




133 Molesworth Street
PO Box 5013
Wellington 6140
New Zealand
T+64 4 496 2000
23 May 2022
Harold
By email: [FYI request #17035 email]
Ref: H202204655
Tēnā koe Harold
Response to your request for official information
Thank you for your request under the Official Information Act 1982 (the Act) to the Ministry of
Health (the Ministry) on 28 March 2022 for:
“For the two advisory groups:
1) COVID-19 Testing Technical Advisory Group
2) COVID-19 Therapeutics Technical Advisory Group
I would like to request copies of
1) All meeting minutes
2) All reports or advice they have produced and submitted to any minister dated since 25
Jan 2022.”
Regarding the first part of your request, the minutes for the COVID-19 Testing Technical
Advisory Group and the COVID-19 Therapeutics Technical Advisory Group from 25 January
2022 to the date of your request are attached and are outlined in the table in Appendix 1. Where
information has been withheld in part, this is noted in the documents themselves. Where
information has been withheld under section 9, I have considered the public interest but do not
consider it outweighs the need to withhold the information at this time.
Regarding the second part of your request, neither advisory group produces or submits reports
or advice to any Minister, therefore this part of your request is refused under section 18(e) on
the grounds that the information requested does not exist.
Under section 28(3) of the Act, you have the right to ask the Ombudsman to review any
decisions made under this request. The Ombudsman may be contacted by email at:
[email address] or by calling 0800 802 602.
Please note that this response, with your personal details removed, may be published on the
Ministry website at:
www.health.govt.nz/about-ministry/information-releases/responses-official-
information-act-requests.
Nāku noa, nā
Gill Hall
Group Manager, Science, Surveillance & Insights
COVID-19 Health System Response
Appendix 1: Documents for release
# Date
Title
Decision on release
1 11 March 2022
COVID-19 Testing Technical
Withheld in full under section
Advisory Group Minutes
9(2)(f)(iv) to maintain the
constitutional conventions that
protect the confidentiality of
advice tendered by officials.
2 23 March 2022
COVID-19 Testing Technical
Some information withheld
Advisory Group Minutes
under the following sections of
the Act:
• section 9(2)(f)(iv); and
• section 9(2)(k) to prevent
the disclosure or use of
official information for
improper gain or advantage.
3 28 January 2022 COVID-19 Therapeutics Technical Some information withheld
Advisory Group Minutes
under section 9(2)(k).
4 11 February 2022 COVID-19 Therapeutics Technical
Advisory Group Minutes
5 25 February 2022 COVID-19 Therapeutics Technical
Advisory Group Minutes
6 11 March 2022
COVID-19 Therapeutics Technical Some information withheld
Advisory Group Minutes
under the following sections of
7 25 March 2022
COVID-19 Therapeutics Technical the Act:
Advisory Group Minutes
• section 9(2)(b)(ii) to protect
information where the
making available of the
information would
unreasonably prejudice the
commercial position of the
person who supplied the
information; and
• section 9(2)(k).
Page 2 of 2

Document 2
MINUTES: COVID-19 Testing Technical Advisory Group
Date:
23 March 2022
Time:
12:30pm to 1:30pm
s9(2)(k)
1982
Location:
ACT
Chair:
Kirsten Beynon
Members:
Maia Brewerton, Patricia Priest, Susan Morpeth, Tim Blackmore, David Murdoch
Ministry of Health Attendees: Ian Town, Mark Ayson, Christian Marchello
Guests:
Apologies:
Pisila Fanolua
INFORMATION
1.0
Welcome and Previous Minutes
Kirsten Beynon welcomed all Members and Attendees in her capacity as Chair of the COVID-19 Testing
Technical Advisory Group (CT TAG).
Minutes of the last meeting (11 March 2022) were accepted.
OFFICIAL
2.0
Update on Open Actions
Actions 4 and 6 are currently in progress.
THE
3.0
Testing Strategy Update
This is in progress.
Surveillance papers have been sent to members.
Feedback from COVID-19 Technical Advisory Group to be shared with members for oversight.
UNDER
4.0
Antibody and Immunity testing
In response to the announcement of a serology test becoming available at pharmacies the Ministry has
requested CT TAG to advise on when and why serology antibody testing should be used. Members are to
develop key messages to feedback to the Ministry and Ministers.
The Chair apologises for the lateness of the document re: Serology Testing for COVID and appreciates
members weren’t given time for detailed observations.
RELEASED
The Chair asks for all members input into this document and welcomes any comments via email by Friday
25 March 2022.
The document will formulate advice for the appropriate use of serology testing for SARS-CoV-2
and brings together information from international guidance for antibody and immunity testing.
Document 2
A member noted the importance of including information and need for wider methods of immunity
testing i.e. pseudo neutralisation assays. The Chair supports this information being included in the
document.
A high-level executive summary will be created from the information gathered in the document.
This summary is intended for the DG and will also be used to feedback to other Technical
Advisory Groups.
ACTIONS:
The Chair asks for all members input into this document and welcomes any comments by Friday
25 March 2022.
Document to be shared with NZNM and Immunology groups via Dr Brewerton for comment.
1982
5.0
CV TAG Statement on Utility of Antibody Testing
A member commented on a point raised in COVID-19 Vaccine Technical Advisory Group noting concern
in members around public access to testing without clinical oversight. This was noted. .
ACT
6.0
Testing Strategy and Plan
The final testing strategy and plan is due early April for the Director-General and Ministers and will be
used for guidance into the future
Chair will send out the document re: Director-General memo on a revised testing strategy. Noting this is a
work in progress.
Chair welcomes all members feedback and comments either via email or in next meeting.
Chair stresses the approach of ‘form follows function’: identifying gaps, what sits under public
health, health NZ, and business guidance including considerations for different phases. To also
consider how we would deliver the information.
INFORMATION
The Ministry of Health noted CT TAG’s specific input will be commissioned on seroprevalence in
particular sampling frame considerations.
7.0
OIA Requested
The following OIA request was included in the agenda for noting.
Copies of meeting minutes from the 'COVID-19 Technical Advisory Group' and 'COVID-19 Testing
Technical Advisory Group (CT TAG)' groups between 28 October and now
OFFICIAL
8.0
Next Steps/Decisions Pending
Two placeholder meetings to be set up for following two weeks to discuss feedback on draft strategy
THE
9.0
Any Other Business
10.0
Agenda Items for Next Meeting
UNDER
Members comments and input on strategic plan
11.0
New Action Items Raised During Meeting
#
Agenda item
Actions
Action Owner
The Chair asks for all members input
into this document and welcomes
7
Antibody and Immunity Testing
Chair
any comments via email by Friday
RELEASED
25 March 2022.
Document 2
Document to be shared with NZNM
8
Antibody and Immunity Testing
Susan Morpeth
for comment.
Updated documents to be circulated
9
Testing Strategy
Chair
to CT TAG for further input
Meeting closed at 1:13pm
Next meeting: TBD
1982
Open Actions:
#
Agenda item
Actions
Action Owner
Updates ACT
s 9(2)(f)(iv)
4
6
The Chair asks for all members
INFORMATION
Serology Antibody
input into this document and
7
Chair
23/03 – Action raised
Testing
welcomes any comments via
email by Friday 25 March 2022.
Serology Antibody
Document to be shared with
8
Susan Morpeth
23/03 – Action raised
Testing
NZNM for comment.
OFFICIAL
Updated documents to be
9 Testing Strategy
circulated to CT TAG for further
Chair
23/03 – Action raised
input
THE
Closed Actions:
#
Agenda item
Actions
Action Owner
Updates
UNDER
To send the COVID-19 Testing
Strategy and Surveillance
11/03 – Action raised
5
Strategy documents to CT TAG
Chair
members for discussion in
12/03 – Action closed
following meeting.
RELEASED

Document 3
COVID-19 Therapeutics Technical Advisory Group
MINUTES: Te Rōpū Haumanu Kowheori-19
Date:
Friday 28 January 2022
Time:
1:30pm to 2:30pm
1982
s9(2)(k)
Location:
ACT
Chair:
Nigel Raymond
Members:
Colin McArthur, Eamon Duffy, Jessica Keepa, Saleimoa Sami, Susan Morpeth, Tim Cutfield
Attendees:
Andi Shirtcliffe, Andrew Oliver, Anne Buckley, Derek Fitzgerald, Josh Wiles, Ian Town,
Phoebe Currie
INFORMATION
Guests:
Pauline Horril
Chris Hopkins, Elaine Yap, Michael Maze, Daniel Bernal, Justine Lancaster, Mark Ayson,
Apologies:
Therese Egan, Adrienne Martin, Rachel Webb
Welcome and Accept Previous Minutes
OFFICIAL
1.0
Dr Nigel Raymond welcomed al members and attendees in his capacity as Chair of the COVID-19
Therapeutics Technical Advisory Group.
THE
Minutes of the last meeting (14 January 2022) were accepted.
Therapeutics
2.0
Pharmac Update
•
The December meeting record of Pharmac’s COVID-19 Treatments Advisory Group is stil being
UNDER
finalised.
•
Pharmac was aware of some rheumatology patients being transferred to the stock of
subcutaneous tocilizumab that is available, in order to preserve the IV tocilizumab for COVID-19
patients. Further supply of IV tocilizumab has been secured.
•
Pharmac approached Roche and Baxter regarding the request for information on the stability of
tocilizumab after conversion from subcutaneous to IV, however the information isn’t currently
available.
RELEASED
•
Pharmac is currently processing the feedback provided to the notification about eligibility criteria
for baricitinib, and casirivimab and imdevimab (branded as Ronapreve).
•
Pharmac is planning to open consultation on the eligibility criteria for molnupiravir and Paxlovid
shortly.
Document 3
• Pharmac’s COVID-19 Treatments Advisory Group will discuss remdesivir at the next meeting, with
a focus on possible use earlier in the disease course. Remdesivir is a Section 29 (s29) product –
this adds to the potential complexity of community use.
• Pharmac is in discussion with Gilead and is planning for further supplies of remdesivir in increased
volumes considering the anticipated increase in cases.
• Pharmac is in active discussions with GSK regarding sotrovimab.
• Pharmac noted there are regular meetings between Pharmac and the Ministry COVID Care in the
Community team to keep them informed.
Discussion
1982
• A member asked about budesonide and Pharmac noted that there are ongoing supply
discussions.
ACT
• An attendee asked about Evusheld and Pharmac noted they are progressing discussions with
AstraZeneca.
Medsafe Update
• Medsafe noted that there is no indication of when an application for Evusheld may be expected.
• Medsafe have noted the known reduction in effectiveness of Ronapreve against Omicron and the
potential need for communication with the sector about this.
• Medsafe is progressing the Paxlovid application and expecting to take this forward to the
Medicines Assessment Advisory Committee (MAAC) shortly. It was noted that Paxlov
INFORMATION id has
provisional approval in Australia.
• Medsafe has completed the evaluation of the remdesivir application and has issued a request for
further information.
• Medsafe is expecting an application for approval for molnupiravir in February. It was noted that
molnupiravir has provisional approval in Australia.
OFFICIAL
Discussion
• Discussion about the s29 process in the context of COVID-19 was raised by Pharmac. This related
to practical aspects of medicine delivery once prescribed. Medsafe wil provide further clarification
THE
to Pharmac.
• A member raised a question about selective serotonin reuptake inhibitors (SSRIs), in particular
fluvoxamine. It was noted that these may be considered by Pharmac’s COVID-19 Treatments
Advisory Group in a future meeting, but that there is currently limited evidence available. Athough
fluvoxamine was previously approved for non-COVID-19 indications, Medsafe has been informed
UNDER
by the company that it is not available. If it is required for use, the company should be contacted
regarding its current status.
Paxlovid in the context of Omicron
• The Chair raised a question about the timeline of the Paxlovid application and supply, noting the
potential benefits of Paxlovid as an oral treatment rather than infusion and the increasing clinical
conc
RELEASED ern given the projected surge in Omicron cases. The question was raised as to whether there
was any further action that could be taken to expedite timely arrival/distribution of Paxlovid.
Pharmac noted that discussions with Pfizer are moving quickly and that the Medsafe approval is
one of the triggers for delivery. It was noted that the application is progressing.
Document 3
• A member queried if there are any operational needs to consider if Paxlovid is approved. It was
suggested that it would be helpful to have concise, straightforward guidance on interactions, their
significance and what to do if a patient is on the medicines involved. It was noted that there may
be international guidance/resources that could support development of guidance.
• A query was raised to Pharmac by a Ministry attendee about resourcing available to produce
information for pharmacists and primary care. Pharmac suggested liaison with the relevant team
member within Pharmac.
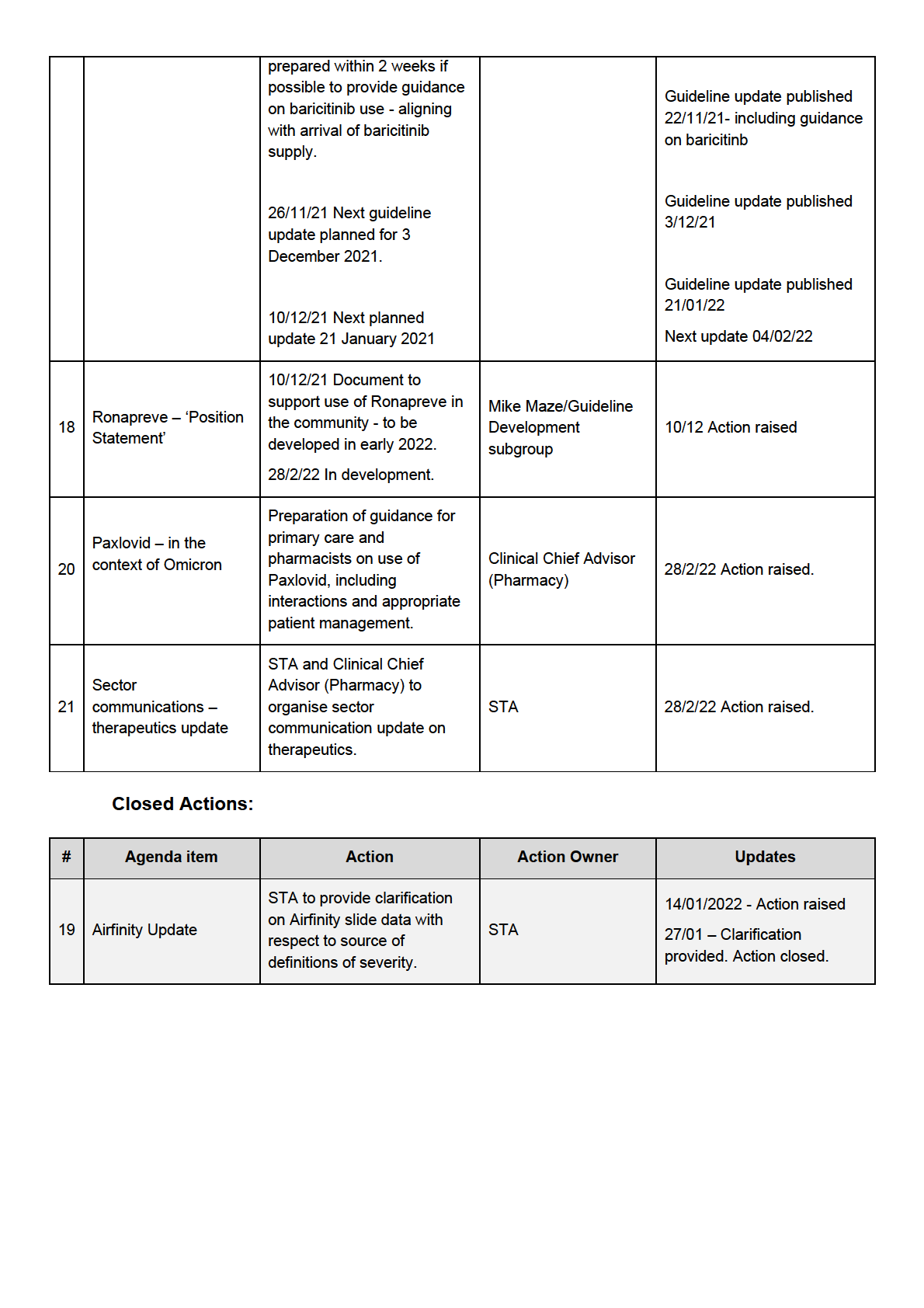
Action: Clinical Chief Advisor (Pharmacy) to liaise with Pharmac team member advised on preparation of
guidance for pharmacists and primary care practices on the use of Paxlovid, focusing on interactions, their
significance, and the appropriate management.
1982
Remdesivir use in immunocompromised
ACT
• A member raised a question about the use of remdesivir earlier in the disease course for this
group, noting some countries have incorporated this into their approach to Omicron. It was noted
that the access criteria for remdesivir are to be discussed next week by the Pharmac COVID-19
Treatments Advisory Group.
Airfinity/STA Update
• ‘
Highlights from Airfinity Therapeutics Report 21st Jan 2022’ was circulated with the agenda for
noting.
• The STA-produced excerpt from the latest Variant of Concern – Omicron Update on th
INFORMATION erapeutics
was circulated with the agenda for noting.
Covid Care in the Community/Ministry update
3.0
• It was noted that the Ministry responded to the Pharmac consultation for patient access criteria for
baricitinib and casirivimab/imdevimab (branded as Ronapreve). The submission was circulated
with the agenda.
OFFICIAL
• An update was given on the ongoing work in the COVID Care in the Community team, requesting
the groups’ feedback on how therapeutics can be incorporated.
THE
• Development of the ‘Population level risk stratification tool’ was outlined, noting that the system
would provide an initial estimation of risk of severe disease or hospitalisation (based on Delta
data) for each person based on age, deprivation, ethnicity, vaccination status and enrolment
status, linked to NHI number. It was noted there are stil many aspects to be worked through
including ethical constraints and data validity.
UNDER
• Different levels of care are being considered based on risk and dynamic symptom monitoring. The
pre-diagnosis algorithm is stil being finalised. Different pathways (self-management or active
management) would be provided based on the initial assessment; however, people would be able
to ‘change lanes’ as needed at any time. It was emphasised that resource distribution and equity
are a key focus of this tool. High levels of patient self-management are expected given the
anticipated increase in case numbers.
Discussion/feedback
• A m
RELEASED ember raised a question about the dataset and extrapolation of the data to Omicron cases.
The COVID Care in the Community representative noted that the tool is designed to be updated
over time and that a wide group of data experts are working to ensure the tool can be adapted
quickly.
Document 3
• A member noted that while pragmatic for community management, rough grouping can be difficult
from a therapeutics perspective. Depending on the agent, groupings may be too crude to
accurately identify people who appropriately meet criteria for a specific therapeutic intervention.
• The group noted that including comprehensive details of vaccination status is important -
especial y differentiating between a third primary dose and a booster dose, as this could serve as
a signal of patients with known risk factors or immunocompromised status.
• The group raised several equity aspects as an important part of the feedback and noted concerns
about whether those who most need monitoring in the community would receive it, given they may
not be enrolled with primary care, for example. The COVID Care in the Community representative
noted that equity is a key focus, many of these points are being considered and the idea of the tool
1982
is that people who need more support are identified and appropriately triaged to receive it. All
feedback was welcomed.
o Members had concerns about relying on patients entering data, as a large number of
ACT
people aren’t digital y enabled. Access to a phone (with credit, reception, and data) is not
something everyone has and is particularly important for remote communities.
o A member raised the importance of language and wording in the information sent to
people about symptoms. Health literacy differs and it is important that information is
accessible.
o A member suggested that geographical location (rurality) be included as a parameter of
risk.
Equity Considerations
4.0
INFORMATION
• A member discussed a recent hui with Te Rōpū Whakakaupapa Urutā (National Māori Pandemic
Group). Hospital and primary care doctors who are preparing for Omicron are keen to know more
about the timelines for antivirals.
• It was suggested that some preliminary information on antivirals would be helpful, so that health
professionals can prepare and educate themselves on their use before they are having to use
them. This was also a concern raised in the Pacific health community.
OFFICIAL
• There are concerns around potential logistical issues of distribution of therapeutics that could
exacerbate geographical inequities, particularly on the East Cape.
• There are concerns around the access criteria for antivirals and how that wil affect those in Level
THE
1 hospitals/rural settings. Pharmac noted that therapeutics wil be made available via DHBs for
their distribution as appropriate including to primary care and Level 1 hospitals.
Guideline Update
5.0
• The guideline was last updated on 21 January 2022. The next planned update is 04 March 2022 –
UNDER
this is expected to be brought forward (as Pharmac access criteria for Ronapreve taking effect
from 1 February 2022).
Next Guideline Update
• There was discussion about preparing guidance on Ronapreve, specifically for use for confirmed
Delta cases given its known limitations in treating Omicron. While important as there are stil Delta
infections in New Zealand, it was noted that criteria for use based on Whole Genome Sequencing
(WGS) was unsuitable as it is not set up as part of a clinical diagnostics pathway. Of note, WGS is
RELEASED done at PH direction, results not visible to clinicians, anticipated increased use of Rapid Antigen
Tests (RATs) etc all make use of WGS criteria impractical. Noted that infections are increasingly
likely to be Omicron and this needs to be reflected in recommendation wording.

Document 3
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
Document 3
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED

Document 4
COVID-19 Therapeutics Technical Advisory Group
MINUTES: Te Rōpū Haumanu Kowheori-19
Date:
Friday 11 February 2022
Time:
1:30pm to 2:30pm
1982
s9(2)(k)
Location:
ACT
Chair:
Nigel Raymond
Members:
Chris Hopkins, Eamon Duffy, Elaine Yap, Michael Maze, Susan Morpeth
Attendees:
Andrew Oliver, Anne Buckley, Daniel Bernal, Derek Fitzgerald, Josh Wiles, Ian Town,
Phoebe Currie
Guests:
Therese Egan, Rachel Webb
INFORMATION
Apologies:
Colin McArthur, Jessica Keepa, Saleimoa Sami, Tim Cutfield, Andi Shirtcliffe, Justine
Lancaster, Mark Ayson
Welcome and Accept Previous Minutes
1.0
Dr Nigel Raymond welcomed al members and attendees in his capacity as Chair of the COVID-19
OFFICIAL
Therapeutics Technical Advisory Group.
Minutes of the last meeting (28 January 2022) were accepted.
THE
Therapeutics
2.0
Pharmac Update
•
Pharmac is stil finalising the record for the December meeting of the Pharmac COVID-19
Treatments Advisory Group.
UNDER
•
The Pharmac COVID-19 Treatments Advisory Group met to discuss updated data on the use of
remdesivir earlier in the disease course. The meeting record is being finalised and consultation on
eligibility criteria will follow.
•
Remdesivir is not currently listed in the Pharmaceutical Schedule but is to be added.
•
Pharmac is working with Gilead in planning for ongoing supply of remdesivir and has secured
another shipment.
RELEASED
•
Pharmac is continuing to engage with GSK regarding sotrovimab.
•
Pharmac has received further advice from the Pharmac COVID-19 Treatments Advisory Group
regarding oral antivirals (Paxlovid and molnupiravir). Pharmac consultation on Paxlovid and
Document 4
molnupiravir eligibility criteria is due out next week and feedback from the Therapeutics TAG is
welcomed.
• Pharmac is in regular communication with the Ministry COVID Care in the Community team about
therapeutics for potential community use.
Discussion
• A member raised a question regarding the timeline for oral antivirals and Pharmac noted it is
working at pace to finalise agreements and it is understood there is progression through Medsafe.
• An attendee raised a question regarding availability and timelines for sotrovimab. Pharmac noted
1982
this wil be a key product once available. At this stage, it is not anticipated to be available until Q3
at the earliest.
• An attendee raised a question regarding the draft sector communications and the drafted
ACT
availability timeline for the oral antivirals of April. Pharmac noted that the delivery dates are not
finalised, and that molnupiravir may not be available as early as Paxlovid.
Medsafe Update
• Medsafe has received all quality, manufacturing and clinical information for Paxlovid and the
request for information to Pfizer has been assessed. A final request for information has been
issued and is currently with Pfizer. It was noted that Paxlovid now has conditional approval in
Europe.
• Medsafe is continuing discussions with MSD regarding an application for molnupiravir and
anticipates an application.
INFORMATION
Discussion
• A member raised a question regarding the status of remdesivir. Medsafe noted that the company
has the initial evaluation request for information and Medsafe are waiting on a response.
• Pharmac asked about the progression of the ‘Dear Healthcare Professional Letter’ updating on
Ronapreve. Medsafe noted this should be available on the Medsafe website shortly.
OFFICIAL
Airfinity/STA Update
THE
• ‘
Highlights from Airfinity Therapeutics Report 7th Feb 2022’ was circulated with the agenda for
noting. Key points included recent information on remdesivir and fluvoxamine and the WHO
recommendations for baricitinib and sotrovimab.
Therapeutics Update for the
UNDER
health sector
• STA reported progress on the therapeutics update for the health sector - open action #21 ‘Sector
communications – therapeutics update’.
• A draft has been developed and discussion with the Ministry communications team regarding
distribution channels is progressing.
• The draft was shared within the meeting and specific feedback was provided.
• Members noted that having an update, especial y regarding potential timelines of treatment
RELEASED availability, released as soon as possible would be beneficial and assist in answering queries,
particularly from medical col eagues.
Document 4
•
Members suggested a key inclusion would be the indication of differences in Aotearoa New
Zealand, compared to the Australian context, as that is often the comparison due to information
coming from specialist colleges etc.
•
Pharmac noted it would be helpful to include a hyperlink through to eligibility criteria on Pharmac
website for Ronapreve.
•
Members suggested it was key to include the Aotearoa New Zealand context about:
o What treatments are currently available
o What treatments are expected
o What treatments are not expected
1982
o What treatments are advised against
•
Once approved by Pharmac and Medsafe, this communique wil be published on the Ministry
ACT
health professionals page and distributed in discussion with the Ministry Communications team.
•
It was agreed that the intention of this communique is to provide clarity around current and
possible COVID-19 treatments in Aotearoa New Zealand, not providing details of administration –
that is the purpose of the guideline.
•
Feedback from the meeting wil be addressed and STA will circulate the revised draft for review by
members.
Equity Considerations
3.0
•
No issues were raised for discussion and due to apologies for this meeting, the Chair requested
INFORMATION
that this item be addressed at the next meeting.
Paediatric Update
4.0
•
It was noted that the communique for the health sector would be helpful to share with paediatric
sub-specialist col eagues who have queries about timelines for delivery of oral antivirals and
monoclonal antibodies.
OFFICIAL
•
A member raised a question regarding remdesivir use in children and it was noted that this is
already in the current Starship paediatric guideline
Covid-19 Disease in Children here and that
remdesivir has been used in Melbourne and Sydney in response to recent outbreaks.
THE
Ronapreve Practical Guidance document
5.0
Feedback, sign off & distribution strategy
•
The Ronapreve Practical Guidance document is now in the final draft stage and members
feedback has been incorporated and circulated back to the group for final sign off.
UNDER
•
The distribution of the ‘Ronapreve Practical Guidance document’ wil occur next week through the
same process as the Guideline. The Ronapreve Practical Guidance document wil be published
on the Ministry’s Health Professional web page once finalised. Members wil circulate to their
networks as appropriate eg. ID pharmacy group, TSANZ.
•
Members noted that the timeline for the use of Ronapreve was limited due to its reduced efficacy
against Omicron.
•
There was a discussion on the value of developing advice around the potential locations where
RELEASED Ronapreve use may stil be appropriate. It was noted that there is geographical data for Whole
Genome Sequencing (WGS) that could possibly be accessed to support guidance provided by the
Therapeutics TAG.
Document 4
•
Members noted that it had been agreed that using WGS as a clinical diagnostic wasn’t appropriate
to set up in a reasonable time frame, given that it would lose relevance in an Omicron dominant
outbreak.
•
It was noted that Public Health teams have greater awareness of the clusters and could support
and provide further information. Geographic information around clusters would be helpful for
clinicians to support treatment decisions in the absence of WGS.
•
In some instances, requesting a microbiology lab to send a sample to ESR for WGS could be
possible and valuable, but it cannot be guaranteed that it will be available for treatment decisions.
•
Members discussed that some remaining Delta dominant areas could still be utilising Ronapreve.
It was suggested that connection with Primary Care in these areas is required to support
1982
implementation.
Action: Chair and STA to prepare a Memo to the COVID Care in the Community team, advising that
ACT
Ronapreve remains appropriate for patients with a Delta infection and highlighting the ESR WGS
geographical reporting which could be used to support implementation.
Guideline Updates
6.0
Previous updates - 1&4 February
•
The ‘Clinical management of COVID-19 in hospitalised adults’ guideline was updated on 1 & 4
February 2022. The next planned update is 4 March 2022.
Next update
•
Members continued the discussion regarding the limited timeline for use of Ronapreve and the
INFORMATION
limited access to WGS outside hospital. Members discussed the possibility of utilising ESR WGS
geographical reporting to gain insight into the variants by region and support treatment decision
making.
•
A member shared a report from ESR and showed the group an example of the type of data that
could be accessed. It was suggested that the Chair request wider distribution of the ESR WGS
geographical reporting for supporting treatment decisions on Ronapreve.
OFFICIAL
Action: Chair to email ESR and request a wider distribution of the ESR WGS geographical reporting for
supporting treatment decisions on Ronapreve.
THE
Any Other Business
6.0
There was no other business discussed.
Agenda Items for Next Meeting
8.0
•
Equity considerations
UNDER
New Action Items Raised During Meeting
9.0
Action: Chair and STA to prepare a Memo to the COVID Care in the Community team, advising that
Ronapreve remains appropriate for patients with a Delta infection in specific geographical areas.
Action: Chair to email ESR and request a wider distribution of the ESR WGS geographical reporting for
supporting treatment decisions on Ronapreve.
RELEASED
Meeting closed at
2:29pm Next meeting 25
February 2022 – 1:30pm to 2:30pm

Document 4
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED

Document 4
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED

Document 5
COVID-19 Therapeutics Technical Advisory Group
MINUTES: Te Rōpū Haumanu Kowheori-19
Date:
Friday 25 February 2022
Time:
1:30pm to 2:30pm
1982
s9(2)(k)
Location:
ACT
Chair:
Nigel Raymond
Members:
Chris Hopkins, Colin McArthur, Eamon Duffy, Elaine Yap, Jessica Keepa, Saleimoa Sami,
Susan Morpeth, Tim Cutfield
Attendees:
Andrew Oliver, Anne Buckley, Daniel Bernal, Derek Fitzgerald, Justine Lancaster, Josh
Wiles, Ian Town, Mark Ayson, Phoebe Currie
INFORMATION
Guests:
Therese Egan
Apologies:
Michael Maze, Andi Shirtcliffe
Welcome and Accept Previous Minutes
1.0
Dr Nigel Raymond welcomed al members and attendees in his capacity as Chair of the COVID-19
OFFICIAL
Therapeutics Technical Advisory Group.
Minutes of the last meeting (11 February 2022) were accepted.
THE
Matters Arising – The Therapeutics Update for Health Professionals document was circulated with the
agenda. This final version included input from Pharmac and Medsafe.
Therapeutics
2.0
Pharmac Update
UNDER
•
Pharmac have opened the consultation on access criteria for molnupiravir (Lagevrio) and
nirmatrelvir with ritonavir (Paxlovid). Pharmac noted the consultation is an agenda item for this
meeting and welcomed feedback from the group or individuals. The consultation closes on 2
March 2022.
•
Pharmac is continuing to progress negotiations on details of supply agreements for molnupiravir
and Paxlovid.
•
Remdesivir – 5000 vials have arrived in Aotearoa New Zealand. Pharmac expects these to be
receipted by the wholesaler today. After the recent results of the PINETREE study, global supply
RELEASED of remdesivir is constrained and Pharmac is working with Gilead to secure more stock as a
measure before other agents such as oral antivirals become available.
•
Tocilizumab - additional stock was delivered in January this year. Global stocks of IV and
subcutaneous tocilizumab remain constrained and this is expected to continue.
Document 5
• Baricitinib is now listed on the Pharmaceutical Schedule with the same criteria as tocilizumab.
DHBs can order. Small regular orders as required will assist in managing stock levels.
• Pharmac noted no change for Ronapreve since the last update - stock remains available.
• The next Pharmac COVID-19 Treatments Advisory Group meeting is on 28 February 2022 and wil
focus on fluvoxamine and ivermectin. Pharmac is aware of the international consensus that
ivermectin is not recommended for use as a COVID-19 treatment and aims to publish advice in
order to formalise the group’s recommendations, inform the public and assist in responding to
ongoing queries about ivermectin for COVID-19.
• Sotrovimab and Evusheld - Pharmac expects to be able to provide further updates in the coming
weeks.
Discussion
1982
• A member raised a question regarding the incoming remdesivir stock. Pharmac confirmed the new
stock is the same product as available currently, which is the powder rather than the solution.
• A member commented that there are ongoing queries from clinicians regarding remdesivir acce
ACT ss
criteria. Pharmac noted that additional information regarding access criteria is expected to be
released on 28 February. It was noted that this timing will align with preparation of the next
guideline due to be published 4 March 2022.
Medsafe Update
• The Paxlovid application has been through the Medsafe process and was considered by the Medicines
Assessment Advisory Committee (MAAC) on 24 February 2022. A decision may be made on whether
to grant approval next week.
INFORMATION
• Medsafe received an application from MSD for molnupiravir last week and an evaluation is now
underway. It is an abbreviated application, based on an application to an overseas regulator and
Medsafe have already received al the data needed for evaluation.
• Remdesivir evaluation - Medsafe have made a further request for information to Gilead and are
awaiting a response.
OFFICIAL
Airfinity/STA Update
• ‘
Highlights of Airfinity report 18 February 2022’ was circulated with the agenda for noting. A
selection of key updates was inc
THE luded, such as recent information on oral antivirals.
•
‘Trends and Insights Report – 24 February 2022’ was circulated on the day of the meeting as an
addition to the agenda for noting. Particularly of interest was the latest Whole Genome
Sequencing (WGS) data, which included the identified number of Delta cases.
Equity Considerations
UNDER
3.0
• Equity concerns were raised regarding the timeline of access for antivirals. It was suggested that
there are a series of potentially challenging factors that need to align in order for treatment to be
provided to those that need it most.
• Factors to be considered in the timeline for access include:
o Early testing of individuals – some individuals may not seek tests for varying reasons e.g.
distrust in the system.
o Accurate reporting of the test results – some individuals may not report their RATs results
RELEASED due to the consequences e.g. loss of income from isolating.
o Practitioners need to familiarise themselves with the eligibility criteria for new therapeutics.
It was noted that this is an increased workload on primary care.
Document 5
o Prompt delivery of prescriptions is required to ensure therapeutics can be given within the
recommended treatment window. A member suggested allowing practitioners to prescribe
early for high risk patients to ensure timely access.
o Potential supply chain disruption is a concern, especially for rural situations. Stock
distribution is important.
o Providing the appropriate information on therapeutics to patients.
• It was noted that it would be beneficial to have oral antivirals included in COVID Health Pathways.
Considering initiatives like audits/query builders to identify and flag eligible patients in advance
would be helpful.
• As the COVID response shifts to ‘self-management’, there are concerns that individuals could be
overlooked. It was noted that ideal y high risk individuals will be triaged into active management.
1982
• A member raised a query regarding pharmacies not being able to buy or hold stock. Pharmac
noted that currently oral antivirals can’t be purchased directly by pharmacies, but they wil be able
to be ordered to fil prescriptions. This approach is intended to prevent potential stockpiling by
ACT
some pharmacies but Pharmac is open to revising the distribution approach if needed.
• Ideas for addressing the equity concerns raised included: further support provided to primary care;
providing clear practical information about who needs to do what and when; incentivising
prospective planning in primary care to identify eligible patients; and increasing patient awareness
of treatments they may be eligible for through patient information sheets.
Pharmac Consultation on access criteria for oral antivirals
4.0
• Feedback on the access criteria from members by linked email discussion was provided to STA
after a request from the Chair and this was col ated and circulated as a paper with the agenda for
further discussion.
INFORMATION
• Members agreed that ‘tightening’ the criteria (increasing the number of co-morbidities) would be
beneficial overall to make the criteria more restrictive. Members supported specifying Maori and
Pacific ethnicity in the criteria to help identify those at high risk. The feedback on specific co-
morbidities provided by members by email was noted.
• Members discussed whether there was a need for the criteria to specify aspects such as drug
interactions (for Paxlovid) and need for concomitant contraceptive use (molnupiravir). It was
agreed that these aspects are not commonly included in access criteria and while important, are
OFFICIAL
more relevant to prescriber safety. It was noted that if there are broader access criteria, drug
interaction becomes increasingly relevant as the broader clinical benefit possibly reduces.
• It was noted that the COVID Care in the Community team have recently established a
THE
Therapeutics Implementation Group. Equity is a key pil ar in the framework and the
implementation plan for the roll out of therapeutics is in development. Further information is
required in order to develop the implementation plan, such as Medsafe approval status, Pharmac
access criteria, stock levels and timelines of deliveries. Further work on the plan wil be done as
information becomes available.
• Members raised equi
UNDER ty concerns about the access criteria, suggesting that they may not capture
some individuals who may benefit from oral antivirals, such as ‘mobile communities’ (individuals
not enrolled with a general practice) or those who may have a later diagnosis of risk factors such
as diabetes and hypertension due to limited contact with primary care. Members supported
allowing for risk factors to be identified through clinical suspicion.
• A member commented that under the current criteria, some practices would have a large number
of people who may be eligible. Members discussed concerns that this could increase pressure on
the health system, while the benefit of the treatment overall is reduced due to lower hospitalisation
rates
RELEASED with Omicron (compared to Delta).
• A member suggested that there were potential medicolegal implications of having wide access
criteria which could not be reflected in the delivery of treatment.
Document 5
• It was suggested that having a single set of access criteria for all antivirals for potential use in the
community would be helpful and this view was supported by the group. It was noted that prescriber
and safety information could be communicated separately to professionals to assist with
management.
Action: A Therapeutics TAG submission on two oral antivirals is to be finalised by the Chair and STA for
submission to Pharmac by March 2, taking in the feedback provided by members and the meeting
discussion.
Implications for Ronapreve
5.0
• The number of likely cases of Delta circulating in the community was discussed, informed by two
1982
ESR reports of whole genome sequencing (WGS) and the
Trends and Insights Report – 24
February 2022. The reports suggest there is very little Delta in the community.
Members noted that
the relevance of Ronapreve is now limited due to reduced efficacy against Omicron and limited
ACT
ability to complete WGS in the community.
• It was noted that Delta may be persistent for longer in hospital admissions - the Australian
experience was of a ‘long tail of Delta’ in the hospital setting, given greater severity of il ness with
Delta. Members noted that Ronapreve use in hospital may stil be relevant.
• Overall members noted that without WGS, distinguishing between Delta and Omicron at disease
onset is very difficult and dependent on knowledge of specific outbreak clusters.
• The Therapeutics TAG decided to recommend that Ronapreve should not be used in the
community in general - except for use on expert recommendation or in extenuating circumstances.
Actions:
Information on Ronapreve in the Therapeutics Update for Health Professionals is to be updated to align
with recommendation that not for general use in community. INFORMATION
Ronapreve content in the
Clinical management of COVID-19 in hospitalised adults guideline wil be
reviewed as part of the next guideline update.
Guideline Updates
6.0
• The next update of the guideline is planned for March 4 and is underway. The group discussed
changes being considered for this update including updating the discharge and disposition
sections with input from the Public Health team in the Ministry as needed. STA acknowledged a
OFFICIAL
role in facilitating this.
• Members discussed budesonide and the varying use around Aotearoa New Zealand. Some areas
have removed budesonide from use due to logistics with prescribing and other factors. The group
THE
generally agreed that therapeutic recommendations should be the same for the whole of Aotearoa
New Zealand. The subgroup will consider how to reflect this in the guideline.
• Members discussed the length of the guideline document and if there could be changes to the
current format facilitated by the Ministry to make it easier to read. STA reported preliminary
discussions with the Ministry communications team about this and that design support was
available but limited. Further suggestions of required improvements could assist with progression.
UNDER
Ease of rapid updating needs to also be considered given timeframe from final preparation of a
guideline update to publication online.
• A member suggested that the ful guideline was helpful in its current format and adding summary
flowcharts grouped by severity could be an alternative approach to improving accessibility of
information.
Any Other Business
7.0
RELEASED
There was no other business.
Agenda Items for Next Meeting
8.0

Document 5
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED

Document 5
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED

Document 6
COVID-19 Therapeutics Technical Advisory Group
MINUTES: Te Rōpū Haumanu Kowheori-19
Date:
Friday 11 March 2022
Time:
1:30pm to 2:30pm
1982
s9(2)(k)
Location:
ACT
Chair:
Nigel Raymond
Members:
Chris Hopkins, Colin McArthur, Eamon Duffy, Elaine Yap, Jessica Keepa, Michael Maze,
Susan Morpeth, Tim Cutfield
Attendees:
Andrew Oliver, Anne Buckley, Derek Fitzgerald, Justine Lancaster Josh Wiles, Phoebe Currie
Guests:
Therese Egan, Rachel Webb, James Entwisle INFORMATION
Apologies:
Saleimoa Sami, Andi Shirtcliffe, Daniel Bernal, Ian Town, Mark Ayson
Welcome and Accept Previous Minutes
1.0
Dr Nigel Raymond welcomed al members and attendees in his capacity as Chair of the COVID-19
OFFICIAL
Therapeutics Technical Advisory Group. The meeting was opened with a karakia.
Minutes of the last meeting (25 February 2022) were accepted.
THE
Therapeutics
2.0
Pharmac Update
•
Consultation on the proposed access criteria for molnupiravir and Paxlovid closed on 2 March
2022. Pharmac had good engagement, including a submission from the Therapeutics TAG.
Pharmac is working through a number of detailed responses and considering possible effects on
UNDER
the criteria. Outcomes of this process are expected in the coming weeks.
•
s 9(2)(b)(ii)
Molnupiravir is undergoing evaluation by Medsafe.
•
Paxlovid - Pharmac are expecting information on shipping arrangements for Paxlovid in the next
few weeks.
•
Remdesivir - In response to significant feedback, Pharmac made changes to the remdesivir
RELEASED access criteria on 4 March 2022. Pharmac increased the number of comorbidities required to
access the treatment, a temporary change until oral antivirals become available. There has been
interest from DHBs regarding community access to remdesivir. Pharmac noted that while stock is
available, supplies are limited, and insufficient to support wide community use at this time.
Document 6
•
Tocilizumab - The most recent delivery was in January; supply remains constrained and Pharmac
continues to work with Roche to manage stock.
•
Baricitinib stock is available from Onelink. Pharmac is monitoring usage and considering when
stock may need to be reordered.
•
Discussions regarding sotrovimab and Evusheld are progressing, and updates are expected in the
coming weeks.
•
Ronapreve stock remains available and evidence about Ronapreve and Omicron is being
monitored.
1982
Discussion
•
A member noted that the recently published RECOVERY trial results for baricitinib were likely to
lead to increased use and asked if that was accounted for in supply discussions. Pharmac
ACT
acknowledged the possible constraint in the future due to increased demand, which would be
discussed with Eli Lily; currently supply is satisfactory.
•
A member raised a recent publication in the NEJM regarding monoclonal antibodies and BA.2 The
study showed a reduction in activity for sotrovimab against BA.2 and that imdevimab retained
some activity against BA.2. There was discussion around the two components of Ronapreve,
including whether further evidence may suggest dosage changes in the future and STA noted
awareness of this study. It was suggested that STA investigate further, given the current outbreak
in Aotearoa New Zealand is dominated by BA.2 and Ronapreve is not being used in NZ for
Omicron on the basis of existing evidence.
INFORMATION
Action: STA to report on emerging evidence on casirivimab and imdevimab and BA.2 and any
developments arising from the NEJM paper.
Medsafe Update
•
Paxlovid has been approved under section 23 of the Medicines Act with conditions on 2 March 2022.
OFFICIAL
•
Remdesivir - Medsafe is waiting on a response to a request for information regarding remdesivir, sent
to the company in January.
•
Molnupiravir - Medsafe has sent a request for information to Merck regarding molnupiravir and are
THE
expecting a response next week.
•
Medsafe wil be having pre-submission meetings with GSK (sotrovimab) and Novartis (ensovibep
) to
discuss information required and facilitating the approval process.
UNDER
Airfinity/STA Update
‘
Highlights of Airfinity report 04 March 2022’ was circulated with the agenda for noting. A selection of key
updates was provided, including the FDA recommendation for doubling of Evusheld dose to 300mg, the
baricitinib RECOVERY trial results and emerging studies regarding Paxlovid and molnupiravir retaining
efficacy against BA.2.
Equity Considerations
3.0
RELEASED
•
A member provided feedback from Primary Care that the ‘Clinical management of COVID-19 in
hospitalised adults’ guideline is useful and the recent formatting updates are helpful, particularly
regarding decisions around remdesivir.
Document 6
• A member noted that their DHB was trial ing remdesivir IV in the community in a patient who has
comorbidities. Members discussed the challenges of identifying people at high risk for treatment in
the community, especial y people who are not currently engaged with the health system.
• Members also discussed the information circulated about the upcoming workshop, ‘Te Tiriti-based
futures + anti-racism’. It was noted that there were several different speakers and topics across
different days that may be of interest to the group.
Operational considerations for Paxlovid use in primary care – update
4.0
• A representative from the COVID Care in the Community team provided an update.
• Paxlovid has been approved by Medsafe and 60,000 doses are expected to arrive in the country
1982
with first shipment in early April. The Therapeutics Implementation Group is in the final stages of
developing an implementation plan to operationalise this, focusing on equitable distribution.
ACT
• One of the key recommendations wil be having one wholesaler for oversight. Stock will be
distributed through nominated community pharmacies.
• Nominated community pharmacies wil be determined locally by DHBs and hubs, as it is
acknowledged that local regions have greater awareness of community needs and populations at
high risk. Usual pharmacy purchasing and claiming of medicines processes will not apply so there
is greater control of distribution.
• Prescribing guidance wil be supported by Matui (He Ako Hiringa) – as noted in the section below.
Guidance wil have clear prescribing and dispensing information to advise people how to safely
take the medication.
INFORMATION
• Guidance wil also be distributed via the Health Pathways website for GPs, so there is point of care
information and national y consistent pathways.
• The COVID Care in the Community team is in discussion with Digital teams within the Ministry to
ensure that systems provide a col aborative platform for Care in the Community management.
• It is understood that Pharmac is utilising xPharm to allow for flexible stock management.
• The Therapeutics Implementation Group is exploring options for auditing and monitoring
OFFICIAL
distribution and are focusing on timely access to medications for those who are at greatest need.
Discussion
THE
• A member raised a question about the xPharm process and how that wil connect with Māori and
Pacific providers. It was noted that the nominated community pharmacies in each area will be
working closely with iwi and Māori providers. Providers wil assist with options such as pick up or
delivery of treatments when needed due to isolation requirements.
• A member raised a question regarding Paxlovid drug interactions and how these wil be addressed
UNDER
when operating in this new model, diverging from the ‘usual’ process of prescribing and
dispensing. The Therapeutics Implementation Group is discussing this and would prefer that
where possible, the person’s normal pharmacist is able to be engaged in a medication review.
However, it is noted that this could be difficult when someone is engaging at a different pharmacy
than usual. It was noted that prescribers wil have access to clinical information to assist with
providing advice around taking the treatment and any required adjustments to other medications.
There are challenges in ensuring both a simple process for timely distribution and a trusted
process to provide equitable outcomes. Further discussion is needed.
RELEASED
• A member raised a question regarding the process from a person testing positive on a rapid
antigen test (RAT) to receiving a treatment in a timely manner, given the limited treatment window.
It was outlined that the Care in the Community model was designed with this in mind. The positive
result is uploaded, triggering a notification to GP and the contact tracing system. Local
Document 6
coordination hubs have visibility of this, and the risk stratification process occurs simultaneously to
triage people into the active management stream. High risk people are proactively identified and
prioritised in the cal ing schedule. The risk stratification tool is not a clinical assessment but assists
in prioritising who is likely to need support and so should be contacted first. There is continuous
improvement to ensure the most at risk are being picked up by the system. When the treatments
are available, the GP wil become aware of the need for a prescription through the above process.
• While covering the COVID Care in the Community model, members discussed the current
situation with remdesivir, in that eligibility is significantly greater than available supply which
creates challenges for Primary Care. Members discussed that further advice on determining who
to prescribe to would be appreciated by the sector to support navigation of this challenge. Further
data on who is at the highest risk is required; members discussed the possibility of gaining insights
1982
from data from the current outbreak but agreed that action was needed before that would be
available.
ACT
Action: Therapeutics TAG to develop clinical advice on remdesivir use to help guide patient selection for
treatment.in the community. This is considered by the group as an urgent priority.
• Members discussed the need for providing advance notice to people about their eligibility for and
benefits of accessing a treatment, targeted to those who are likely to need it most.
• Members discussed whether the remdesivir access criteria could include people who have a
negative RAT but are symptomatic in a household with positive COVID-19 cases. It was noted that
‘probable’ is listed in the criteria, however such cases would not be picked up by the electronic
system at this stage, so it is challenging to provide them with rapid access to the treatment.
INFORMATION
Resource development update
• A brief document ‘Update from Pharmac Implementation team 9.3.22 – Guidance on Paxlovid
resource’ which outlines an approach to develop Paxlovid guidance to support prescribers in the
community was circulated to members on 10 March 2022 to inform discussion.
OFFICIAL
• The document outlines the current approach of focusing on awareness and management of the
drug-drug interaction potential of Paxlovid and wil be adapted from an international resource for a
New Zealand context and audience. Publication of this resource is anticipated by 1 April 2022,
with the support of Matui (He Ako Hiringa). Updates on the timeframe for final delivery wil be
THE
provided.
Guideline Updates
5.0
• The most recent ‘Clinical management of COVID-19 in hospitalised adults’ guideline was
published on 4 March 2022. Many changes were made in the recent update, including the removal
UNDER
of Ronapreve due to the displacement of Delta by Omicron and updated remdesivir access
criteria. Members discussed the need for further data to support advice around determining high
risk individuals and it was noted that finding people who require early treatment needs to be
strongly linked to testing.
• Members discussed a draft infographic that col ated information from the tables and put together
criteria for the severity categories alongside the therapeutic options. The infographic is a simplified
approach, intended as a reference figure in the document. It does not contain dosing or
RELEASED contraindications, which wil remain in the main body of the document.
• There is an ongoing conversation with the Ministry communications team regarding capacity for
design and updates of an infographic of this nature. It was noted that the graphic would require an
expert reviewer before it was published to ensure clinical accuracy if it were to be updated by other

Document 6
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED

Document 6
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED

Document 7
COVID-19 Therapeutics Technical Advisory Group
MINUTES: Te Rōpū Haumanu Kowheori-19
Date:
Friday 25 March 2022
Time:
1:30pm to 2:30pm
1982
s9(2)(k)
Location:
ACT
Chair:
Nigel Raymond
Members:
Chris Hopkins, Colin McArthur, Eamon Duffy, Elaine Yap, Jessica Keepa, Michael Maze,
Susan Morpeth, Tim Cutfield
Attendees:
Andrew Oliver, Anne Buckley, Daniel Bernal, Derek Fitzgerald, Justine Lancaster, Josh
Wiles, Ian Town, Mark Ayson
INFORMATION
Guests:
Therese Egan, James Entwisle, Brooke Hol ingshead
Apologies:
Phoebe Currie, Saleimoa Sami, Andi Shirtcliffe
1.0
Welcome and Accept Previous Minutes
Dr Nigel Raymond welcomed al members and attendees in his capacity as Chair of the COVID-19
OFFICIAL
Therapeutics Technical Advisory Group.
Minutes of the last meeting (11 March 2022) were accepted.
THE
2.0
Therapeutics
PHARMAC Update:
•
Pharmac has updated its website for the portfolio on COVID treatments including availability,
access criteria, clinical advice, and published guidance.
UNDER
•
s 9(2)(b)(ii)
•
Antivirals access criteria are being drafted based on feedback received in response to the
consultation which closed on 2 May 2022. Pharmac is aiming to have this finalised in the week
commencing 28 March 2022.
•
Paxlovid and molnupiravir wil be listed on the Pharmaceutical Schedule from 1 April 2022. Stock
RELEASED won’t be available from that date but, the treatments are being listed it in anticipation of one or
both treatments being available at some point during April.
•
s 9(2)(b)(ii)
Document 7
• s 9(2)(b)(ii)
• Remdesivir: stock remains available. Additional stock is expected to arrive in New Zealand in the
week commencing 28 March 2022.
• Pharmac is working with Roche to manage supply and stock of Tocilizumab in NZ
• s 9(2)(b)(ii)
Discussion:
A member noted there are shortages of supply of Paxlovid in the United States currently.
PHARMAC acknowledged this but noted this is not expected to affect NZ’s supply. There is the ability to
order more stock as needed and Pfizer has not communicated any issues with stock availability.
1982
Medsafe Update:
• Have met with GSK (sotrovimab) and Novartis (ensovibep)
ACT
• Sotrovimab: expecting an abbreviated application by end April
• s 9(2)(b)(ii)
• Evusheld: Medsafe is expecting an application from AstraZeneca late March/early April. Company
has indicated it wil be an abbreviated application.
• Molnupiravir (Lagevrio): Medsafe received additional information from sponsor on 18 March
however there are stil unresolved issues.
Discussion:
A Member noted the actions of Therapeutics TAG wil be scrutinised. People are dying of COVID; there is
need to put emphasis on the urgency of supply for NZ.
INFORMATION
Both PHARMAC and Medsafe agree with comment and are acutely aware of time sensitivity. Reassured
the group that they are working to get supply into the country as soon as possible.
Airfinity/STA Update
• Key slides for drugs of interest have circulated around members – the key thing to note from this is
the global supply shortage with Paxlovid however supply looks OK for NZ.
•
Excerpt taken from ‘Science and Technical Advisory V
OFFICIAL
ariants Update, 15 March 2022: This
document brings in data from neutralisation studies on casirivimab and imdevimab (Ronapreve)
suggesting possible future use for BA.2. This is from the New England Journal of Medicine
(NEJM).
THE
Discussion:
A member noted the group needs to be mindful of the NEJM article. There is no evidence to suggest
neutralising activity for BA.2. The article appears vague, conclusions drawn from this require more careful
consideration before sharing.
UNDER
3.0
Equity Considerations
• Some technology issues with people learning how to log a RAT test result. Issues arising with
patients not knowing how to log their test results.
• Some RAT tests are returning false negative tests early in the il ness meaning some patients who
are eligible for Oral medication are missing out due to the 5-day window.
• Budesonide stock is available local y however breakdown in communication has occurred; GPs
being told not to prescribe this due to low stock.
RELEASED
• It was noted Māori now have the highest COVID case rates, overtaking Pacific Peoples. This
needs to be front of mind with guidelines, prioritising Māori and Pacific peoples when there is a
limited supply.
Document 7
• Rural communities that are prone to geographical isolation (from flooding etc.) need thought into
how supply is maintained and managed.
Action: Feedback to digital team re usability and availability of different instructions for logging RAT results
specifically around having an instructional video available.
4.0
Remdesivir Community Guidance
• Community advice became available yesterday.
• Group sees the need for external guidance prioritising risk.
• Information for this is largely sourced from overseas, data from NZ is only becoming available
now. This wil be used to prioritise medications coming into the country as well as learning who is
1982
high risk. Becoming progressively important to look at different subgroups with Māori being
recognised as falling behind in health outcomes.
ACT
5.0
Budesonide – Possible Update
• This has been brought up for discussion due to concern for supply. It was noted that the issue was
more likely an issue with distribution and not supply.
• Issues were noted with time constraints teaching patients to use a new inhaler device. Not always
practical for non-English speakers or those who don’t have internet access. With a limited
workforce there are large time constraints, therefore there needs to be consideration of the
practical benefit of use for those who are low risk.
• It was noted by a member there was a lack of evidence for use of inhaled budesonide against
Omicron in the general population. It was recommended to reduce the access criteria and target
those at high risk of hospitalisation and/or partially/not vaccinated individuals.
INFORMATION
• A member noted that remdesivir and antivirals should be prioritised before budesonide for
practicality and budesonide would be better suited to prescribe if a patient was to miss the window
for antivirals/intravenous medications.
• Noted it would be helpful for clinicians to have a clear set of criteria for prioritisation. Medications
need a clear priority order. A risk table and guidelines for clinicians would be useful especially
when oral medications arrive. It was mentioned a heat map would be useful and include ethnicity,
vaccination status and age. OFFICIAL
• It was noted that once the access criteria are updated, the position statement should be updated
from the original guidance to reflect the changes and their rationale.
Actions: Elaine to revise the Position Statement on Budesonide Use and send to members.
THE
6.0
Nirmatrelvir/Ritonavir (Paxlovid)
•
Approach for Therapeutics TAG advice
A member noted Therapeutics TAG was not only for hospital guidance. Suggested the sub-group for more
community focussed guidelines
UNDER and include community guidelines into physical statements. There wil be
further work between the Ministry and PHARMAC for clinical access and guidelines.
Need national subject expertise to guide content for the national health pathways. Therapeutics TAG is a
good place for this.
Therapeutic TAG is interested to move towards integrated community guidance. In the short-term
Therapeutics TAG is to support resources being developed elsewhere for Paxlovid. Making sure the
information being produced is consistent and reflects consensus of health pathways.
RELEASED
•
Update - Information for public (eg. Health Navigator)
Health navigator currently creating information for consumers around Paxlovid. Health Navigator is asking
for expert advice on content.

Document 7
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED

Document 7
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED

Document 7
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED

Document 7
1982
ACT
INFORMATION
OFFICIAL
THE
UNDER
RELEASED
Document Outline
- H202204655 Harold Binder Docs for release_Redacted.pdf