1982
Act
Information
Official
the
under
Released
Document 1
o The next Testing Strategy wil be submitted to the group by Tuesday 16 November
• A survey is underway to get a community perspective with a major focus on equity. This wil inform
what follows the strategy after 22 November.
o Action: The chair requested this survey to be shared with the group for their awareness
Chair opened the floor for discussion.
• A member noted that feedback had been captured in the new version of the strategy
• A member noted that the situation in Auckland is critical; the laboratories are beyond capacity and
need some level of prioritisation before adding more categories that will increase testing demand.
o A member noted a key function of the strategy should be to offer flexibility and enable
prioritisation.
o A member noted the 22 November ministerial deadline didn’t feel soon enough, in relation
to prioritisation and reduction in non-essential testing particularly for the Auckland region.
o It was noted by MOH that a meeting with NHRCC discussed immediate priorities for
testing strategy. There have been some approvals made.
1982
o The MOH noted that a meeting is being organised with NHRCC to discuss supply and
demand options.
Act
o Action: The chair requested that these recommendations are shared with the group for
their awareness.
• A member questioned traveller, MIQ, and education setting testing, and the extra demand this wil
place on testing and what was being planned in these areas.
o There is work being done in the border workers group.
• A member asked if there were any updates regarding incorporating prioritisation into eOrders.
o It was noted the team had IT capacity to do this.
o A member noted Sysmex had been working on doing this, but progress has been slow.
Information
o Members agreed finding a functional way of doing this was a priority.
o Action: A member requested an update and a timeline for e-ordering.
Actions:
• Feedback on testing strategy wil provided to MoH after a meeting of Testing TAG on 16th Nov
Official
4.0
Evaluation Framework
the
• It was noted that this was similar to the previous version. The main part addressed was item 13
(selection criteria) and how additional criteria would fit in.
• A member noted that the evaluation group previously used (ESR) was not the appropriate one to
use.
under
o It was clarified that ESR are coordinating but not conducting.
o A member noted involving two entities may cause delays.
• A member stated they were unsure from the framework what the trigger point was for further
evaluation of the POC test.
o It was agreed this was subjective.
o An explanation was given that it would be done by STA as they went through the criteria.
Released
o A member asked if a laboratory person would be involved in this.
o MOH advised that a laboratory background wasn’t required to make these decisions, just
a clear set of criteria for someone with a health science background to use.
• A member was concerned about flooding the NZ market with hundreds of different tests, which
would cause confusion among the public. The member recommended a high threshold for
approving a test.
• A member noted the storage requirements for these tests could be an important inclusion criterion
– whether the manufacturer can store these or not. Hospital storage is running low.
• For 13b (integrating reporting infrastructure) a member noted this was incorrect because these
were not laboratory-based tests.
Document 1
o It was noted that there are two different measures combined into one point: does the test
comply with NZ standards and can the provider or user integrate this into reporting
system.
• A member noted one criteria that should be included is deliverability (i.e. supply of the kit), which
didn’t appear to be on the criteria.
o Adding this would eliminate some of the kits out of the 100 that need evaluation.
• It was noted that there wil be questions on why/why not we are including some RATs and not
others.
• A member addressed item 3 (authorisation to import, supply and/or use 3 RATs) as being too
broad:
o It was explained this was a public health order.
• The member asked whether laboratories could order kits from MOH on a continuous basis or does
this need to be publicly funded.
o It was agreed the supply and distribution for labs needs to be discussed through the
National Network meetings or directly with the MOH testing team.
• It was noted that sensitivity depends on who the kit is evaluated on (if they’re symptomatic, or if
1982
they just want to go to a large social gathering).
o A member agreed and suggested the wording in 10a should be clarified to say the specific
Act
population being tested or context for appropriate utilisation.
o It was noted that this was taken from the WHO EDCE.
o A member suggested that a comment be made about interpreting the context of sensitivity
and specificity in NZ.
o It was noted the urgency to commence evaluation of the large number of submissions to
import devices.
Information
The chair asked if the group supported this framework
o The group agreed to endorse this framework, noting the additional comments from the CT
TAG and
o Action: MOH to provide some examples to the CT TAG of how they evaluate the first few
Official
devices and recommend context for use.
5.0
Ministry of Health Position Statements
the
5.1 Position on saliva as a diagnostic sample
• MoH explained that saliva could not currently be used by ESR for WGS, so the wording in the
position statement was updated to reflect this.
under
• A member noted they believed the diagnostic and operational capacity and turn around times of
saliva testing are two different things.
o This is not necessarily obvious to the public at large.
• In MIQ, daily testing has started with a push to encourage workers to take up saliva testing.
• The group agreed to accept the saliva paper, with a caveat that we don’t have capacity to use it to
the same extent as nasopharyngeal swabs for RT-PCR.
Released
5.2 Position on use of rapid antigen testing and programme rol -out
• A member asked whether there was a plan for implementation by businesses, such as a checklist.
o A member noted there should be a normal POCT implementation process for community
roll-out i.e., process, framework, requirements, operations.
• A member noted labs require RATs for contingency planning. There have been conflicting
statements about which RATs can be ordered.
• A member asked if this TAG is implementing RATs for the community and businesses.
o It was noted that this would managed by the MoH Testing and Supply team
• A member noted equity didn’t seem to be demonstrated in the roll-out.
1982
Act
Information
Official
the
under
Released

1982
Act
Information
Official
the
under
Released
Document 2
o MoH: that standing capacity came from 2% positivity rate which required a 60k standing
capacity. It also takes into account the available capacity across the network – technical
capability that would be available.
o The group encourages further engagement with national laboratory group around
assumptions.
ACTION: MoH to continue engagement with national network and let them know what’s going on. If there’s
an action on this, MoH wil report back to CT TAG to ensure that it’s done.
• A member asked whether there were timelines in place for the strategy to be updated, given that it
was described as a living document.
o MoH: a regular cycle of review is anticipated that is consistent with other engagements,
particularly to incorporate innovative technologies. The surveil ance strategy sits above
the testing strategy. The review is set for March, with an interim review before then to
ensure the framework is appropriate for pre- and post-Christmas.
o A member advocated for a review before March 2022.
1982
• A member asked whether there is an organisational design of strategies and plans, noting who is
responsible / inputting into the work. This could be especially helpful to col ectively outline what the
strategies are, how they relate to each other, and what the timelines are on each.
Act
ACTION: create a standing item in the agenda for CT TAG to identify any changes and input that may be
required for the testing strategy.
3.0
Prioritisation via IT upgrades
• MoH: A line is being built into the LIZ registration screen that wil give the ability to prioritise some
tests.
• Clinical advisors and lab IT team were consulted to develop these criteria.
Information Factors to determine
priority are the surv codes, are they close contact, are they in an isolating household, have had
positive test in last 3 months?
• Working with operational groups on the ground to address these tests for visual / physical cue i.e.,
stickers. However, ethnicity or other socio-demographic factors aren’t currently reported in the
Official
priority criteria. Working with Kirk to ensure equitable outcomes in product design, but ultimately
this will help with the prioritization. Wil incorporate this on Friday and wil go live first as a pilot with
Waitemata and counties Manukau
the
o A member asked why ethnicity is not included in prioritisation, highlighting its importance
in ensuring an equitable approach.
o MoH: E-swab ordering cannot incorporate ethnicity easily. Incorporating it into the e-
ordering is technic
under ally very difficult at present and would result in a considerable delay to
the rol -out of the revised e-ordering. Another option is to copy ethnicity information from a
person’s NHI. Incorporating ethnicity into the e-ordering form will be in the next phase of
prioritisation development and wil take approximately 4-6 weeks.
o A member urged this to be done urgently rather than waiting for the next phase since
there is no equity lens if these groups are not prioritised.
o A member countered that any priority system wil improve equity, even without ethnicity
Released
data, since the only way laboratories can prioritise currently is to manually prioritise
hospital testing and that of close or household contacts. Community testing is not
prioritised; many tests in this group are non-urgent, but they also include tests from Māori
and Pacific people who are symptomatic. Prioritising symptomatic testing wil also improve
equity.
• A member urged the Ministry to use NHI for ethnicity as this is generally more accurate than other
processes.
• A member asked whether this prioritisation plan wil be national
Document 2
o Prioritization system wil ultimately be national. Most community testing centres and popup
testing centres are on the e-ordering system. However, not all GPs are on the system.
There are constraints with labs not using Delphic but working with them.
• The Chair invites Erika Kuhn to feedback in future meetings and provide an overview of how
they’re addressing equity gaps nationally.
4.0
Equity (introduction of new point of contact at MOH and community engagement)
• Kirk Mariner was introduced as the new point of contact
• MoH: the aim is ensuring engagement and that a voice is coming through to the present equity
lens. There are pockets within testing supply that address and implement equity well, and it’s
important to ensure to the COVID-19 directorate is linked up across the system to ensure equity
as well.
o A concern is that sometimes things are done so fast that equity is not possible.
o Currently working on setting up engagement process for Māori, Pasifika, disability, and
other priority populations so that they can be both key contributors and designers of the
1982
solutions.
5.0
Operationalising selection criteria
Act
• MoH: There is a specific item in Criteria #2 on test sensitivity that would be quite a limiting factor
for selecting appropriate tests. Further, it’s unlikely that independent clinical studies wil meet that
threshold. Most manufacturers are claiming sensitivity of 95%+ but in the real world, sensitivity is
unlikely to be that high. There is a concern that the three kits already approved would not meet
these criteria.
o The Group suggested to re-word the criteria. Devices should have to meet the
sensitivity/specificity thresholds following WHO guidelines. There need to be independent
validation studies measuring sensitivity and specificity in addition to the manufacturers’
Information
claims. The Group raised the concern that if we don’t include the WHO guidelines in the
selection criteria, the NZ market wil be flooded with too many RATs.
• Note that the criteria outlines selection criteria for point of care tests (POCTs), as not al point of
care tests are RATs. There were over 200 applications, which have been screened. The majority
were RATs but there were also some antibody and rapid PCR tests.
Official
• A member noted that we urgently need point-of-care style rapid tests available, because of
shortage of GeneXpert. The STA wil begin reviewing rapid molecular tests.
the
ACTION: MoH Testing Operations to share the RAT roll out plan with CT-TAG
5.1
Horizon scanning/innovation intel report
• MoH: The Science and Technical Advisory team will be meeting fortnightly with a consultancy. The
under
first meeting has just taken place but did not explore testing modalities in detail.
• This is the first report that the consultancy has completed. They can conduct ad hoc requests
aside from the fortnightly presentations and could look into rapid PCR tests at our request.
• These reports wil be released regularly and won’t be included in the agenda but sent out as the
Group wants. Note that the terms of the contractual arrangement with the consultancy means that
while the information can be shared with the Testing TAG, it cannot be disseminated more widely.
• A member asked why the US and UK were chosen as countries in the report.
Released
o MoH: these countries were chosen because they had extensive RAT strategies. For the
next report, we have asked to see countries with similar strategies to NZ next e.g.,
Australia, Singapore, Taiwan. We would like more feedback on innovation on two tiers:
one focussed on the future and another focussed on places that are especial y innovative.
o Member: There are two ways of being innovative: innovative tests and then innovative
strategies.
• In a higher prevalence environment, a PCR test may not be required following a positive result on
a RAT.
• A member asked what is meant by “decent” prevalence? What is that benchmark?
1982
Act
Information
Official
the
under
Released
Document 2
1982
Act
Information
Official
the
under
Released

1982
Act
Information
Official
the
under
Released
Document 3
Matters arising:
• There were no matters arising.
Therapeutics
2.0
Pharmac Update
• COVID-19 Treatments Advisory Group meeting record from October has been published and is
available on the Pharmac website. The meeting record for the December meeting is being
finalised. The group is considering access criteria for a number of treatments.
• Consultation on the Pharmac proposal on access criteria for two COVID-19 treatments (baricitinib
and casirivimab/imdevimab) closed on Wednesday 12 January 2022. Pharmac is now working
through feedback; themes so far include ensuring equity of access, other groups that might
1982
benefit, requirements for serology testing.
• Pharmac has secured more stock of baricitinib and remdesivir which is currently in transit to
Act
Aotearoa New Zealand.
• Pharmac is aware that oral antivirals (molnupiravir and Paxlovid) are anticipated and wil release
consultation on access criteria for these as wel , aiming to provide as much time as possible for
preparation as to how these might be administered.
Tocilizumab
• Pharmac has purchased a one-off supply of subcutaneous tocilizumab, which has been distributed
Information
to 9 DHBs across the country, alongside guidance on administration. Subcutaneous tocilizumab
does not have regulatory approval. DHBs are able to decide how to use the medicine. Funding is
in line with IV tocilizumab.
• Pharmac released some IV tocilizumab stock to DHBs prior to Christmas, is working on resupply
and continues to monitor usage. Official
Discussion
the
• A member asked about the estimated time of arrival for molnupiravir and Paxlovid. Pharmac noted
that they need to go through the Medsafe approval process. Current expectations are that they
may arrive in New Zealand in the coming months.
• A member raised a question about potential supply of sotrovimab. Pharmac advised they are
under
aware of increasing global demand and hope to achieve progress with GSK about NZ supply early
this year.
Medsafe Update
• Medsafe facilitates applications and application pathways. Medsafe is reliant on companies
Released
making applications and responding to information requests to progress the approval process.
• Molnupiravir – Merck have not submitted an application to Medsafe for molnupiravir. Medsafe are
expecting to receive an application in February. US FDA have given molnupiravir an emergency
use authorization (EUA).
• Casirivimab/imdevimab (Ronapreve) was approved by Medsafe in December 2021- the first of the
completely new medicines to be approved for treatment of COVID-19 in Aotearoa New Zealand.
• Paxlovid – Medsafe is assessing information provided by Pfizer in response to questions. Pfizer is
releasing ongoing clinical information. US FDA have given Paxlovid an EUA.
Document 3
• Remdesivir – Medsafe have almost finished the initial evaluation process.
Discussion
• Baricitinib: A member raised a question about the status of baricitinib. It was noted that baricitinib
is not approved and no application from Eli Lily has been received by Medsafe. Pharmac noted
that their understanding is that Eli Lily do not intend to make an application to Medsafe for
approval. Supply was at Pharmac’s request as an alternative to tocilizumab.
• A member raised a question regarding the use of baricitinib. It was noted that currently it can be
used under exceptional circumstances, and (pending access criteria) from 01 February 2022 it can
be used via the standard section 29 processes.
• A member raised a question regarding the Roche application for Ronapreve and dosing in
hospitalised adults. Medsafe have approved what Roche applied for in the original application.
Airfinity/STA Update
1982
• As requested previously, STA provided a summary of key reporting from Airfinity (7 January 2022)
on therapeutics as well as an excerpt taken from a more comprehensive document ‘Science and
Act
Technical Advisory Omicron Update, 11 January 2022’. Key content from the updates included:
o US NIH changes to their guidance which included Paxlovid being the preferred outpatient
treatment.
o Several neutralisation studies showing Omicron resistance to Ronapreve.
• A member raised a question regarding the definition of disease severity used in data reported in
the Airfinity summary (slide: Overview of current approved COVID-19 treatment candidates and
Information
their status in the UK, EU & US). STA wil provide clarification following review.
Equity Considerations
3.0
• A member noted that equity feedback on Ronapreve has already been provided but emphasised
that the idea of a therapeutics/administration centre as a general concept could be beneficial and it
Official
is likely that colleagues in Pacific health would be involved.
• A member raised a question regar
the ding the supply of remdesivir and whether it would be made
available in the community, as the initial criteria was around hospital use. It was noted that
National Institutes of Health (NIH) have recommended that remdesivir could be used as a
treatment for non-hospitalised patients with COVID-19 who are at high risk of progressing to
severe disease. Pharmac n
under oted that the Special Authority criteria for remdesivir has yet to be
finalised.
Guideline Update
4.0
• The next planned update is 21 January 2022. The group met during the week and discussed a
number of issues. Significant changes are not expected for the coming update. The draft 21
January update is currently being reviewed by the group.
Released
• Casirivimab + imdevimab (Ronapreve) - not included in the 21 January update as Pharmac access
criteria yet to be finalised. Noted that the group provided a submission to the Pharmac
consultation on baricitinib and Ronapreve which closed 12 January 2022. See 5.0 for further
discussion on the submission.
• Remdesivir - The group noted the PINETREE study definition of high risk is similar but different to
studies for access to monoclonals. The group agreed that it is sensible to align a common
definition of high risk, to simplify for the practitioner. Further discussion may be needed on this for
future guideline updates.
Document 3
• The group noted that the guideline’s definitions of mild, moderate and severe disease are slightly
different to those used in some other guidelines. Noting as a group – no changes deemed
necessary at this point.
Tocilizumab
• There was discussion about subcutaneous tocilizumab. It was noted that for COVID-19 treatment,
IV tocilizumab was preferred and that converting subcutaneous tocilizumab for IV use is practically
challenging and there is potential for error resulting in dose reduction. It was noted that the
company have provided guidance on this process, but it was suggested by a member that the
technical aspects prohibited its ready use in busy clinical environments.
• Some members expressed the view that the clinical priority for use would be IV tocilizumab as
preferred treatment, with baricitinib as an alternative. It was noted that this is the preference the
group have signal ed previously in meeting discussions. Subcutaneous tocilizumab was suggested
for treatment of acute or critical covid and reserved for when neither IV or baricitinib are available
1982
and suitable for use (e.g., a person has contraindications for use of baricitinib).
• A member suggested that it would be helpful to have further information on the stability of
Act
tocilizumab after conversion from subcutaneous to IV. Information on stability (how long the
treatment is viable for) could inform other suggestions, such as possible use of a centralised
centre/s completing the conversion required which could decrease pressure on clinical staff and
the likelihood of errors.
Pharmac Consultation Feedback
5.0
• The group submitted feedback to the Pharmac consultation proposal on access criteria for two
Information
COVID-19 treatments (baricitinib and casirivimab/imdevimab).
• The baricitinib section of the submission largely noted that the eligibility criteria are mostly similar
to the current guideline, the only difference being that the submission recommendation does not
require raised inflammatory markers.
Official
• It was noted that the baricitinib access criteria for Pharmac matched tocilizumab criteria; and that
there is a discrepancy regarding eligibility for tocilizumab between the criteria and the
the
recommendations in the guidelines from this group. This will be reviewed once the access criteria
are finalised.
• The casirivimab/imdevimab (Ronapreve) section of the submission outlines several competing
treatment tensions including:
under
o the lifespan of usefulness is potential y limited due to the likelihood of an Omicron
outbreak and the evidence suggesting Ronapreve does not neutralise Omicron.
o there could be positive impacts for a large number of people in the community who could
be eligible, however, the opportunity costs are large (e.g., redirecting limited health
resources).
Released
o demands on serology also produce a competing priority for laboratories processing PCR
tests to monitor the pandemic.
Discussion/Feedback
• The group noted that the likelihood of an Omicron outbreak adds complexity to the treatment
situation and that it would be helpful to have a timeframe for when treatments are expected to
arrive.
Ronapreve
Document 3
• From an equity perspective it was noted that the timeline for an Omicron outbreak is unknown,
however the Delta outbreak is continuing and using Ronapreve now could be beneficial. Māori and
Pacific people have high case numbers of COVID-19, on top of the burden of comorbidities and
deprivation. Any support that can be provided would be positive, however it is understood that
there are logistical challenges.
• Feedback was provided by a member from some Pacific medical practitioners in Auckland who
commented that among the Pacific community there is a high double vaccination rate (with the
caveat of immunocompromised and those who have not produced a good immune response). It
was felt that establishment and resourcing of Ronapreve clinics in the community could be very
challenging and not as beneficial once Omicron is in the community.
• It was noted that:
o There is work underway within the Ministry in relation to community use of therapeutics
and further coordination and communication is expected in the coming weeks.
o Demand for quick WGS to enable administration of Ronapreve in a timely manner also
1982
presents an equity issue due to processing times.
o Setting up clinics and using Ronapreve now would be an opportunity to benefit patients
Act
and could also provide the logistical framework for administering other treatments in the
future.
o Ronapreve could be used in hospital quite quickly, however if there is not a system for an
equivalent use in the community, this could present a dilemma for clinicians, with hospital
admission needed for patient access to the treatment.
o Once the final access criteria are released, further work may be needed to determine who
should get the medicine and how. The group felt that the Therapeutics TAG could
Information
contribute to this discussion, but others, including primary care and rural hospitals are
essential to the discussion/planning.
Timeline for Oral Antivirals – Community
6.0
Official
o It was noted that there is increasing global demand for Paxlovid and that the current timeline
estimated by Pharmac for arrival in Aotearoa New Zealand is April 2022.
the
Next Steps/Decisions Pending
7.0
• Guideline update planned for 21 January 2022.
under
Any Other Business
8.0
• An attendee suggested that improved connections with the Ministry COVID Care in the
Community team could assist their planning, particularly detailed discussion of when therapeutics
might be expected.
• A member noted that therapeutics and testing strategies need to be considered together, given
efficacy is greatest when treatments are given early. Also, that testing strategies may change
Released
during the anticipated Omicron outbreak with greater use of rapid antigen tests rather than PCR
confirmation.
Agenda Items for Next Meeting
9.0
COVID Care in the Community team update
New Action Items Raised During Meeting
10.0 STA to provide clarification on Airfinity slide data with respect to source of definitions of severity.

1982
Act
Information
Official
the
under
Released

1982
Act
Information
Official
the
under
Released

Document 4
COVID-19 Therapeutics Technical Advisory Group
MINUTES: Te Rōpū Haumanu Kowheori-19 Date:
Friday 10 December 2021
Time:
1:30pm to 2:30pm
S9(2)(k)
Location:
1982
Chair:
Nigel Raymond
Act
Members:
Chris Hopkins, Colin McArthur, Eamon Duffy, Elaine Yap, Jessica Keepa, Michael Maze,
Susan Morpeth, Tim Cutfield
Attendees:
Andi Shirtcliffe, Andrew Oliver, Anne Buckley, Daniel Bernal, Derek Fitzgerald, Justine
Lancaster, Josh Wiles, Ian Town, Mark Ayson, Phoebe Currie
Guests:
Therese Egan; Rachel Webb
Information
Apologies:
Saleimoa Sami, Adrienne Martin
1.0
Welcome and Accept Previous Minutes
Dr Nigel Raymond welcomed al members and at
Official tendees in his capacity as Chair of the COVID-19
Therapeutics Technical Advisory Group.
Minutes of the last meeting (26 Nov
the ember 2021) were accepted.
Matters arising:
• There were no matters arising.
under
The Chair thanked the group for their work during the year and noted their important contribution to
the COVID-19 Response, including the ongoing work on the guideline Clinical Management of
COVID-19 in Hospitalised Adults.
2.0
Therapeutics
Pharmac Update
Released
• The Pharmac COVID-19 Treatments Advisory Group is meeting on 13 December with
discussion planned on eligibility criteria for Ronapreve, other monoclonal antibodies from
AstraZeneca and Celltrion, Pfizer’s oral antiviral and remdesivir.
• Baricitinib has been distributed to DHBs and ongoing supply is being progressed.
• Additional supply of remdesivir is to be secured to meet potential need if access criteria
changes.
• Ronapreve – following initial supply early 2022, an additional supply is expected mid-year
of a further 7,500 doses.
Document 4
• Pharmac is in ongoing discussions with various suppliers. Pharmac has negotiated an
agreement for 60,000 courses of Pfizer’s new oral antiviral protease-inhibitor treatment
Paxlovid (nirmatrelvir+ritonavir).
Medsafe Update
• Medsafe provided an update on approval processes following receipt of an application
from a drug company.
• Ronapreve – Medsafe is currently assessing additional information the company has
provided on request from Medsafe.
• Paxlovid – Medsafe has received an application from the company and an initial
assessment has been completed. Additional information has been requested from the
company.
• Remdesivir is under assessment by Medsafe.
• Molnupiravir - Medsafe has not yet received an application from the manufacturer.
1982
Airfinity/STA Update
Act
• STA provided a summary of key reporting from Airfinity (3 December) on therapeutics,
including content on molnupiravir, a list of recent papers, and the impact of Omicron and
therapeutics. Feedback within the meeting was that both the content selection and length
were appropriate for ongoing regular updates via the meeting from STA.
• STA reported that there was a media briefing today (10 December) regarding therapeutics
including mention of the Therapeutics TAG. The briefing was led by Ashley Bloomfield
Information
(DG, Ministry), Ian Town (Chief Science Advisor, Ministry) and Sarah Fitt (CEO Pharmac).
The briefing can be found here.
3.0
Equity considerations
• A document ‘Wai 2477 Te Ora case’ was c
Official irculated with the agenda for discussion. A
member gave an update regarding this document and outlined key equity issues for
discussion.
the
The document has key statements about the Māori population in NZ that the NZ Māori Council
identify as important:
• [Māori]
are a younger, more mobile and socially active community with high essential
under
worker status that dictate that we wil be more likely to be in contact with COVID 19
• [Māori]
are an undervaccinated population and therefore more likely to be infected
when exposed and to get sick
• [Māori]
have an ‘older population who are more unwel ’ and therefore more likely to get
very ill and/or die
Released
• [Māori]
have a population who are generally more marginalised from various aspects
of care and therefore harder to diagnose, contact trace and treat”
• It was noted that it is important to link these considerations to the mahi the Therapeutics
TAG is doing, particularly what can be done to ensure that Māori have equitable access to
therapeutics in the community.
• Equity issues such as those mentioned above should be considered when developing
eligibility criteria for therapeutics and model ing to support delivery of therapeutics.
• It is important to have good information available about any therapeutics that are to be
used in the community. For example, it would be beneficial to give information to Māori
Document 4
providers to disseminate, wananga or socialise, to increase understanding of what
treatments are available and the reasons for engaging with treatment provision.
Discussion
• A member raised the importance of testing and case identification, given the short period
post-onset in which many therapeutics offer effective treatment. The group agreed this
was an integral equity consideration.
• A member noted that a positive COVID-19 diagnosis in NZ currently carries a lot of stigma
and that the group may have a role in reducing this stigma. Another member suggested
that a video of whanau with ‘lived experience’ of COVID-19 could be a useful tool to
reduce stigma.
• The issue of potential treatment hesitancy in NZ was raised. Recent research in the USA
included in the Airfinity summary information provided by STA showed that treatment
hesitancy and vaccine hesitancy were not linked there. The group discussed the need to
provide information for people who may be uncertain about treatments and require more
1982
certainty before engaging.
• The group agreed it is important to increase health literacy about COVID-19, particularly
Act
when new treatments become available in the community.
• It was noted that the Ministry is progressing work on misinformation and disinformation
relating to vaccines which could be built on. The group agreed that misinformation about
treatments could be a topic for discussion in the future.
The Chair noted that it is important the group incorporates learnings from the vaccine programme
and Waitangi Tribunal case into the Therapeutics TAG work.
Information
4.0
Guideline Update
• An update of the guideline was published on 3 December 2021 and is available here.
• The update included a change to the layout of the immunomodulatory therapeutics section
for moderate COVID-19 to indicate the pr
Official eference for tocilizumab.
• Preparation of content on Ronapreve for inclusion wil be addressed once eligibility criteria
the
are finalised by Pharmac.
• The next planned update is 21 January 2022.
5.0
Paediatric Update
under
A paediatric update was provided, including Starship experience of the current Delta outbreak in
Auckland.
• The Starship paediatric guideline
Covid-19 Disease in Children is found here
It continues to be monitored and updated. There is close liaison with colleagues in Sydney
and at the Royal Childrens’ Hospital in Melbourne, both centres having more COVID-19
Released
cases in children than seen in NZ to date. The guidelines include content on
dexamethasone, remdesivir, tocilizumab, as well as a statement noting that there is no
evidence to support the use of inhaled budesonide for community management of
COVID-19 in children.
• The Royal Childrens’ Hospital in Melbourne has developed a treatment pathway which
includes sotrovimab & also management of Paediatric Inflammatory Multisystem
Syndrome (PIMS).
Discussion

1982
Act
Information
Official
the
under
Released

1982
Act
Information
Official
the
under
Released

1982
Act
Information
Official
the
under
Released
Document 5
There was an initial discussion about the draft criteria, including hospitalised patients and
a specific group of community patients, but it was noted that this was confidential until the
records are published.
There wil an opportunity for wider consultation on the criteria. This consultation typically
identifies broader issues and practical matters eg. relating to delivery or serology testing,
to be considered prior to the funding decision being made.
Discussion
•
Members noted that if criteria include a requirement for serology testing in hospital patients
this would increase pressure on the laboratory system.
•
Serology turnaround times are variable around the country. Provincial hospitals access to
serology testing and turnaround times vary markedly compared to large metro hospitals
and a member suggested this needs to be taken into account in the criteria.
•
Members noted that there needs to be a clear definition for immunosuppression/’severely
immunocompromised’. An example is the criteria used to define immunosuppression for
those recruited into the REMAP-CAP trial.
Medsafe Update
•
Three products are under assessment – Ronapreve, remdesivir, Paxlovid.
•
Applications for molnupiravir and Evusheld have not been received yet.
Airfinity/STA Update
•
STA provided an update on the Airfinity therapeutic surveil ance information.
•
Airfinity provide fortnightly updates to STA on therapeutics in response to parameters set
by STA as wel as information on any specific questions asked.
•
STA can also summarise primary research for specific agents or request this information
from Airfinity
•
The group noted that the amount of information is significant. A summary or indication of
important points/new developments would be useful.
ACTION: STA to provide key points of the Airfinity therapeutics surveil ance information to
Therapeutics TAG meetings.
under the Official Information Act 1982
3.0
Equity considerations
•
An update on the CAG group was requested – this is working on models of care for the
community. Several people from within that group have expressed a wil ingness to liaise
with Therapeutics TAG regarding practical considerations and primary care therapeutic
management as needed.
Released
•
The Therapeutics TAG noted the importance of having the infrastructure in place in the
community to deliver treatments equitably, for Ronapreve or for other treatments going
forward.
•
Eligibility criteria for medicines, including Ronapreve, need to be considered from an equity
perspective. As noted in earlier discussion on Ronapreve, there are equity considerations
regarding the geographic differences in serology testing turnaround time.
•
The Pacific Pharmacist group have provided feedback in response to engagement from
the Therapeutics TAG via our Pacific representative.
Document 5
o The group have reviewed the current Guideline and had no specific concerns or
ideas but indicated they wil have more to contribute as more treatments become
available in the community.
o General comments shared from the group included that better communication with
community clinical pharmacists is required regarding notification of COVID-19
cases and dispensing of their medications. There is currently no standardised
process notifying patients’ pharmacist of a positive case.
• It was noted that the Ministry is actively working on the Pharmacy primary care clinical
model – mentioned in the meeting of 12 November with a draft document circulated to the
group.
ACTION – STA to circulate summary feedback from Pacific Pharmacist Group to Ministry
(Pharmacy team).
4.0
Guideline Update
1982
• Latest Guideline Update was published on 22 November 2021 and included guidance on
baricitinib use. Available here.
Act
• The Guideline subgroup were thanked for their ongoing input. It was acknowledged that
the work of international guidelines in reviewing evidence greatly assisted the process of
rapid updating. Of note - newer agents could potentially be available for use in NZ before
they are included in international guidelines.
• Next planned update is 03 December 2021
To be included:
Information
o Note that use of baricitinib is under Section 29
o Clarification points noted from subgroup feedback re. anticoagulation
Hospital use of Ronapreve – for inclusion in a future update
Official
• This wil be included in a coming guideline update to coincide with supply expected. Not
planned for this update as supply not expected now before January.
the
Serology testing
under
An update on serology testing
was included in this section as it has relevance to potential hospital
use of Ronapreve.
• The document ‘CoV2 serology TAT summary for Therapeutics TAG from NZMN’ was
circulated with the agenda to inform discussion.
• The document provides an update on the availability and turnaround time of SARS CoV-2
serology testing around NZ, current as at 15 November 2021.
Released
• The information was shared with the Therapeutics TAG by Dr Susan Morpeth, Chair of the
NZ Microbiology Network (NZMN) and member of the group.
• There are some parts of the country that are likely to have slow (inadequate) turnaround
times for serology testing if required prior to initiating Ronapreve treatment.
• Some labs have indicated they could expand their serology testing service, however a
signal of the number of tests required would be needed for that to be considered.
• Upscaling serology testing would put additional capacity pressure on the same labs and
lab staff who are already increasing PCR testing capacity.
1982
Act
Information
Official
the
under
Released
Document 5
Therapeutics TAG via
scheduled meetings.
STA to circulate summary
feedback from Pacific
17 Equity Considerations
STA
26/11 – Action raised
Pharmacist Group to Ministry
(Pharmacy team).
1982
Act
Information
Official
the
under
Released

1982
Act
Information
Official
the
under
Released
Document 6
• Tocilizumab - closely monitoring stock with Roche and expecting January resupply.
Working to get additional stock, either IV or SC - both are being used overseas. Pharmac
wil provide an update on whether any additional supply likely to be IV or SC.
• Baricitinib – stock may be received by end of November 2021. Sourced 500 treatment
courses and working with supplier to source long term.
• Casirivimab + imdevimab (Ronapreve) – no update to provide. Expecting the advice from
the Pharmac COVID Treatments Advisory Group to be out by next week.
• Pfizer antiviral – in discussions with Pfizer to negotiate an advance purchase agreement.
• Molnupiravir – 60000 doses already secured, working on paperwork.
• Evusheld - in discussions with AstraZeneca – confidentiality agreement signed.
• Lenzilumab – no update to provide.
Issues discussed:
1982
Baricitinib/ tocilizumab
• Identified that guidance on baricitinib use needed to be added to clinical guideline as soon
Act
as feasible given likely availability as an alternative to tocilizumab. Tocilizumab is being
sourced by Pharmac and is the preferred agent. Guidance needed regarding use of
tocilizumab versus baricitinib in patient subgroups (eg, pregnancy, renal impairment) and
order of preference for use would be helpful - particularly for clinicians who have limited
experience working with COVID-19.
• Medsafe asked for comment on approval status: tocilizumab is currently approved for
rheumatoid arthritis. As an approved medicine it can be prescribed for other indications.
Information
Baricitinib is not currently approved by Medsafe. Unapproved medicines can be used
under Section 29.
• Tocilizumab – a member expressed concern about the complexity of using SC formulation
to prepare an IV infusion based on the information provided by the company. It was
Official
suggested by the member that baricitinib be preferred over SC formulation of tocilizumab
for the majority of ward-based care as per most international guidelines e.g. Australia.
the
Noted by Pharmac that the issue of SC tocilizumab may need to be considered more fully
with further discussion/advice sought.
Action: Guidance on use of baricitinib to be introduced into the guideline ‘Clinical Management of
COVID-19 in Hospitalised Adults’ and next guideline update to be brought forward.
under
Ronapreve
• An update from Pharmac was sought by members on patient criteria Pharmac wil be
recommending (in general terms of wide access or patient subgroups only). Pharmac
advised that this information has yet to be finalised and wil be provided in the summary
from the Pharmac COVID Treatments Advisory Group due out by next week which wil be
circulat
Released ed to the Therapeutics TAG.
• Members raised specific issues relating to Ronapreve of relevance to clinical and health
system use:
If Ronapreve is expected in advance of molnupiravir this may change the
perspective on community use of Ronapreve.
Serology testing – wil the recommended use require this. Implications for access
to testing and treatment.
Document 6
Information on the number needed to treat (NNT) for benefit for Ronapreve and
other products of interest to the group and anticipated to be in the summary of
information provided from the Pharmac advisory group October meeting.
4.0
Equity considerations
Oral antivirals
Initial thoughts on supporting models of care for delivering molnupiravir
and oral antivirals in the
community from an equity perspective:
• Ensuing appropriate access to testing and fast processing times. Query whether saliva
testing wil be widely available.
• Accessibility to treatments - offering antivirals to the patient within time needed for
treatment benefit (for molnupiravir this is within five days of symptom onset). Also ease of
access to medicine supply via pharmacy/ delivery etc.
• Providing appropriate information, for example a patient information sheet on the treatment
1982
was suggested as desirable. Information provided through media channels was also
suggested but it was recognised that messaging around the importance of vaccination was
Act
the key message to communicate.
• Several barriers were discussed, such as hesitancy for testing, speed of access to test
results, medical prescribing only (limited GP access in some rural areas); potential
financial barriers (e.g. if script co-payment required; transport costs to testing centre etc.).
• Ministry attendees noted that there was some work happening to address some of these
barriers within the Care in the Community programme. There is also work progressing in
the Ministry regarding Pharmacy Services. The draft document COVID-19 Primary Care
Information
Clinical Model – Pharmacy Services was circulated to indicate what community pharmacy
can/may deliver.
• A member suggested that it is likely that barriers may be faced by the index case in the
household but that with proactive support/treatment as needed for the household as a
Official
whole, barriers to care could be reduced.
• There was general discussion about the prescribing of medications. It was suggested by a
the
member that COVID-19 therapies be added to the list of medicines able to be
prescribed/ordered by non-medical practitioners to assist with capacity and accessibility
issues.
under
• A Ministry attendee suggested that there may be a need to prioritise treatments and a risk
stratification may be required to understand the communities who may be at high risk and
have accessibility barriers.
• A member noted that the link between therapeutics and community testing is important,
especial y to facilitate the provision of a ‘bundle’ of services to people, rather than multiple
channels and visits.
Released
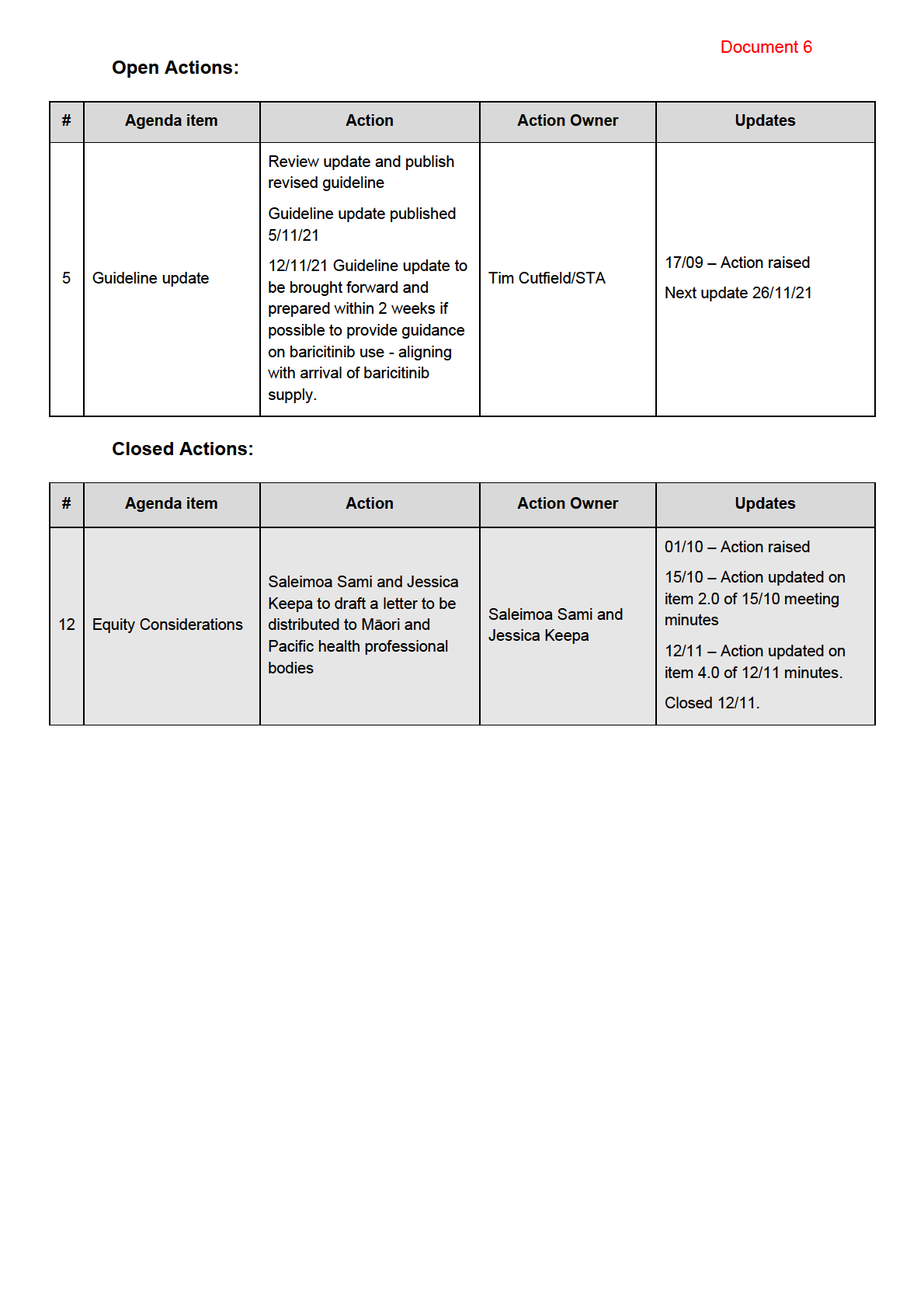
Letter to relevant Maori & Pacific professional organisations
• The letter requesting feedback for the Therapeutics TAG from Māori and Pacific health
organisations is going out to all organisations this week and feedback wil be reported to
the next Therapeutics TAG meeting.
5.0
Primary Care – progress in aligning work
• Chair attended the CAG group meeting where Therapeutics TAG Position Statement on
Inhaled Budesonide Use was tabled for information. A list of members of the CAG
interested in being part of a subgroup on therapeutics was collated at the meeting.
Document 6
• There was discussion about a Therapeutics TAG subgroup to act as a liaison group with
CAG although it was noted that the CAG group itself is nearing the end of its planned
work programme. Initial thinking is that the Therapeutics TAG could support with guidance
on treatments for COVID-19 in the community and some members expressed interest in
involvement if a Therapeutics TAG subgroup for this liaison purpose was formed.
6.0
Guideline Update
• The guideline was updated on 05 November 2021. Link available here.
• This was a substantive update, in particular in the inclusion of specific advice for
management of COVID-19 in pregnancy.
• A system for documenting changes made in each update and associated rationale has
commenced with the 5 November update. This wil be used prospectively and will assist
with any queries.
• The next planned monthly update is 03 December 2021. This update may include hospital
1982
use of Ronapreve. An earlier update later in November now seems required given
baricitinib supply potentially in 1-2 weeks. A guideline subgroup meeting wil be convened
within the next week.
Act
Action: Next Guideline update to be brought forward and prepared within 2 weeks if
possible to provide guidance on baricitinib use - aligning with arrival of baricitinib supply.
7.0
Patient Information Update
COVID Resources – Health Navigator
• ‘COVID-19 positive - Consumer resources for care in the community’ was provided with
Information
the agenda as an update of what is being produced.
It was noted several medication specific information sheets have been circulated without any
changes needed which the group agreed was an indication of the quality of the work. The
publication of these products into other language is stil being followed up within the Ministry.
Official
8.0
Booklet – COVID-19 rehabilitation
the
Booklet titled ‘
Support for rehabilitation: self-management for COVID-19-related il ness’ was
provided with the agenda for information.
• The booklet has been modified from the WHO version and brought into the Aotearoa New
Zealand context.
under
• Members suggested that the title could cause confusion for the intended audience. The
booklet focuses on the post-acute phase however this could be misunderstood and cause
a delay in seeking treatment. Comments received wil be fed back to the author and the
revised booklet wil be brought back to the next meeting with a view to endorsement from
the group if deemed appropriate.
Released
10.0
Agenda Items for Next Meeting
Booklet – COVID-19 rehabilitation – for discussion
11.0
Action Items Raised During Meeting
Action: Next Guideline update to be brought forward and prepared within 2 weeks if possible to
provide guidance on baricitinib use - aligning with arrival of baricitinib supply.
Meeting closed at
2:30pm Next meeting
Friday 26 November 2021 – 1:30pm – 2:30pm
1982
Act
Information
Official
the
under
Released