
1982
Act
Information
Official
the
under
Released
Document One
•
A comment was raised that a pathway is needed for positive RAT results, which could potential y
overload a laboratory if an overwhelming number of tests come back positive. That is, moving
towards a PCR test to verify if a RAT has yielded a true or false positive is important and also
adds additional strain
•
Remaining actions for recommendations were described.
Chair opened the floor for discussion
•
Some elements of the report have already been overtaken by events that have occurred since its
release. Laboratories are at capacity currently and slightly over capacity in Auckland. Testing will
only continue to increase and likely in the upcoming days rather than weeks to months.
1982
•
Member would like clarity on the communication and when that process wil begin. Requesting
timelines for specific elements of the testing strategy. Another member responded there is a health
navigator to communicate with the public sector currently. Fact sheets wil be available soon.
•
Some iwi have been asking who to speak to for the testing plans and are seeking information on
Act
testing. Ministry to action this item and provided point of contact.
•
Comment was raised that laboratories are under extreme stress and pressure everywhere in the
country and that was without cases outside Auckland. Wel ington has been asked to pick up some
testing to support Auckland. Laboratory staff everywhere are struggling to cope. Testing needs to
shift its balance from surveil ance that is overburdening the system to diagnostic/clinical testing.
•
Member noted that that MIQ day 12 testing is suffering delays, often receiving results several days
later due to longer TAT from all of the community testing.
•
Member noted there are active discussions about Auckland’s outbreak management strategy.
•
A member asked if the report ‘Transitioning to COVID-19 endemicity: Laboratory considerations’
Information
was shared. The Chair confirmed it had been circulated previously but can be provided again to
the TAG.
Testing strategy draft
•
This is a very preliminary draft and wil form the basis of engagement and discussion in the coming
Official
weeks.
•
There are three principles underpinning the strategy: reaching high vaccination, case and contact
management, and testing.
the
•
Feedback requested from the TAG on slides 3, 5, and 6 and can be sent directly to the Science
and Technical Advisory team. Another iteration wil be provided at the next TAG meeting.
o Slide 3: Does the breakdown of the four testing categories make sense?
o Slide 5: Are the proposed testing modalities and surveil ance plan appropriate?
o Slide 6: Do the different testing modalities for different settings and communities make
sense? Are the titles on sections 3 and 4 appropriate?
under
•
Comments from the TAG on the specific slides were:
o It is unclear what bul et point C on slide 3 means. Is this category HCW surveil ance? It
was noted that in low prevalence, NP by PCR is not well tolerated and as a result HCW
surveil ance is only once a week or fortnight when in reality should be every couple of
days. NP by PCR is not a practical strategy for surveil ance. Understand NP by PCR is the
reference standard, especially for finding cases in low prevalence but it creates issues
with laboratory capacity and TAT. Should take advantage of the NPV of RAT. Study on
testing frequencies for different modalities. Science and Technical wil share this study
Released with the TAG.
o It was noted that slides should use NAAT instead of PCR. There were too many
categories that do not help choosing the right test. Should be a risk-based approach. Too
much on technology and not what is trying to be achieved by the strategy.
Document One
o It was noted that the final statement on slide 3 that the future state wil be low symptomatic
rates, low symptomatic testing. This is incorrect – in a future state, everyone with any cold
and flu-like symptoms are considered symptomatic testing.
o It was noted that receiving the documents sooner would be helpful to al ow for sufficient
review of documents like these in the future.
o Additional feedback to be provided in writing to Science and Technical Advisory to share
with owners of the document.
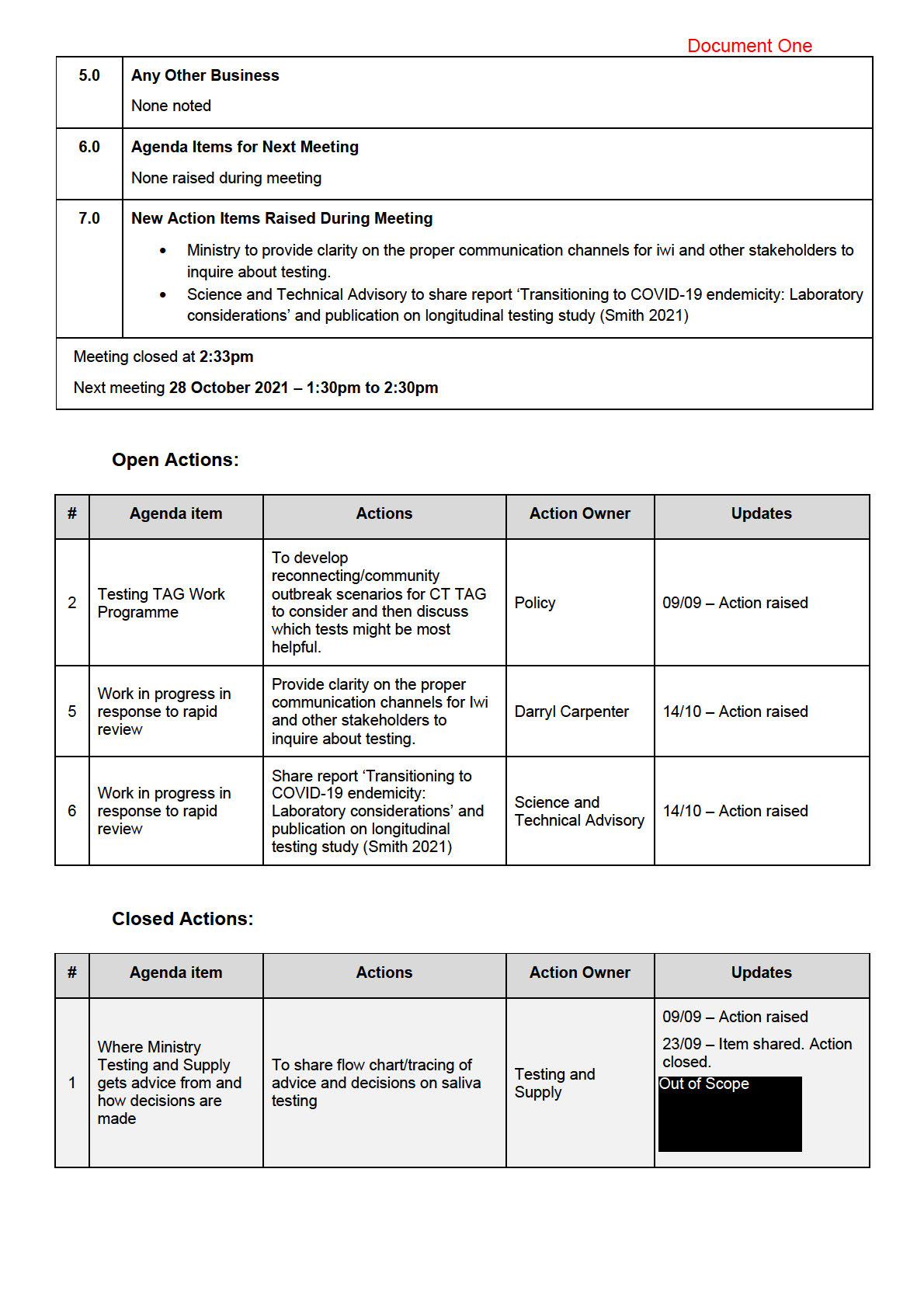
Actions:
• Ministry to provide clarity on the proper communication channels for Iwi and other stakeholders to
1982
inquire about testing.
• Science and Technical Advisory to share report ‘Transitioning to COVID-19 endemicity: Laboratory
considerations’ and publication on longitudinal testing study (Smith 2021)
Act
3.0
Pilot projects for RAT
• Businesses requested to start using RAT. There are 29 businesses on board and are part of the
consortium being run by MBIE. The Ministry of Health is providing advice and input into a charter
that businesses wil agree to. This charter wil ensure public health is managed appropriately such
as use of the tests, resulting, what to do with a positive, etc.
• A member asked where the supply wil come from for businesses. Testing and Supply noted 600k
RAT kits have been ordered and are available for supply, but these are for the public health
response and healthcare. Businesses wil be responsible for their own supply. Business and
health are separate pools.
Information
• A draft of the charter to be used by MBIE wil be provided to Testing TAG at a later date for their
input.
• A member noted saliva has not been approved for RAT. This was recognised as correct but that
businesses are using saliva in Australia and it was an example of protocols from Australian
operations.
4.0
New tests evaluation and approval framework
Official
• Framework described by Testing and Supply
• A member asked how the current 3 RAT kits were evaluated and approved for import and if that
the
same criteria wil be used in this framework.
o It was noted the ESR criteria wil likely be modified to be fit for purpose. Likely part of the
evaluation process will incorporate TGA approval along with a review of literature and
international evidence
• A member questioned who wil be funding the evaluation.
o ESR received funding to source and assess kit performance. This could change in the
under
future and include LabPLUS.
• A member questioned if the role described for the Testing TAG was suitable and aligned with the
TAG’s Terms of Reference. This process appears more operational and not part of TAG’s
responsibilities.
• It was noted ESR or the SME group from NZMN would complete due diligence to confirm
manufacturer claims.
• Testing TAG should not be endorsing every test for import and it was noted not every new test
would need field evaluation.
Released
• A member noted that ESR may not be the best organisation to be completing the evaluation
process. This concern was agreed by multiple members. It was initial y suggested that Medsafe be
in charge of this but another member noted Medsafe would not be involved with this work.
• A request was made that the documents be distributed before the next meeting.
1982
Act
Information
Official
the
under
Released

1982
Act
Information
Official
the
under
Released

1982
Act
Information
Official
the
under
Released
1982
Act
Information
Official
the
under
Released
Document Two
- Roche have provided results of Phase 3 trials to Pharmac. These results documents
are supplied under a confidentiality agreement and therefore cannot be shared with
the Therapeutics TAG at this time. They wil be reviewed by the Pharmac advisory
group and general comments may be shared across the two groups.
• Further discussion points:
- A member commented that wil be important to align the testing and therapeutics
implementation approaches, especial y if/as community-delivered therapeutics
become available.
- A member asked if projections of case numbers from model ing (per admission
rather than bed days) could be made available to assist management of current
1982
supply. This model ing data was circulated electronical y from the CSA via the
Secretariat during the meeting.
Medsafe Update
Act
Medsafe provided an update on the status of COVID-19 treatment applications and approvals.
This included a Medsafe update in relation to the fol owing therapeutics:
• Dexamethasone
• Tocilizumab (Actemra)
• Casirivimab + Imdevimab (Ronapreve)
• Regdanvimab
• PF-07321332 +ritonavir
Information
• Remdesivir
• Molnupiravir
The update is included in ful as an appendix to the Minutes. The main points in relation to each
therapeutic in the update were presented verbally in the meeting.
Official
5.0
Structure for Interface with Primary Care
Justine Lancaster provided an update of work being completed in the Ministry to develop models of
care and also by Health Pathways with the aim of both to provide guidance for primary care.
the
ACTION: CSA requested a brief summary be circulated to the therapeutics TAG of the work being
undertaken in developing models of care for Primary Care.
ACTION: Chair of Therapeutics TAG to meet with lead/s for the Primary Care work to identify next
steps in aligning work. Justine Lancaster to convene meeting.
under
6.0
Community Therapeutics
The focus of discussion was
oral antivirals and the recognition of their potential in ease of
community delivery – compared with the complexity of delivering parenteral treatments in the
community. The Chair acknowledged the wide networking and research interests of group
members and asked members to bring the group’s attention to any emerging treatments as they
come to their attention.
Additional points in discussion:
Released • Horizon scanning: Pfizer oral antiviral (PF-07321332); favipiravir.
Favipiravir – some trials, with reporting expected in next few weeks. Preliminary reports
suggest not as promising as molnupiravir.
Document Two
• Remdesivir supply in hospitals that is not needed could potentially be available for
community use. Remdesivir is administered by IV infusion (over 3 days In Auckland
hospitals). Any use outside hospital setting would require discussion with DHBs re
operational matters etc.
• Importance of socialising information about new treatments before they are ‘rol ed out’,
especial y from an equity perspective to ensure that the value of the treatments are
understood within the community and thus facilitate good uptake.
• Alignment of testing and treatment seen as important in community setting. MIQ facilities
may not be wel -placed to administer IV treatment given pressure of numbers. One
member suggested there would be value in a ‘testing plus infusion centre’. Operational
issues are important considerations.
1982
7.0
Paediatric Therapeutics
The meeting was attended by a guest infectious diseases paediatrician who led discussion on this
Act
topic.
• To date there have been few paediatric cases hospitalised but this appears likely to
increase in the future. Treatments include tocilizumab, steroids, remdesivir.
• Paediatric dosing:
- noted that older children and teenagers often weigh same as adults
- FDA ‘pushing’ for information on paediatric dosing to be provided by drug companies for
COVID-19 treatments
Information
• Molnupiravir:
Queried whether potential for molnupiravir use in children given the trials included people
18 years plus. NZ paediatricians in contact with Australian & UK colleagues on matters of
COVID-19 clinical practice. Royal Children’s Hospital (Australia) currently preparing
guidelines and NZ likely to follow this lead.
Official
8.0
Guideline Update/Patient Information Update
• The latest update of the Guideline was published on the Ministry site for health
professionals on 8 October 2021. Next update planned for 5 November 2021.
the
• Update frequency has moved to a monthly schedule though a more frequent update may
occur if there is a significant recommendation/content change to make.
• Guideline subgroup last met Wednesday 13 October.
• The Chair advised 2 Obstetrics & Gynaecology specialists have been co-opted on to the
under
Guideline Working Group and wil lead drafting of additional content for guideline on
management of COVID-19 in pregnant women.
• A recommendation regarding the use of baricitinib wil be prepared for a coming update,
anticipating availability of this therapeutic in the near future as an alternative to tocilizumab
(if there are tocilizumab supply shortages). Patient population wil be specified.
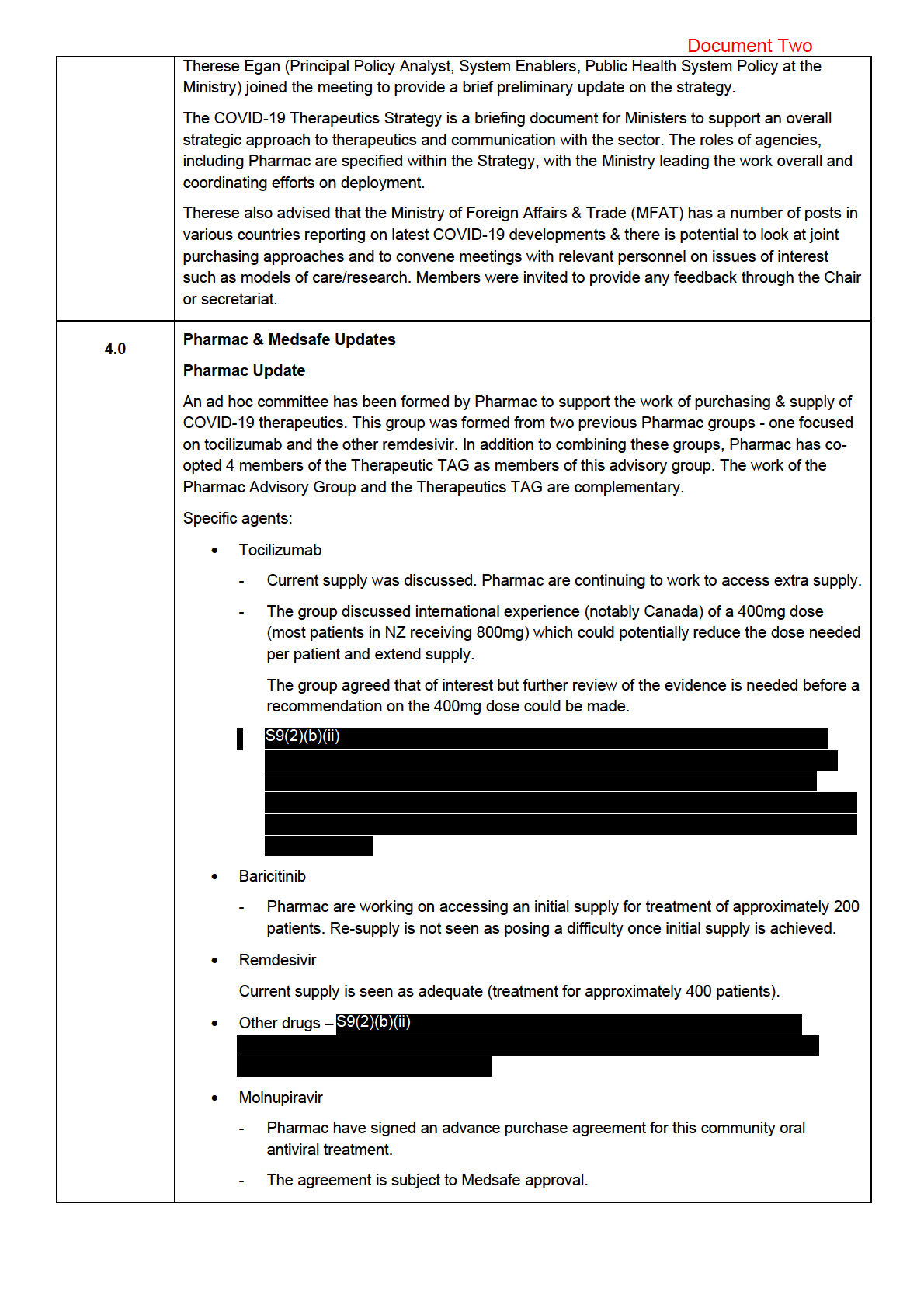
• Budesonide
- It is not currently included in the Guideline but this is under review. Of note, it is
Released now included as a ‘consider’ in the Australian Guideline and Ontario Guideline.
Also noted that the age cut-off of 50 years used in other guidelines may not be
appropriate in the NZ Context. From an equity perspective may be appropriate to
include adults of any age with one or more c-morbidities. There is currently a
1982
Act
Information
Official
the
under
Released

1982
Act
Information
Official
the
under
Released

1982
Act
Information
Official
the
under
Released

1982
Act
Information
Official
the
under
Released
1982
Act
Information
Official
the
under
Released
Document Three
• Pharmac are in active discussions for five or six other medicines, including antivirals,
monoclonal antibodies, and baricitinib. Discussions are reaching the stage of
confidentiality agreements which wil limit how much information can be shared with the
wider group. Information can stil be shared with STA to assist with monitoring.
• Pharmac noted a member’s comments about a smal minority of patients for whom
baricitinib is not a suitable treatment option due to certain comorbidities. It was suggested
that it would be helpful to get an indication of the potential size of this cohort. Developing
guidance for baricitinib was suggested.
ACTION: Group to consider the development of guidance for the use of baricitinib.
• A member raised the issue of use of baricitinib, proportions of hospitalisation and numbers
1982
of people who are mechanically ventilated due to advanced renal failure. It was noted that
pregnant people are excluded from those studies. The future use wil be dependent on the
next outbreak and the populations affected. Given the vulnerable population that COVID-
19 is affecting in the current outbreak, pregnancy, late presentation, and advanced kidney
Act
disease should be anticipated.
• The Chair noted feedback received; a reminder to consider paediatric formulations and
what would be used in such situations. Noting that this is infrequent, but helpful to be
aware of.
3.0
Therapeutics: Prioritization Criteria
STA raised the discussion points that were signalled in the ‘Therapeutics Prioritisation Criteria’
document circulated with the agenda.
Information
• STA suggested a staged approach for the criteria using three criteria:
1. Evidence of
effectiveness,
5. Magnitude of benefit, and
6. Magnitude of ADRs relative to context.
Looking at evidence for efficacy and safety first and once they meet the required threshold,
continuing to analyse the other domains.
o The group generally agreed with this, with a member noting that magnitude of benefit
is the key aspect of how to prioritise an agent when several have evidence of efficacy
and safety. The group noted that the feedback around how to apply them in practice
Official
would be helpful to receive.
• In monitoring evidence of efficacy (and safety) does the TAG anticipate
appraising/reviewing trial findings? How would this process be managed/resourced? Or is
the view that it is appropriate to wait/use other panels for this e.g., living guidelines groups
the
internationally?
o The guideline group is monitoring literature and international evidence, but it is helpful
to have support around accessing trials and international guidelines. It was suggested
systematic support would be helpful going forward.
o A member noted that if more than one living guideline has recommended a treatment
under
based on their meta-analysis, that should escalate it for priority analysis, so that the
approach remains current. However, this approach shouldn’t automatical y exclude
evidence from single studies if they are powerful and deemed appropriate for
consideration.
o The group raised the need to prioritise Māori and Pacific input in this space, especially
regarding research about adverse reactions, to ensure these are communicated
appropriately to different communities.
• Does ‘Addressing a key purpose for NZ’ in criterion
8 Favourable features for pipeline
Released
agents belong here or is does it more relate to horizon scanning of therapeutics in early
phase trials?
o The group advised that this relates to horizon scanning, but also thinking about
priorities, being able to alert to agents that might be important. Consider the best
approach for obtaining treatments quickly if needed.
Document Three
The group had general discussion about the prioritisation of therapeutics.
• STA noted that there is communication with the UK regarding therapeutics.
• It was noted effectiveness and magnitude of benefit are separate and should be evaluated
separately with consideration to number needed to treat and cost benefit analysis.
• A member suggested that as the COVID-19 landscape in Aotearoa New Zealand changes,
it wil be increasingly important to think about where therapeutics can and wil be used
(e.g., outside of hospitals), as well as addressing the needs of different communities. It
was also noted that there are equity issues involved, such as access to care and late
presentation to hospital.
• A member suggested that when reviewing therapeutics, it would be useful to have scoring
1982
table at the top, with areas of interest so it is clear what they are.
• Members suggested that reviewing a range of therapeutics for each severity was important
to ‘diversify the portfolio’ of therapeutics, in case the evidence changes or supply issues
Act
arise and a modification in approach is required.
• Members highlighted the importance of focusing on treatments in the community that
prevent hospitalisation and treatments in hospital that prevent mortality.
ACTION: STA review feedback of prioritization criteria, consider further draft.
4.0
Guideline Update/Patient information update
• The Interim Guidance - Clinical Management of COVID-19 in Adults was updated on 24
September 2021.
Information
• The group intends to update the guideline fortnightly initially, then progress to a monthly
update or reactively as required.
• For the next update the group wil focus on any potential changes in recommendation for
the use of budesonide. Pharmac has indicated there is capacity to supply a sustained
increase.
Official
• It was suggested that it would be useful to have some signal ing around the use and
availability of baricitinib, in preparation for any potential changes.
the
• As noted in previous minutes, there has been suggestions to incorporate pregnancy into
the guideline. A member suggested that there are several options in how this could work
which would be circulated to the group.
ACTION: Chris Hopkins to circulate options for incorporating pregnancy into the Interim Guidance -
Clinical Management of COVID-19 in Adults.
under
• There are several obstetric physician colleagues who may be interested and available to
contribute to the guidelines working subgroup. STA noted that bringing members on as
part of the working group (but outside the Therapeutic TAG membership) could be
facilitated.
ACTION: Chair to contact obstetric physician col eagues regarding contribution to the guidelines
working group.
• The group discussed membership general y and noted that there may be a requirement for
Released other involvement as the COVID-19 situation changes.
• The Chair noted that there had been some discussion of documenting the decision making
involved in developing the guidelines.
Document Three
ACTION: Anne Buckley to talk to Tim Cutfield regarding documenting guideline group decision
making.
Patient information update
• There is a scoping discussion on 08 October 2021 to form a subgroup with the Health
Navigator team and those who have been working on resources that are being used in
hospitals.
• The aim is to put forward a proposal to set aside budget for this patient information update
work so it can progress. The team have recently done similar work for a new therapy, so
they have already thought through some of the likely challenges.
• The group noted that this would be a very useful and widely used document once
complete.
1982
5.0
Equity Considerations
Pasifika representative-led discussion
Act
• A member raised an issue for consideration when exploring the use of budesonide. It was
suggested that the age cut-offs in the Australian Living Guideline may not be appropriate
for the Aotearoa New Zealand context. Using these age cut-offs could create an equity
barrier for Māori and Pacific peoples, who may develop disease earlier.
• There was discussion about the use of ‘over 50 with comorbidities’ criteria and if that
would help in this situation, However the group agreed that it would be beneficial to
recognise earlier onset of comorbid disease by adjusting both of the age criteria from
PRINCIPLE to be reduced by 10 years for Māori and Pacific patients. (40 vs 50 years with
Information
comorbidities and 55 vs 65yrs without).
• The group acknowledged that this adjustment would be stepping outside of the trial
evidence but noted that the risk of introducing hazard was low, and the change seemed
beneficial based on clinical experience. If a change was operationalised, ongoing
surveil ance of outcomes would be helpful. A member noted that this would align with what
Auckland MIQ group decided to do, with similar reasoning as above.
Official
ACTION: Guideline working group to consider these suggestions of more equitable age criteria
the
when exploring the use of budesonide.
• The Chair suggested the group should write to Māori and Pacific health care providers to
give more information about what the TAG is doing. Members agreed this would facilitate
further feedback and important aspects to consider. It was suggested to also include Māori
and Pacific Pharmacy Associations, and Te Rōpū Whakakaupapa Urutā.
under
ACTION: Saleimoa Sami and Jessica Keepa to draft a letter to be distributed to Māori and Pacific
health care providers from the group.
6.0
Therapeutics: Clinical Trials Including in Primary Care/Community
• No update given.
• The group had general discussion about reducing stigma of receiving a positive COVID-19
test and the important role that Primary Care wil continue to have in the future.
Released
7.0
Next Steps/Other Matters
• A member noted that they wil report back to the group regarding the Australasian COVID-
19 Trial (ASCOT).

1982
Act
Information
Official
the
under
Released
Document Three
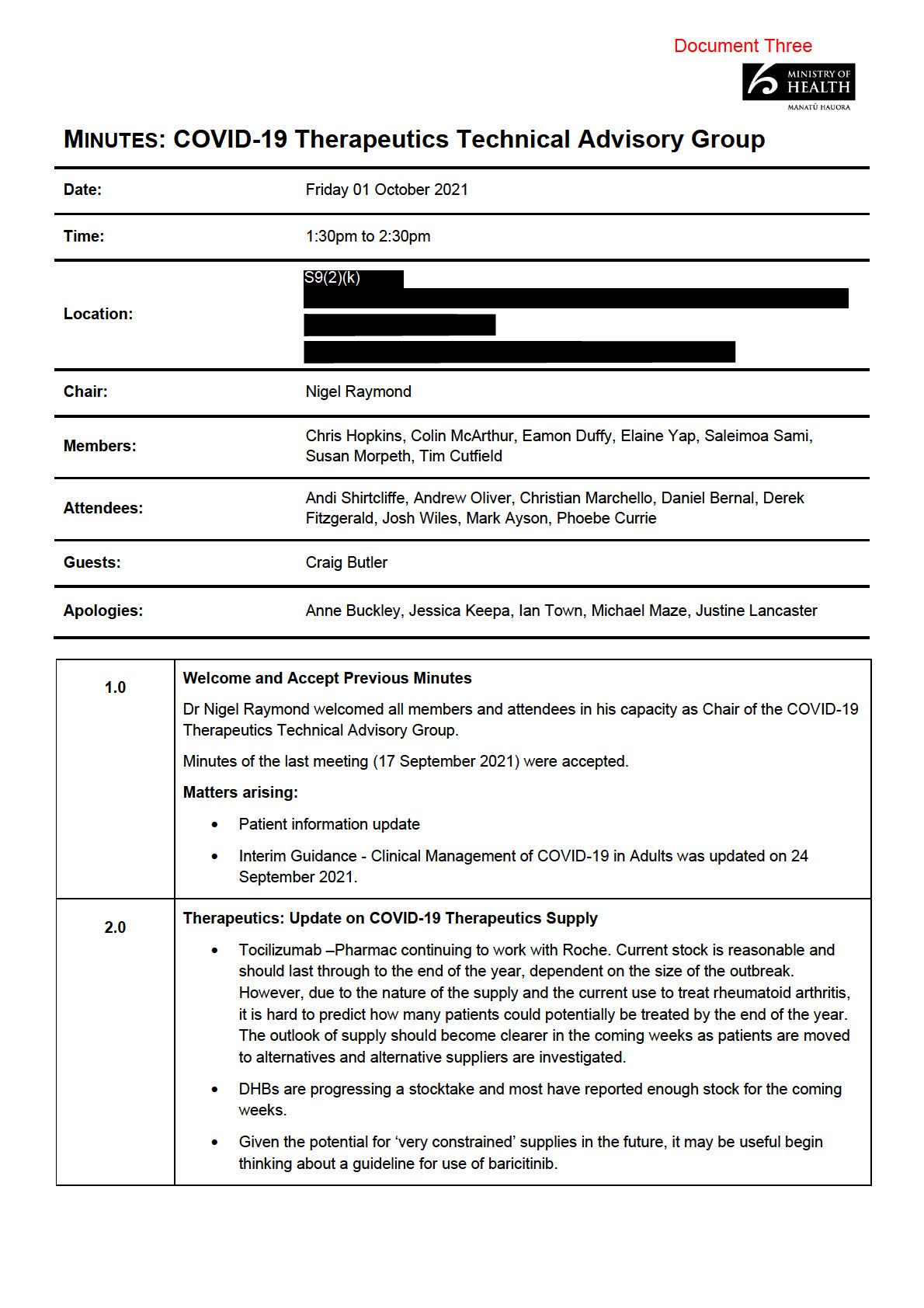
Review update and publish
17/09 – Action raised
5 Guideline update
Tim Cutfield/STA
revised guideline
01/10 - Next update 8/10/21
17/09 – Action raised
Therapeutics:
Preliminary testing of
6
STA
01/10 – STA review
prioritisation criteria
prioritisation criteria
feedback, consider further
draft.
Therapeutics: Update
Group to consider the
7 on COVID-19
development of guidance for All
01/10 – Action raised
Therapeutics Supply
the use of baricitinib.
1982
Chris Hopkins to circulate
options for incorporating
Guideline
Act
pregnancy into the Interim
8 Update/Patient
Chris Hopkins
01/10 – Action raised
Guidance - Clinical
information update
Management of COVID-19 in
Adults.
Chair to contact obstetric
Guideline
physician colleagues
9 Update/Patient
Chair
01/10 – Action raised
regarding contribution to the
information update
guidelines working group.
Information
Anne Buckley to talk to Tim
Guideline
Cutfield regarding
10 Update/Patient
Anne Buckley
01/10 – Action raised
documenting guideline group
information update
decision making.
Guideline working group to
consider these suggestions
Official
Guideline working
11 Equity Considerations of more equitable age criteria
01/10 – Action raised
group
when exploring the use of
budesonide.
the
Saleimoa Sami and Jessica
Keepa to draft a letter to be
Saleimoa Sami and
12 Equity Considerations distributed to Māori and
01/10 – Action raised
Jessica Keepa
Pacific health care providers
under
from the group.
Released