the group. It can hold discussions and make
recommendations for later confirmation or rejection by the group.
Official Information Act requests
All agendas, emails and other communication and information relating to the Network are subject to the Official
Information Act 1982, and the Ministry may be required to release such information on request unless there are
valid reasons for withholding the information under the Act.
Fees Framework
under the Official Information Act 1982
The daily rate has been set in accordance with the Ministry’s Fees Framework and has been approved by the
Director-General of Health and may be paid to Members who are self-employed or privately employed.
Members who are paid for their time/employed through the wider state sector (eg they work for Universities,
District Health Boards, Government departments and State agencies) are not personally eligible for a fee,
although on the production of an invoice, the Ministry can reimburse a government-funded agency employing
organisation for the Member’s time.
Released
The membership register will indicate those Members that are eligible to claim a fee under the Fees Framework
and the level of the fee, based on the above declaration.
10
Document Eleven
A working day of eight hours is the basis of the daily fee calculation, with hourly pro-rata rates calculated
accordingly. A working day of longer than eight hours does not attract extra payment beyond the daily fee. The
daily fee applies to all work, including the work performed outside of meetings that is required for the group to
carry out its role (e.g. preparation, representing the group at other forums, or administrative work).
All fees and expenses (where agreed) are to be submitted either on a Ministry claim form or as an invoice.
Reasonable expenses are to be agreed in writing in advance and should be supported by tax invoices and/or
receipts.
Payments will be made in accordance with the Ministry’s accounts payable guidelines.
Work outside of meetings that has been formally commissioned by the Ministry will be formally described in a
written request with anticipated days or hours of work required and the fee rate, which the individual or group
may accept or decline. Additional days or hours of work required must be agreed in writing with the Manager of
STA prior to commencement of the hours worked.
Guidance on organisations that form part of the wider state sector can be found on the SSC website.
For more information, please refer to the Cabinet Fees Framework.
Review of Membership
Membership of s TAG will be reviewed by the Deputy Chief Executive TAG Health System Response Directorate,
on or before September 2022.
under the Official Information Act 1982
Released
11

Document Twelve
under the Official Information Act 1982
Released
Document Twelve
under the Official Information Act 1982
Released

Document Twelve
under the Official Information Act 1982
Released

Document Twelve
under the Official Information Act 1982
Released

Document Twelve
under the Official Information Act 1982
Released

Document Twelve
under the Official Information Act 1982
Released

Document Thirteen
•
Pharmac are in active discussions for five or six other medicines, including antivirals,
monoclonal antibodies, and baricitinib. Discussions are reaching the stage of
confidentiality agreements which wil limit how much information can be shared with the
wider group. Information can stil be shared with STA to assist with monitoring.
•
Pharmac noted a member’s comments about a smal minority of patients for whom
baricitinib is not a suitable treatment option due to certain comorbidities. It was suggested
that it would be helpful to get an indication of the potential size of this cohort. Developing
guidance for baricitinib was suggested.
ACTION: Group to consider the development of guidance for the use of baricitinib.
•
A member raised the issue of use of baricitinib, proportions of hospitalisation and numbers
of people who are mechanically ventilated due to advanced renal failure. It was noted that
pregnant people are excluded from those studies. The future use wil be dependent on the
next outbreak and the populations affected. Given the vulnerable populat on that COVID-
19 is affecting in the current outbreak, pregnancy, late presentation, and advanced kidney
disease should be anticipated.
•
The Chair noted feedback received; a reminder to consider paediatric formulations and
what would be used in such situations. Noting that this is infrequent, but helpful to be
aware of.
3.0
Therapeutics: Prioritization Criteria
STA raised the discussion points that were signalled in the ‘Therapeutics Prioritisation Criteria’
document circulated with the agenda.
•
STA suggested a staged approach for the criteria using three criteria:
1. Evidence of
effectiveness,
5. Magnitude of benefit, and
6. Magnitude of ADRs relative to context.
Looking at evidence for efficacy and safety first and once they meet the required threshold,
continuing to analyse the other domains.
o The group generally agreed with this, with a member noting that magnitude of benefit
is the key aspect of how to prioritise an agent when several have evidence of efficacy
and safety. The group noted that the feedback around how to apply them in practice
would be helpful to receive.
•
In monitoring evidence of efficacy (and safety) does the TAG anticipate
appraising/reviewing trial findings? How would this process be managed/resourced? Or is
the view that it is appropriate to wait/use other panels for this e.g., living guidelines groups
internationally?
o The guideline group is monitoring literature and international evidence, but it is helpful
to have support around accessing trials and international guidelines. It was suggested
systematic support would be helpful going forward.
o A member noted that if more than one living guideline has recommended a treatment
under the Official Information Act 1982
based on their meta-analysis, that should escalate it for priority analysis, so that the
approach remains current. However, this approach shouldn’t automatical y exclude
evidence from single studies if they are powerful and deemed appropriate for
consideration.
o The group raised the need to prioritise Māori and Pacific input in this space, especially
regarding research about adverse reactions, to ensure these are communicated
appropriately to different communities.
•
Does ‘Addressing a key purpose for NZ’ in criterion
8 Favourable features for pipeline
Released
agents belong here or is does it more relate to horizon scanning of therapeutics in early
phase trials?
o The group advised that this relates to horizon scanning, but also thinking about
priorities, being able to alert to agents that might be important. Consider the best
approach for obtaining treatments quickly if needed.
Document Thirteen
The group had general discussion about the prioritisation of therapeutics.
• STA noted that there is communication with the UK regarding therapeutics.
• It was noted effectiveness and magnitude of benefit are separate and should be evaluated
separately with consideration to number needed to treat and cost benefit analysis.
• A member suggested that as the COVID-19 landscape in Aotearoa New Zealand changes,
it wil be increasingly important to think about where therapeutics can and wil be used
(e.g., outside of hospitals), as well as addressing the needs of different communities. It
was also noted that there are equity issues involved, such as access to care and late
presentation to hospital.
• A member suggested that when reviewing therapeutics, it would be useful to have scoring
table at the top, with areas of interest so it is clear what they are.
• Members suggested that reviewing a range of therapeutics for each severity was important
to ‘diversify the portfolio’ of therapeutics, in case the evidence changes or supply issues
arise and a modification in approach is required.
• Members highlighted the importance of focusing on treatments in the community that
prevent hospitalisation and treatments in hospital that prevent mortality.
ACTION: STA review feedback of prioritization criteria, consider furthe draft.
4.0
Guideline Update/Patient information update
• The Interim Guidance - Clinical Management of COVID-19 in Adults was updated on 24
September 2021.
• The group intends to update the guideline fortnightly initially, then progress to a monthly
update or reactively as required.
• For the next update the group wil focus on any potential changes in recommendation for
the use of budesonide. Pharmac has indicated there is capacity to supply a sustained
increase.
• It was suggested tha it would be useful to have some signal ing around the use and
availability of baricitinib, in preparation for any potential changes.
• As noted in previous minutes, there has been suggestions to incorporate pregnancy into
the guideline. A member suggested that there are several options in how this could work
which would be circulated to the group.
ACTION: Chris Hopkins to circulate options for incorporating pregnancy into the Interim Guidance -
Clinical Management of COVID-19 in Adults.
under the Official Information Act 1982
• There are several obstetric physician colleagues who may be interested and available to
contribute to the guidelines working subgroup. STA noted that bringing members on as
part of the working group (but outside the Therapeutic TAG membership) could be
facilitated.
ACTION: Chair to contact obstetric physician col eagues regarding contribution to the guidelines
working group.
• The group discussed membership general y and noted that there may be a requirement for
Released other involvement as the COVID-19 situation changes.
• The Chair noted that there had been some discussion of documenting the decision making
involved in developing the guidelines.
Document Thirteen
ACTION: Anne Buckley to talk to Tim Cutfield regarding documenting guideline group decision
making.
Patient information update
• There is a scoping discussion on 08 October 2021 to form a subgroup with the Health
Navigator team and those who have been working on resources that are being used in
hospitals.
• The aim is to put forward a proposal to set aside budget for this patient information update
work so it can progress. The team have recently done similar work for a new therapy, so
they have already thought through some of the likely challenges.
• The group noted that this would be a very useful and widely used document once
complete.
5.0
Equity Considerations
Pasifika representative-led discussion
• A member raised an issue for consideration when exploring the use of budesonide. It was
suggested that the age cut-offs in the Australian Living Guideline may not be appropriate
for the Aotearoa New Zealand context. Using these age cut-offs could create an equity
barrier for Māori and Pacific peoples, who may develop disease earlier.
• There was discussion about the use of ‘over 50 with comorbidities’ criteria and if that
would help in this situation, However the group agreed that it would be beneficial to
recognise earlier onset of comorbid disease by adjusting both of the age criteria from
PRINCIPLE to be reduced by 10 years for Māori and Pacific patients. (40 vs 50 years with
comorbidities and 55 vs 65yrs without)
• The group acknowledged that this adjustment would be stepping outside of the trial
evidence but noted that the risk of introducing hazard was low, and the change seemed
beneficial based on clinical experience. If a change was operationalised, ongoing
surveil ance of outcomes would be helpful. A member noted that this would align with what
Auckland MIQ group decided to do, with similar reasoning as above.
ACTION: Guideline working group to consider these suggestions of more equitable age criteria
when exploring the use of budesonide.
• The Chair suggested the group should write to Māori and Pacific health care providers to
give more information about what the TAG is doing. Members agreed this would facilitate
further feedback and important aspects to consider. It was suggested to also include Māori
and Pacific Pharmacy Associations, and Te Rōpū Whakakaupapa Urutā.
under the Official Information Act 1982
ACTION: Saleimoa Sami and Jessica Keepa to draft a letter to be distributed to Māori and Pacific
health care providers from the group.
6.0
Therapeutics: Clinical Trials Including in Primary Care/Community
• No update given.
• The group had general discussion about reducing stigma of receiving a positive COVID-19
test and the important role that Primary Care wil continue to have in the future.
Released
7.0
Next Steps/Other Matters
• A member noted that they wil report back to the group regarding the Australasian COVID-
19 Trial (ASCOT).
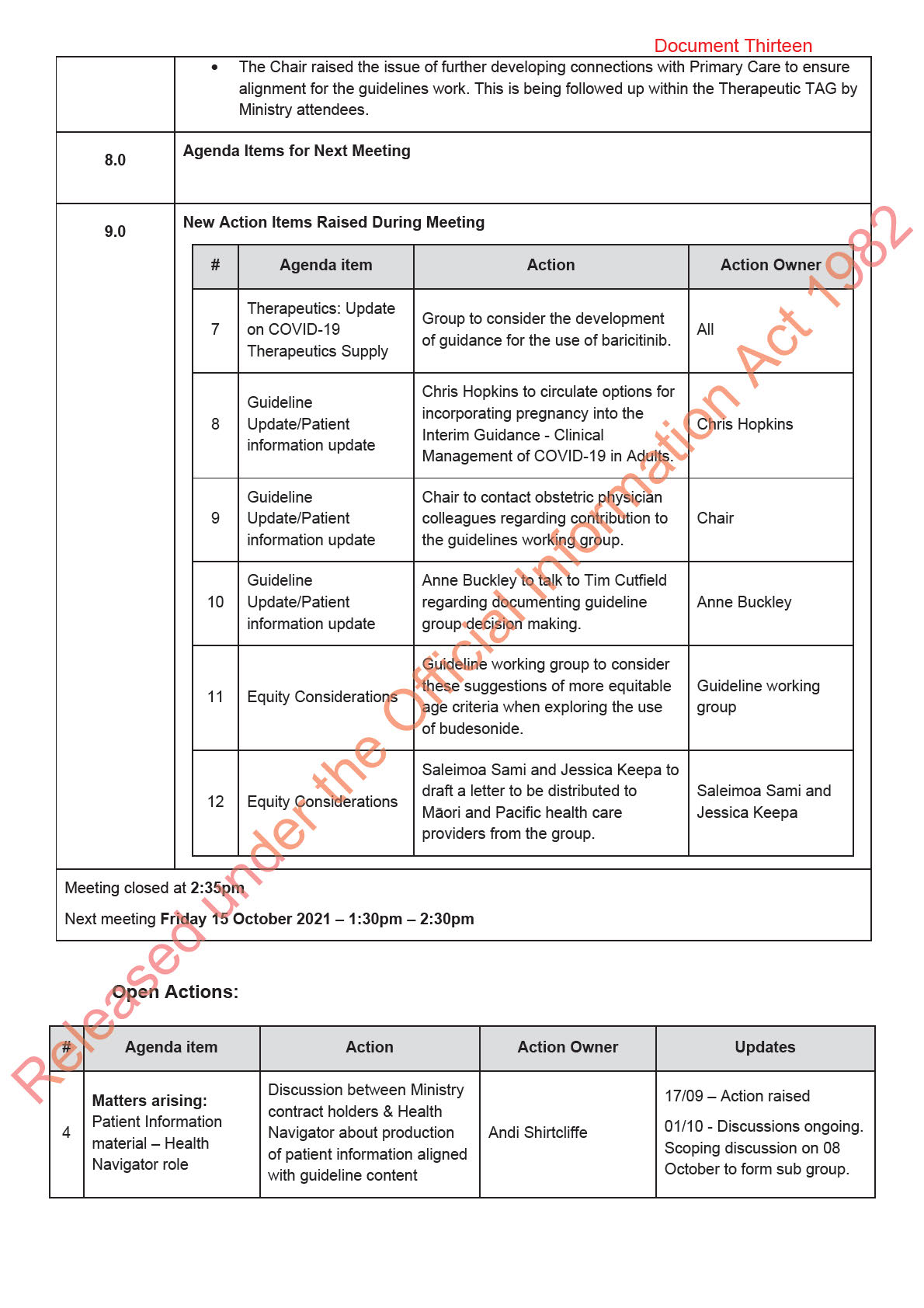
Document Thirteen
Review update and publish
17/09 – Action raised
5 Guideline update
Tim Cutfield/STA
revised guideline
01/10 - Next update 8/10/21
17/09 – Action raised
Therapeutics:
Preliminary testing of
6
STA
01/10 – STA review
prioritisation criteria
prioritisation criteria
feedback, consider further
draft.
Therapeutics: Update
Group to consider the
7 on COVID-19
development of guidance for All
01/10 – Action raised
Therapeutics Supply
the use of baricitinib.
Chris Hopkins to circulate
options for incorporating
Guideline
pregnancy into the Interim
8 Update/Patient
Chris Hopkins
01/10 – Action raised
Guidance - Clinical
information update
Management of COVID-19 in
Adults.
Chair to contact obstetric
Guideline
physician colleagues
9 Update/Patient
Chair
01/10 – Action raised
regarding contribution to the
information update
guidelines working group.
Anne Buckley to talk to Tim
Guideline
Cutfield regarding
10 Update/Patient
Anne Buckley
01/10 – Action raised
documenting guideline group
information update
decision making.
Guideline working group to
consider these suggestions
Guideline working
11 Equity Considerations of more equitable age criteria
01/10 – Action raised
group
when exploring the use of
budesonide
Saleimoa Sami and Jessica
Keepa to draft a letter to be
Saleimoa Sami and
12 Equity Considerations distributed to Māori and
01/10 – Action raised
Jessica Keepa
Pacific health care providers
under the Official Information Act 1982
from the group.
Released
Document Fourteen
• Was advised to use existing information where available.
• STA have staff involved with a ‘Lived Experience’ group which may be able to provide
input/review.
2.0
Therapeutics: Update on COVID-19 therapeutics supply
• Tocilizumab – Pharmac continuing to work with Roche and wholesalers on supply. Stock
in hand likely to be adequate for residual RA users and current outbreak on current
estimates.
Query about access to tocilizumab approved for manufacture in India. This reflects Roche waiving
rights to allow manufacture of tocilizumab for low-income and middle-income countries. Wil
therefore not factor into NZ supply issues.
One member raised the issue of more definitive communication to the sector given clinicians
concerns about supply. Further communications expected from Pharmac – initially via hospital
pharmacists who may also be monitoring that the use of tocilizumab conforms to the priority use
for COVID-19 and the selected subgroup of patients with RA.
• Baricitinib – discussion progressing with Eli Lily. Supply likely to be achieved ‘in weeks’.
Company needing support around S29 requirements. Pharmac working towards having
baricitinib available as a ‘back-up’ option, with a reserve in place to counter any increased
tocilizumab demand (e.g., if further/extended outbreak) or increased difficulties with
supply.
• Ronapreve & sotrovimab – progressing discussions with suppliers. Timeframe for supply
of Ronapreve likely to be some months away
• Pfizer & GSK – Pharmac are in discussion about some other agents but not able to
provide further information at this time due to confidentiality requirements.
• Remdesivir – looking to have good supply. One member commented that one trial now
showing no benefit. Recognised that the time required to put supply in place for a drug
means that new evidence may emerge to support or counter its use over that time period.
• Acknowledged that Pharmac are working hard to access all potentially useful medicines
and that prioritisa ion for use can come from the Therapeutics TAG. The work being done
in the criteria for prioritisation and by the Therapeutics TAG in general serves to keep
Pharmac informed on potential supply/distribution needs.
3.0
Therapeutics specific agents
1. Inhaled budesonide
• Noted that the Australian Living Guideline has a new Conditional Recommendation on use
under the Official Information Act 1982
of inhaled budesonide.
• Some discussion of the certainty of the evidence showing budesonide reduces the need
for supplemental oxygen. One member stated that there is evidence for symptom
reduction but the evidence is less clear for use preventing hospitalisations.
• The guideline subgroup previously considered whether or not to include budesonide in the
guideline and it was omitted. Decision to include wil be reviewed again ahead of the next
guideline update/review for those with mild COVID-19 symptoms. Guideline update/review
expected date 24 September.
Released • Pharmac note that there is a potential to disadvantage other users. If inhaled budesonide
is to be included in guideline, Pharmac would like to be advised and would consider a
restriction to the Pharmaceutical Schedule.
Document Fourteen
• One member commented that the dosing should be 800 mcg b.d. (with the 400 mcg
inhalers prescribed). The Symbicort inhaler (budesonide/formoterol) should not be
prescribed for the COVID-19 indication.
ACTION: Inclusion of inhaled budesonide to be considered for the guideline update of 24 Sept. If
included, Pharmac to be advised by Therapeutics TAG.
2. remdesivir (access criteria)
• Identified that the access criteria specified in the guideline differs from that specified by
Pharmac. Member suggested that Pharmac change criteria to align. Pharmac have
reviewed and decided their criteria needs to remain as is – based on Australian criteria
Use of remdesivir a clinical decision and therefore no conflict in having more ‘restrictive’
use specified in the guideline.
• No change to either guideline content on remdesivir or Pharmac access criteria to be
made fol owing this discussion.
3. Ronapreve, sotrovimab
No further comments/discussion.
Therapeutics: Criteria for prioritisation
STA thanked members for their work on the criteria for prioritization of therapeutics which was
collated during the week and circulated with the agenda. The intention was to use the criteria table
to create a checklist and STA reported they would test the criteria against some of the specific
agents identified in the prioritisation document as of interest to members to monitor (nafamostat,
inhaled budesonide/ciclesonide (ou patient use), fluvoxamine, colchicine (outpatient use),
bamlamivimab plus etesevimab monoclonal antibody combination).
ACTION: STA wil provide further feedback on application of prioritisation criteria at next meeting.
4.0
Guideline Update: Feedback/pathways
Guideline update planned by 24 September. Guideline subgroup wil review whether to include
budesonide in th s update.
A member reported that a colleague at Middlemore has experience of ‘obstetric COVID’ through
managing cases in the current Auckland outbreak. Col eague has put together some guidance on
management for this patient group. Suggested this person could be invited to participate in a
guideline subgroup meeting to look at whether any information should be integrated within existing
under the Official Information Act 1982
guideline or kept as a separate piece of guidance.
5.0
Next Steps/Other matters clinical trials in primary care/community
Discussion of to be included in agenda for next meeting.
Agreed that meeting schedule would now be fortnightly – next meeting Friday October 1. 1.30-
2.30pm.
Released No other business.
6.0
Agenda Items for Next Meeting
Therapeutics: Prioritization criteria – feedback/further discussion.



Document Fifteen
Discussion
• Could be similar to NZF 1 pg format – medications for use in COVID-19. Name of drug,
why given, how given etc.
• Specific therapeutics used in COVID-19 rather than agents used for other aspects of
general patient care.
• A UK patient information example is broader than specific therapeutics only.
• Need for any information prepared to be in different languages. Of note, there are a large
number of Samoan patients in the current outbreak.
• Pictorial information recognised as helpful.
The Chair asked STA what options for the development of patient information exist/are typical.
These include:
− Canterbury Medicines Information Group – tend to be as described in bul et point one.
However, only produced for approved medicines.
− Some DHBs produce patient information about medicines.
− Health Navigator – this approach may have potential.
In addition to patient information material, need to also consider wider cultural services
available/being used. RNZCGP has offered MIQ the support of a roster of Pacific GPs to assist.
4.0
Therapeutics: Update on Supply of Immunomodulators
Update on supply of immunomodulators – Pharmac
Tocilizumab - Pharmac liaising closely with manufacturer and distributing what is available. NZ
Rheumatology Association (NZRA) have a statement in place to guide practice – reducing use for
rheumatological indications.
Baricitinib – promising discussions with manufacturer and looking to obtain supply. Stil some work
to address s29 requirements.
Remdesivir – additional supply obtained. Powder that needs reconstitution. More information wil
be available on the Pharmac website.
Sarilumab – stil following up with manufacturer acknowledging Therapeutics TAG preference for
sarilumab as alternative to tocilizumab. Supply this year looks unlikely.
Overall, adequate supply of tocilizumab or an alternative looks achievable – especially if COVID-19
case numbers in hospital shrink rather than grow.
under the Official Information Act 1982
5.0
Therapeutics: Pre-hospital e.g. Casirivimab & imdevimab (REGEN-COV, Ronapreve),
sotrovimab – logistical issues
Pre-hospital e.g. Casirivimab & imdevimab (REGEN-COV, Ronapreve), sotrovimab – logistical
issues
See 2 slides attached prepared to inform the meeting discussion.
Pre-Hospital
treatment consideratio
Released
• Pre-hospital mainly applies to MIQ at present but over time may involve the community
more widely
• Primary care access and equity – need to avoid postcode inequities.



Document Sixteen
Medsafe is an ex officio advisor to the Committee and has a role in advising on regulatory
matters.
2.0
Therapeutics: Briefing for government
Therese Egan Principal Policy Analyst, System Enablers, Public Health System Policy at the
Ministry attended as a guest. Therese has shared her presentation with the Therapeutics TAG
(attached) – note it is confidential to the Therapeutics TAG.
In her role, Therese prepared a briefing paper for the ministers on the current therapeutics
situation for COVID-19. She acknowledged the very active work being undertaken by Pharmac in
this space and the work of the Therapeutic TAG in providing expert advice.
Therapeutic supply:
The need for active supply management was acknowledged given supply pressures on
therapeutics global y. In looking at what further NZ could do, a number of additional measures
were noted including actively facilitating entry of products evidenced and approved international y,
and the potential for pooled advance purchase agreements (akin to the COVAX approach).
Collaboration with groups international y:
This was raised for discussion. It was noted that members all have international connections &
collaborate through professional contacts and organisations.
Clinical research:
Members were asked whether there was further potential for engagement with clinical research.
There is current involvement of members in trials, including ASCOT and REMAP-CAP.
One member noted that many of the therapeutics being used overseas are not currently available
in NZ and this is a potential limitation.
One potential research gap suggested was in the pre-hospital setting e.g. budesonide is being
used but not in the context of a clinical trial.
A member commented that there is a lot involved in the setting up of a clinical trial, including
engagement with DHBs. This is particularly difficult given competing priorities in the pandemic
situation.
Therese Egan mentioned that Pfizer are currently looking at Phase 2 & 3 clinical trials of an oral
antiviral and suggested this one may be of interest to NZ clinicians to engage with.
under the Official Information Act 1982
Therese welcomed any further feedback from the Therapeutics TAG on the topics of her
presentation.
3.0
Therapeutics: Update on Regulatory Issues, Update on supply issues, and Stock
Holding/Projections
•
Update on regulatory issues:
Medsafe representative provided an update of regulatory issues of relevance and advised that if
the Pharmac or the Therapeutics TAG made a recommendation about a specific drug/s, then
Released Medsafe would give priority to addressing any regulatory issues pertaining to it. The details of the
content presented are included in the Appendix.
•
Update on supply issues:
Pharmac representative advised on current supply/supply issues:
Document Sixteen
Dexamethasone – widely used international y and for many indications. No problem with global
supply or NZ supply currently or expected.
Tocilizumab – supply shortages expected later in year. Pharmac have been in discussion with
Roche but high demand worldwide. Noted by the group that Australia have already declared a
critical shortage. Pharmac have also been in discussion with rheumatologists to free up existing
supply for COVID-19 treatment.
Sarilumab – Pharmac have been in contact with manufacturer Sanofi. Wil continue to explore but
not looking likely in terms of achieving ready and prompt supply.
Baricitinib – Pharmac fol owing up supply with some urgency.
Sotrovimab – Pharmac are in discussion with GSK about potential supply.
REGEN-COV Casirivimab + imdevimab – Pharmac expect supply more readily available.
Remdesivir – need for supply acknowledged. No specific supply status minuted.
•
Stock holding/Projections
Questions were raised about the quantity of tocilizumab supply – definitely have some weeks of
supply. Rheumatologists supportive of re-distribution – approximately 10-15% wil have to be
retained for use in rheumatology patients.
•
Alternatives to tocilizumab Information on baricitinib and sarilumab was circulated to the membership in the STA-produced
paper included under agenda item 4.0
Discussion
Agreement of Members that need to have at least one of the 3 immunomodulators (tocilizumab,
sarilumab, baricitinib) available for t eatment of patients with COVID-19 in the hospital setting.
These were identified as the top 3 therapeutic priorities (in the order listed) although Pharmac’s
update on supply issues with sarilumab was acknowledged.
One member suggested that may be helpful to have Ministry issue advice to the sector that priority
use for tocilizumab be for COVID-19 treatment.
4.0
Therapeutics: Further prioritisation of Key Therapeutics
Further prioritisation of key therapeutics
See STA paper circulated.
Discussion
under the Official Information Act 1982
REGEN-COV:
It was noted that the administration route of IV infusion could create some chal enges in the pre-
hospital setting and if recommended by the membership would require planning to put in place
clear clinical pathways.
Remdesivir:
Released Discussed that for mild to moderate severity only; not of benefit for those with severe COVID-19.
Issue raised is how to get it to those who need it earlier ie. in the community. Noted that if looking
at IV infusion delivery for REGEN-COV that may allow consideration of IV remdesivir in the pre-
hospital setting also.
Document Sixteen
Sotrovimab – likely to be included in priority list. Not discussed further.
5.0
Equity considerations Māori & Pasifika representative-led discussion
Dr Jessica Keepa identified 3 actions for the group to consider:
1. DHBs having a statement on institutional racism
2. Collection of ethnicity data on al patients with COVID-19
3. Information available for families on therapeutics, reflecting the guideline.
The Chair noted that DHB initiatives would be outside the scope of this group’s ToR. The
COHESION cohort study has collected previous inpatient case information, thought likely including
ethnicity. In discussion, the information for families was supported as an extra piece of work that
could be undertaken by a small group. Having it available in multiple languages was noted as
desirable especially given difficulty in accessing interpreters.
Further consideration/action on information for families/whānau once the guideline is finalised.
Dr Saleimoa Sami raised issues in relation to the treatment of Pasifika patients:
• Protocols and equity – protocols tend to be a ‘one size fits al ’ approach. Using the example of
remdesivir for mild to moderate COVID-19, could the protocol create a barrier to access for
Pasifika? Some discussion about the relative benefits of remdesivir followed.
Outcomes in Pasifika with COVID-19 – Dr Sami stated that there have been high mortality rates
documented in Pasifika people e.g in the US compared with the general population. Need to
ensure the needs of Pasifika patients in NZ with COVID-19 are met, with ‘protocol’ modifications if
needed.
6.0
Guideline – Feedback from Working Group
Guideline – feedback from working group
A draft of the revised guideline was circulated ahead of the meeting. The Guideline subgroup were
thanked for their work and achieving rapid progress on it.
The Guideline subgroup have had two meetings. Tim Cutfield has facilitated those meetings at the
Chair’s request and has collated al the feedback received.
The draft document is close to final but the following input is needed:
1. Equity perspective – our equity representatives in particular were asked to review the
guideline with an equity lens
under the Official Information Act 1982
2. Pharmac – need to ensure aligns as necessary with Pharmac documents (Schedule)
3. Public Health input
4. Post hospital care – adding information on this is in hand.
Any further feedback on the guideline draft circulated to Tim asap.
The query was raised as to who would host the guideline and how would this be communicated to
colleagues. The CSA advised that once the guideline was finalised the Ministry would be able to
Released host the guideline (as an html document) and to disseminate news of the guideline via CMOs,
CNOs, pharmacy managers and others to whom the guideline is relevant.
The Chair proposed that the guideline be uploaded (‘published’) without wider consultation given
urgency. However, a plan to take in any feedback provided could be formulated. The benefit of any
feedback being col ated by professional organisations/associations (rather than coming from

Document Sixteen
12.0
Appendix 2: Summary information provided by Medsafe for Therapeutics TAG Minutes 3
September 2021 (relates to item 3.0.)
A verbal update of this information was provided to Therapeutics TAG meeting 3 September 2021
Medicines Approval
• The Medicines Act 1981 generally requires medicines to go through an approval process
(operated by Medsafe) before they can be supplied. Approval is the best option for the
supply of medicines as this gives confidence that the NZ regulator has assessed the
particular product to ensure it meets internationally agreed standards of quality, safety and
efficacy. There are exemptions to the requirement for approval.
• There are two approval processes – section 20 (s20) is the standard approva process and
almost all medicines fol ow this route. Section 23 (s23) is a provisional approval route
which requires a smal er data set for approval (commonly but not exclusive y, abbreviated
clinical trial data) and is used where the benefits of having a medicine outweigh the risks
presented by the lower assurance of limited data. This form of approval is time limited with
a maximum period of 2 years, after which it can be renewed. Provisional approval is often
issued with conditions. An example is the approval for the COVID-19 vaccines.
• Section 20 approval requires a substantial data set and usually takes some time with
Medsafe often asking the company for additional information. Applications are usually
queued, however the priority can be changed based on urgent clinical need. It is also
possible to speed the approval process if the medicine has already been approved by an
overseas regulator Medsafe recognises (though this may depend on the type of approval
given – emergency use authorisation overseas is not acceptable). Medsafe may also
accept a ‘rolling submission’ process where a company wil supply data as it becomes
available. Medsafe and PHARMAC discuss approval timelines on a regular basis under
an existing MoU.
• For both types of app oval Medsafe must receive an application from the company
wishing to import and sell the medicine. This company (the Sponsor) must be based or
have a registered office in New Zealand.
• Worth noting that it is a product (‘medicine’) that is approved, not the use of the active
ingredient. This means that a second product with the same active ingredient wil also
need to be specifical y approved.
• Timelines are dependent on the above factors and are often driven by the company’s
response to requests for information. Medsafe policy is to ensure COVID-19 matters are
prioritised.
under the Official Information Act 1982
Use of unapproved medicines (or use of approved medicines for unapproved indications)
• Note that approved products can be used by clinicians for unapproved indications. While
the company supplying the product cannot advertise the unapproved indication, a clinician
with prescribing rights can use professional judgement to prescribe / use the product in
particular patients. No prior approval is required by Medsafe and no post-use reporting is
required.
Released • A description of how unapproved products and how approved products can be used for
unapproved indications is available at: http://www.medsafe.govt.nz/profs/RIss/unapp.asp.
• There are two principal routes by which an unapproved product can be obtained and
used. Supply via section 29 is the most commonly used. This requires a supplier (often
the NZ office of the company that manufactures the product overseas, a wholesaler, a
Document Sixteen
specialist wholesaler or sometimes a pharmacy (Licence may be required)) to import the
product. It can then be supplied on demand into the supply chain. Limitations are that
supply can only be made on the request of a medical practitioner (this does not extend to
other prescribers or prescribing via standing orders) and only for a particular patient. The
details of the patient, prescriber and location must be supplied to the product supplier and
these must be kept. The supplier must provide a declaration to Medsafe each month
about supply activities. The supplier cannot advertise the availability of the product. No
pre-approval from Medsafe is required. While information about the prescribing is
generally required before supply is made, stock can be made available in the supply chain
or lodged with users before these details are known provided there is agreement that the
required details wil be notified back to the supplier when the product is used.
• The less-used route permits a wider range of prescribers to obtain a product directly from
overseas for a particular patient that is known at the time of importation. This requires no
pre-approval, and has no post-event reporting requirement.
• Note that informed consent is a professional practice requirement when using a medicine
not approved for the purpose it is being used.
• It is possible to use a product via the unapproved route whilst an approval process is
taking place.
• An option remains for an unapproved product to be used in a clinical trial – this requires
pre-approval
As the legal aspects of supply are quite complicated (some details have been simplified for clarity)
and depend on circumstances, we are happy to advise on particular situations.
13.0
Appendix 3: Ivermectin – Medsafe Warning (relates to item 8.0)
Link here: http://medsafe.govt.nz/safety/Alerts/ivermectin-covid19.htm
14.0
Appendix 4: RNZCGP statement on Ivermectin (relates to item 8.0)
SUBJECT: Ivermectin and COVID-19
Ivermectin has become the subject of much debate and conjecture in both the popular press and
social media for the treatment of COVID-19. While there is low-quality data that supports further
evaluation of Ivermectin in well-conducted clinical trials, there is as yet no evidence that supports
the use of Ivermectin for treatment of COVID-19 outside the setting of one of these trials.
under the Official Information Act 1982
Additionally, there is reason to doubt these trials wil demonstrate benefit, as the level of Ivermectin
required to inhibit SARS-CoV-2 in-vitro greatly exceeds the highest safe dose in humans.
Off-label use of Ivermectin for treatment of COVID-19 is strongly not recommended.
Ivermectin is a critical medicine for treating some parasitic infections, including
Strongyloides
stercoralis, which can rarely cause life threatening ‘hyper infection syndrome’ in people who receive
immunosuppressive medications. As a result, Ivermectin is regularly used to treat proven or
suspected
Strongyloidiasis in patients who are treated with immunosuppressive medications, which
include many of the proven treatments for COVID-19 (e.g., dexamethasone and tocilizumab). Some
Released people with COVID-19, who have lived in areas endemic for
Strongyloides, receive treatment for this
condition in addition to other COVID-19 specific therapies.
Ivermectin can, and does, cause harm when misused. Prescribing it could well mean that even if
the patient had given consent, the doctor could stil be held liable for making an il -informed decision
on a medication that at this point has not been shown to provide benefit and could cause harm. It


Document Seventeen
• Noted that guidelines for primary care and also for paediatrics (Starship) in development. These
areas not for inclusion but ‘line of sight’ of other guideline work needed to align if/as necessary.
• Focus of this group is therapeutics but recognised that in clinical guidelines, of value to clinicians
to have information on clinical management/severity & other treatments (eg. oxygen therapy)
within same document – as in ‘Middlemore guidelines’.
• ‘Middlemore guidelines’ draw heavily on Australian Living Guidelines and other international
guidelines. Relied on Australia review of the evidence and have not reviewed the individually
studies. Detailed evidence review not within the scope of TOR for Therapeutics TAG.
• Useful aspect is that give ‘heads up’ on ‘escalation’ and therapies needed – without providing
detail, which can be found elsewhere.
• Possibly require more detail on respiratory therapies, including oxygen – to be considered.
• Detailed information available through other sources eg. Health pathways. Could include key
sources/links rather than duplicate information.
4.0
Procurement – Preliminary list
STA provided some explanatory detail about the draft Background paper (based on STA document CSU
42) and Airfinity slides (not for wider sharing due to licensing).
Discussion about the areas where this group can assist and support the wider work of the
Ministry/COVID-19 response:
• Clinical perspective & from clinical trial involvement on potentially useful agents.
• Horizon scanning – initial focus on agents for moderate-severe COVID-19
• Pharmac – well-placed to look at detail of evidence on agents identified as potentially of benefit.
• Issues of supply (Pharmac) – timeliness of procurement process relevant – and of regulatory
process (Medsafe) - Medicines for approval (Medicines Act) vs unapproved medicines access.
• May be useful to do a stocktake of what therapeutics are currently being used in NZ for COVID-
19 treatment.
Discussion about specific agents:
• tocilizumab in use in hospitals treating COVID-19 patients. Increased supply of tocilizumab
required and/or increased access to sarilumab (as an alternative).
• Baricitinib – as a second-line agent? Query safety – monitoring required.
• Sotrovimab – noted that this is going through the approval process in Australia.
General discussion points:
under the Official Information Act 1982
• Concerns raised about therapeutics running low on supply now and need to advise on a plan for
that.
• Of value to see what Australians are doing/using, such as monoclonals approved in Australia.
• Early priorities suggested by a member was first accessing additional tocilizumab, and/or
sarilumab as an alternative, and then if insufficient supply of those two agents, baricitinib.
5.0
GP Guidelines – Line of sight Update
Released
Recognition of need for guidance for GPs on management of patients with mild-moderate COVID-19 in
the community – what agents, when secondary care required, etc.
Work has begun on this in Health Pathways drawing on guidelines in use in Ontario.

Document Seventeen
up supply issue with
wholesaler
under the Official Information Act 1982
Released





Document Twenty
6.0 Any Other Business
5 mins
All
Verbal
7.0 Agenda Items for Next Meeting
Chair
Verbal
Act 1982
under the Official Informatio
Released