
4 February 2022
Andrew McGregor
E: [email address]; fyi-request-17708-
[email address]; [email address]; fyi-request-17710-
[email address]
Dear Andrew
Official information request W21-695
I refer to your official information request received by the Ministry of Health on 25
November 2021, transferred to this DHB on 9 December 2021.
Request:
1:
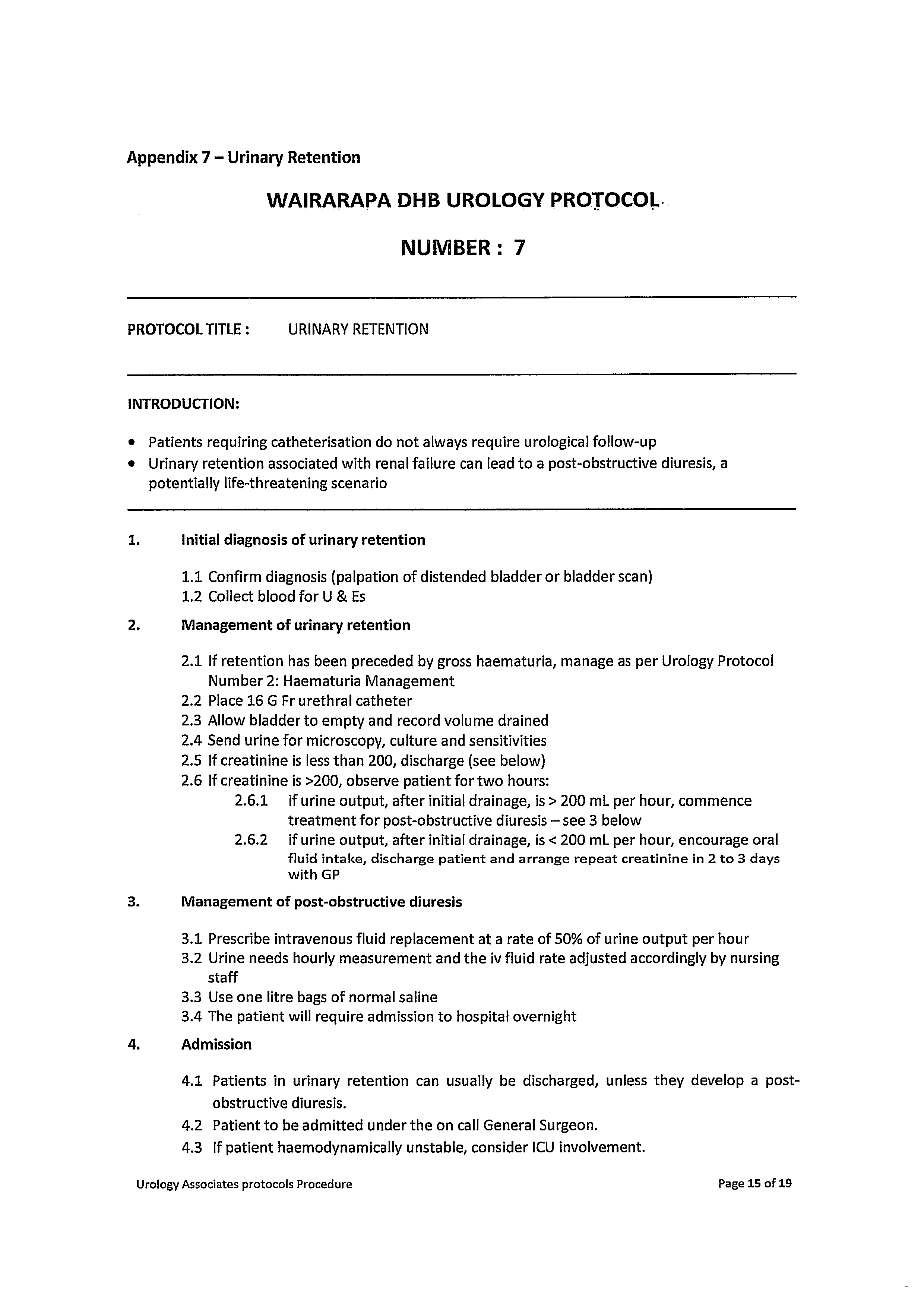
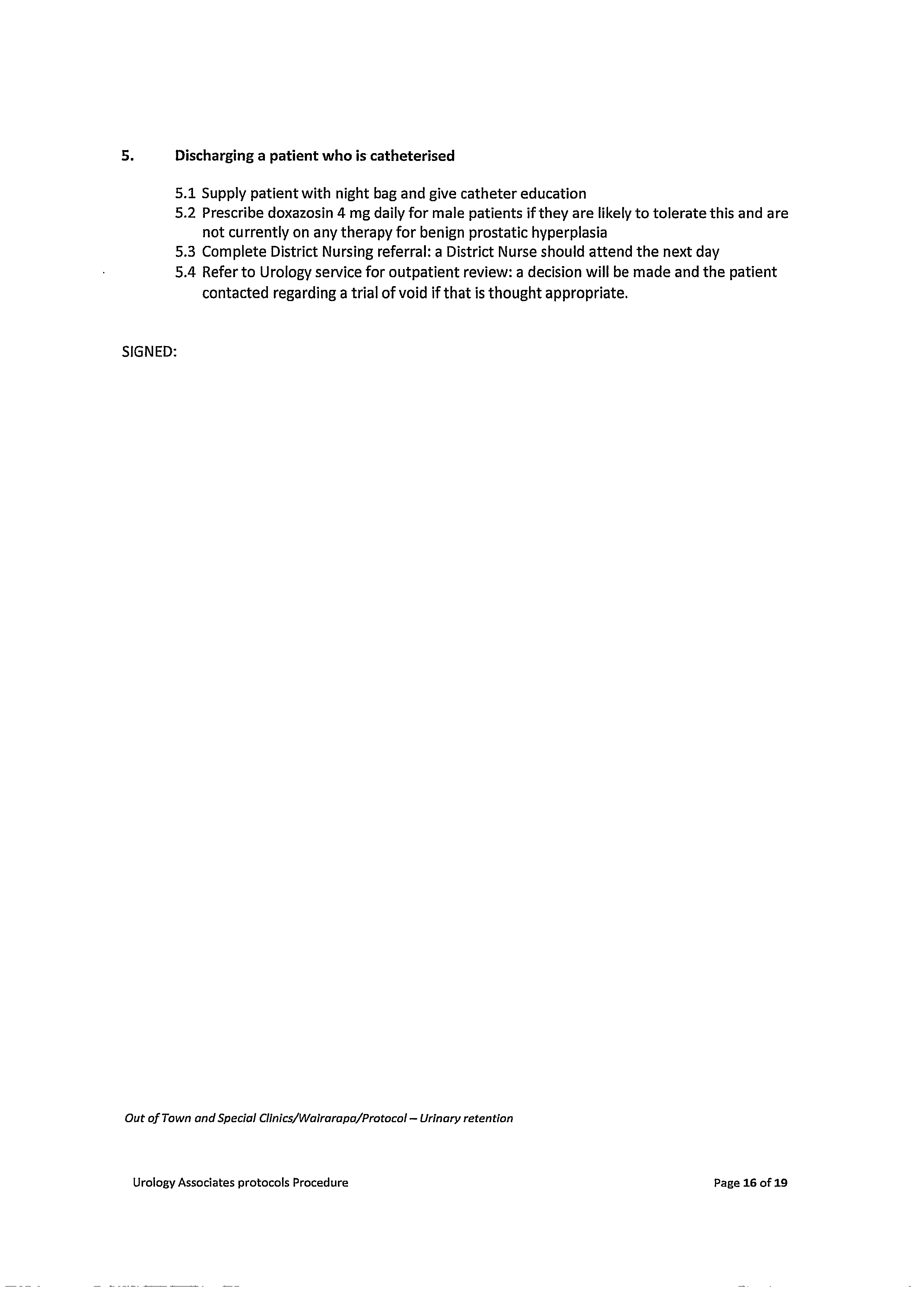
“Please provide Guidelines/Procedures for the management of postoperative Urinary
Retention (POUR)”
2:
"Please provide Guidelines/procedure for the management/prevention of persistent
Postsurgical Pain”
3:
“Please provide Guidelines/procedure in the treatment of patients after a suicide attempt
and/or suicidal ideation”
4:
“Please provide Guidelines/procedure differentiating subtypes of primary (idiopathic)
constipation”
Response:
The information you have requested is below.
1:
Please see attached “Urology Associates Protocols Procedure” Protocol 7
2:
Please see attached “Patient Controlled Analgesia Guideline” & “Lippincott
Procedures – Pain Management”
3:
Mental Health, Addiction and Intellectual Disability Service (MHAIDS) are provided
at Wairarapa DHB by Capital and Coast DHB, they will answer this question as part
of their response to your request.
4:
Please see attached “Lippincott Procedures – Constipation management,
oncology”

You have the right, under section 28 of the OIA, to seek an investigation and review by the
Ombudsman of this decision. Information about how to make a complaint is available at
www.ombudsman.parliament.nz or freephone 0800 802 602.
Please note that this response, or an edited version of this response, may be published on the
Wairarapa District Health Board website no less than one week after the response has been provided
to you. Any personal or identifying information will be redacted from any response published online.
The DHB will endeavour to resolve any concerns you should raise but, subject to any legal grounds for
withholding, ultimately reserves the right to publish any information.
If you wish to discuss this response with us, please feel free to contact:
OIA Coordinator
Email: [email address]
Ph: 06 946 9800
Yours sincerely
Dale Oliff
Chief Executive



11/01/2022
Lippincott Procedures - Pain management
This website uses cookies to improve the functionality and performance of this website. See our Privacy and Cookie policy for more information.
By continuing to use this website you are giving consent to cookies being used.
Continue
Pain management
Introduction
Pain, considered the fifth vital sign, is defined by the International Association for the Study of Pain as the sensory and
emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Thus, pain
includes not only the perception of an uncomfortable stimulus, but also the response to that perception.
The patient's self-report of pain is the most reliable indicator of the existence of pain. When a patient feels severe pain, he
seeks medical help because he believes the pain signals a serious problem. This perception produces anxiety, which, in turn,
increases the pain. To assess and manage pain properly, the nurse must depend on the patient's subjective description in
addition to objective tools, and any relevant pain history from which to make a comparison.
According to The Joint Commission, health care facilities are required to develop policies and procedures supporting the
appropriate use of analgesics and other pain control therapies. Pain should be assessed at admission and be reassessed at
regular intervals. Pain assessment should include personal, cultural, spiritual, and ethnic beliefs. Patients and families should
be educated about their role in pain management. They should also be informed about potential limitations and adverse
effects of pain treatment.
Several interventions can be used to manage pain, including analgesics, emotional support, comfort measures, and
complementary and alternative therapies such as cognitive techniques to distract the patient. The Analgesic Ladder provides a
useful stepped approach to the use of analgesics and adjuvants. Mild pain can be treated with non-opioids such as aspirin or
paracetomol, while more severe pain responds to strong opioids such as morphine. Acute severe pain is best treated using the
intravenous route in order to effectively titrate pain relief.
Invasive measures, such as epidural analgesia or patient-controlled analgesia (PCA), may also be required.
Equipment
Pain assessment tool or scale
Implementation
Perform hand hygiene.
Assess the patient's pain by using a pain assessment tool or scale or by asking key questions and noting his response to
the pain. For instance, ask him to describe its duration, severity, and location. Look for physiologic or behavioral clues to
the pain's severity.(See below How to assess pain.)
Establish with the patient what a low pain level means. Generally, this number is no more than 4 on the 0-10 scale.
Work with the patient to develop a nursing care plan using interventions appropriate to the patient's lifestyle. These may
include prescribed medications, emotional support, comfort measures, complementary and alternative therapies such as
cognitive techniques, and education about pain and its management. Emphasize the importance of maintaining good
bowel habits, respiratory functions, and mobility because pain may exacerbate any problems in these areas.
Explain to the patient how pain medications work together with other pain management therapies to provide relief. Also
explain that management aims to keep pain at a low level to permit optimal bodily function.
Implement your care plan. Because individuals respond to pain differently, you'll find that what works for one person
may not work for another.
HOW TO ASSESS PAIN
To assess pain effectively, you'll need to consider the patient's abilitiy to understand and communicate, depending on age,
cognitive ability and preferred language. As part of the pain assessment you will need to consider the patient's description of
the pain as well as observations of behavioural responses and physical functioning. Start by asking this series of key
questions (bearing in mind that the patient's responses will be shaped by his prior experiences, self-image, and beliefs about
his condition):
Onset and duration. "When did the pain start?"
Provokes or relieves. "What makes the pain worse, or better?"
Quality or character. "Describe the pain."
https://procedures.lww.com/lnp/view.do?pId=729475&disciplineId=493
1/5
11/01/2022
Lippincott Procedures - Pain management
Region(s)/Radiate. "Where is the pain?"
Severity/intensity. "How sore are you at rest? On movement?"
Timing. "Is the pain constant, or intermittant?" Is the pain associated with other symptoms such as nausea, vomiting,
diarrhoea?
Understand response. "What do you think or feel about this pain?" "What are your expectations for treating this pain?"
Ask the patient to rank the severity and intensity of his pain, using an age cognitively appropriate and language sensitive tool
or scale of 0 to 10 (Numerical Pain Scale), with 0 denoting no pain and 10 denoting the worst pain level ever. This rating
helps the patient verbally evaluate pain therapies. It is important to assess pain both when the patient is resting and when
he is active.
Features in the pain history might might suggest the presence of neuropathic pain. Please link to WDHB's IPS Handbook p.
100-102 for more on this.
Assess the pain regularly throughout the day, especially before and after giving analgesia, and through the night (when pain
is usually heightened). Keep in mind that the ability to sleep doesn't indicate absence of pain.
Observe the patient's behavioral and physiologic responses to pain. Physiologic responses may be sympathetic or
parasympathetic, but remember the absence of physiologic responses doesn't mean an absence of pain.
Behavioral responses
These include altered body position, moaning, sighing, grimacing, withdrawal, crying, restlessness, muscle twitching, and
immobility.
Scales such as PAINAD (The Pain Assessment Checklist for Seniors with Limited Ability to Communicate) and, CNPI (Checklist
of Nonverbal Pain Indicators) are behavioural tools for use in the assessment of pain in older adults with communication
difficulties secondary to cognitive impairment/dementia. Link to WDHB IPS Handbook Appendix VI.
Sympathetic responses
These are commonly associated with mild to moderate pain and include pallor, elevated blood pressure, dilated pupils,
skeletal muscle tension, dyspnea, tachycardia, and diaphoresis.
Parasympathetic responses
These are commonly associated with severe, deep pain and include pallor, decreased blood pressure, bradycardia, nausea
and vomiting, weakness, dizziness, and loss of consciousness.
Giving medications
Before administering and pain relief, confirm the patient's identity using at least two patient identifiers according to your
facility's policy.
If the patient is allowed oral intake, begin with a nonopioid analgesic, such as paracetamol, every 4 to 6 hours as
ordered.
If the patient needs more relief than a nonopioid analgesic provides, you may want to consider giving a mild opioid such
as codeine or tramadol as ordered, or a strong opioid such as morphine as prescribed. Administer oral medications if
possible. Check the appropriate drug information for each medication given. There are many other adjuvant drugs which
may improve pain management and could be worth considering e.g. amitriptylline for neuropathic pain.
If ordered, teach the patient how to use a Patient-controlled analgesia (PCA) device. Such a device can help the patient
manage his pain and decrease his anxiety. (See the "
Patient-controlled analgesia" procedure.)
Assess pain according to your facility's guidelines after parenteral medication administration. Following oral medication
administration assess pain within 60 minutes. If the patient is still in pain, reassess him and alter your care plan as
appropriate, and consider asking for medical assistance.
Providing emotional support
Pain can cause or exacerbate anxiety. Show your concern by spending time talking with the patient. Discuss the patient's
concerns if he is frustrated or anxious about his pain and provide clear information about pain management.
Performing comfort measures
Reposition the patient periodically to reduce muscle spasms and tension and to relieve pressure on bony prominences.
Increasing the angle of the bed can reduce pull on an abdominal incision, diminishing pain. If appropriate, elevate a limb
to reduce swelling, inflammation, and pain.
Splinting or supporting abdominal and chest incisions with a pillow when coughing or changing position helps decrease
pain.
Apply cold compresses, as appropriate, to decrease discomfort.
Give the patient a back massage to help reduce tense muscles.
https://procedures.lww.com/lnp/view.do?pId=729475&disciplineId=493
2/5

11/01/2022
Lippincott Procedures - Pain management
Perform passive range-of-motion exercises to prevent stiffness and further loss of mobility, relax tense muscles, and
provide comfort.
Provide oral hygiene. Keep a fresh water glass or cup at the bedside because many pain medications tend to dry the
mouth.
Wash the patient's face and hands to soothe the patient, which may reduce his perception of pain.
Using complementary and alternative therapies such as cognitive therapy
Help the patient enhance the effect of analgesics by using such techniques as distraction, guided imagery, deep
breathing, and relaxation.You can easily use these "mind-over-pain" techniques at the bedside. Choose the method the
patient prefers. If possible, start these techniques when the patient feels little or no pain. If he feels persistent pain,
begin with short, simple exercises. Before beginning, dim the lights, remove the patient's restrictive clothing, and
eliminate noise from the environment.
For distraction, have the patient recall a pleasant experience or focus his attention on an enjoyable activity. For instance,
have him use music as a distraction by turning on the radio when the pain begins. Have him close his eyes and
concentrate on listening, raising or lowering the volume as his pain increases or subsides. Note, however, that distraction
is usually helpful in relieving pain lasting for brief episodes or for painful procedures of short duration.
For imagery, help the patient concentrate on a peaceful, pleasant image, such as walking on the beach. Encourage him
to concentrate on the details of the image he has selected by asking about its sight, sound, smell, taste, and touch. The
positive emotions evoked by this exercise minimize pain.
For deep breathing, have the patient stare at an object, then slowly inhale and exhale as he counts aloud to maintain a
comfortable rate and rhythm. Have him concentrate on the rise and fall of his abdomen. Encourage him to feel more and
more weightless with each breath while he concentrates on the rhythm of his breathing or on any restful image.
For muscle relaxation, have the patient focus on a particular muscle group. Then ask him to tense the muscles and note
the sensation. After 5 to 7 seconds, tell him to relax the muscles and concentrate on the relaxed state. Have him note
the difference between the tense and relaxed states. After he tenses and relaxes one muscle group, have him proceed to
another and another until he's covered his entire body.
Special Considerations
During periods of intense pain, the patient's ability to concentrate diminishes. If your patient is in severe pain, help him
to select a cognitive technique that's easy to use. After he selects a technique, encourage him to use it consistently.
Remind the patient that results of cognitive therapy techniques improve with practice. Help him through the initial
sessions.
Pain shouldn't be considered a normal part of the aging process. Provide pain relief for the elderly patient using
pharmacologic and nonpharmacologic approaches. Remember, safety is a special concern, especially the risk for falls due
to impaired mobility from pain and from adverse effects from pain medications.
It's important to identify age-related factors that affect assessment and pain management in elderly patients. For
instance does the elderly patient have cognitive impairment?
Remember too that elderly patients may have a number of medical conditions for which they are being treated. he
addition of pain medications may increase the risk of adverse effects due to drug interactions.
Evaluate your patient's response to pain management. If he's still in pain, reassess him and alter your care plan as
appropriate.
Culture and beliefs affect behavioral responses to pain and treatment preferences. Therefore, you must take into account
the patient's expectations regarding pain relief when developing the care plan.
Patients receiving opioid analgesics may be at risk for developing tolerance, dependence, or addiction. However, studies
have demonstrated that addiction during acute pain treatment is less than one percent.
Addiction is defined as psychological dependence characterized by a persistent pattern of dysfunctional drug use. The
patient's behavior will be characterized by a craving for the drug to experience effects other than pain relief. A patient
demonstrating such behavior usually has a pre-existing problem that's exacerbated by the opioid use.Discuss the
addicted patient's problem with supportive personnel, and make appropriate referrals to experts.
Physical dependence is a physiologic state in which withdrawal symptoms occur with abrupt cessation or reversal of the
drug. Physical dependence doesn't mean that addiction coexists. Symptoms include anxiety, irritability, chills and hot
flashes, excessive salivation and tearing, rhinorrhea, sweating, nausea, vomiting, and seizures. These signs and
symptoms are likely to begin within 6 to 12 hours and peak within 24 to 72 hours of discontinuing the drug. To reduce
the risk of dependence, discontinue an opioid by decreasing the dose gradually each day. You may also switch to an oral
opioid and decrease its dose gradually.
Tolerance is a neuro-adaptive response that results in a decrease to one or more of the effects of the drug over time,
such as decreased analgesia or sedation. Tolerance doesn't mean that addiction coexists.
If your patient has dementia or some other cognitive impairment, don't assume that he can't understand the pain scale
or communicate about his pain. Experiment with several pain scales. A scale featuring faces, such as the Wong-Baker
FACES scale or the Faces Pain Scale - are both good choices for many cognitively impaired patients and those with
limited language skills. (See
Visual pain rating scale.)
VISUAL PAIN RATING SCALE
https://procedures.lww.com/lnp/view.do?pId=729475&disciplineId=493
3/5





11/01/2022
Lippincott Procedures - Pain management
You can evaluate pain in a nonverbal manner for pediatric patients age 3 and older and for adults with language difficulties.
One instrument is the Wong-Baker FACES pain rating scale; another, two simple faces such as the ones shown below. Ask
the patient to choose the face that describes how he's feeling — either happy because he has no pain, or sad because he has
some or a lot of pain. Alternatively, to pinpoint varying levels of pain, you can ask the patient to draw a face.
Hockenberry, M.J., et al. Wong's Essentials of Pediatric Nursing, 7th ed. St. Louis: Mosby, Inc., 2005. Reprinted with
permission.
Complications
The most common adverse effects of opioid analgesics include sedation, constipation, nausea, vomiting and itch. Respiratory
depression, the most serious happens less commonly though is much feared.
Documentation
Document each step of the nursing process. Describe the subjective information you elicited from the patient, using his own
words. Note the location, quality, and duration of the pain as well any precipitating factors.
Record your nursing diagnoses; include the pain-relief method selected and the patient's rating of the pain before and after
pain management interventions. Use a flow sheet to document pain assessment findings. Summarize your actions including
the name and dosage of any medication given, and the patient's response. If the patient's pain wasn't relieved, note
alternative treatments to consider the next time pain occurs. Also record any complications of drug therapy.
References
1. American Society of Anesthesiologists Task Force on Chronic Pain Management and American Society of Regional
Anesthesia and Pain Medicine. "Practice Guidelines for Chronic Pain Management: An Updated Report," Anesthesiology
112(4):810-33, April 2010.
2. American Society of PeriAnesthesia Nurses (August 1, 2003). "ASPAN Pain and Comfort Clinical Guideline," [Online].
Available:
http://www.aspan.org/Portals/6/docs/ClinicalPractice/Guidelines/ASPAN_ClinicalGuideline_PainComfort.pdf
[June 2011].
3. Costantini, R., et al. "Controlling Pain in the Post-Operative Setting," International Journal of Clinical Pharmacology and
Therapeutics 49(2):116-127, February 2011.
4. Courtenay, M., and Carey, N. "The Impact and Effectiveness of Nurse-Led Care in the Management of Acute and Chronic
Pain: A Review of the Literature," Journal of Clinical Nursing 17(15):2001-2013, August 2008.
5. Fine, P.G., et al. "Long-Acting Opioids and Short-Acting Opioids: Appropriate Use in Chronic Pain Management," Pain
Medicine 10 Suppl 2:S79-88, July 2009.
6. Helfand, M., and Freeman, M. "Assessment and Management of Acute Pain in Adult Medical Inpatients: A Systematic
Review," Pain Medicine 10(7):1183-99, October 2009.
7. Institute for Clinical Systems Improvement (ICSI). Assessment and Management of Acute Pain. Bloomington, Minn.: ICSI,
2006.
8. Institute for Clinical Systems Improvement (ICSI). Assessment and Management of Chronic Pain. Bloomington, Minn.:
ICSI, 2005.
9. The Joint Commission. Comprehensive Accreditation Manual for Hospitals: The Official Handbook. Standard
NPSG.01.01.01. Oakbrook Terrace, Ill.: The Joint Commission, 2012. (Level I)
10. The Joint Commission. Comprehensive Accreditation Manual for Hospitals: The Official Handbook. Standard
NPSG.07.01.01. Oakbrook Terrace, Ill.: The Joint Commission, 2012. (Level I)
11. The Joint Commission. Comprehensive Accreditation Manual for Hospitals: The Official Handbook. Standard PC.01.02.07.
Oakbrook Terrace, Ill.: The Joint Commission, 2012. (Level I)
https://procedures.lww.com/lnp/view.do?pId=729475&disciplineId=493
4/5
11/01/2022
Lippincott Procedures - Pain management
12. The Joint Commission. Comprehensive Accreditation Manual for Hospitals: The Official Handbook. Standard PC.02.03.01.
Oakbrook Terrace, Ill.: The Joint Commission, 2012. (Level I)
13. Kelly, R.B. "Acupuncture for Pain," American Family Physician 80(5):481-84, September 2009.
14. Martell, B.A., et al. "Systematic Review: Opioid Treatment for Chronic Back Pain: Prevalence, Efficacy, and Association
with Addiction," Annals of Internal Medicine 146(2):116-27, January 16, 2007.
15. Macintyre, P., Scott, D., Schug, S., Visser, E., & Walker S. (Eds.) Acute Pain Management: Scientific Evidence. Third
Edition 2010. ANZCA.
16. Nwokeji, E.D., et al. "Influences of Attitudes on Family Physicians' Willingness to Prescribe Long-Acting Opioid Analgesics
for Patients with Chronic Nonmalignant Pain," Clinical Therapeutics 29 Suppl:2589-2602, 2007.
17. Samuels, J.G., and Fetzer, S.J. "Evidence-Based Pain Management: Analyzing the Practice Environment and Clinical
Expertise," Clinical Nurse Specialist 23(5):245-51, September-October 2009.
18. World Health Organization (2010). "WHO's Pain Relief Ladder," [Online]. Available:
http://www.who.int/cancer/palliative/painladder/en [July 14, 2010].
IP Address: 202.20.63.252, Server: AUSE1PLNSWEB2.WKRainier.com, Session: D686CAEEDDF32B7DC085216D13B0292E
©2022 Wolters Kluwer Health, Inc. and/or its subsidiaries. All rights reserved.
License Agreement & Disclaimer Privacy Statement
https://procedures.lww.com/lnp/view.do?pId=729475&disciplineId=493
5/5

04/02/2022
Lippincott Procedures - Constipation management, oncology
This website uses cookies to improve the functionality and performance of this website. See our
Privacy and Cookie policy for more
information.
By continuing to use this website you are giving consent to cookies being used.
Continue
Constipation management, oncology
Revised: November 19, 2021
Introduction
Constipation is the decreased passage of stool characterized by infrequent bowel movements, hard stool, the sensation
of abdominal bloating or cramping, straining with bowel movements, and the feeling of incomplete evacuation. 1 It
may be a symptom of cancer, an adverse effect of treatment, or the result of tumor progression. 2 Constipation may be
accompanied by abdominal discomfort, abdominal distention, anorexia, and headache. 3
Factors that increase a patient's risk of constipation include mechanical pressure on the bowel (caused by ascites, a
tumor, or an obstruction), spinal cord damage, decreased mobility, dehydration, inadequate dietary fiber intake,
metabolic and endocrine disorders, use of certain medications, and laxative overuse. Constipation affects one-half of
patients with advanced cancer and most patients being treated with opioids. 1 4
Managing constipation in patients with cancer is challenging and complex because it commonly has more than one
cause. Patients also may be embarrassed to discuss the problem, so it may go unrecognized until a patient is in
distress. Prevention and early intervention are the keys to avoiding such complications as nausea, vomiting, malaise,
hemorrhoids, anal fissures, abdominal and rectal pain, paralytic ileus, and bowel obstruction and perforation, which can
occur if constipation progresses. Teaching patients about measures to prevent constipation and encouraging them to
report symptoms when they occur is essential. Various pharmacologic and nonpharmacologic interventions are available
for treating constipation. Treatment should be individualized according to the patient's history, treatment regimen, and
condition. 1
https://procedures.lww.com/lnp/view.do?pId=1440722&disciplineId=493
1/13



04/02/2022
Lippincott Procedures - Constipation management, oncology
Equipment
Prescribed medications
Vital signs monitoring equipment
Stethoscope
Disinfectant pad
Severity of constipation grading tool
Optional: bedside commode, assistive devices, gloves, gown, mask with face shield or mask and goggles, enema
administration equipment
Preparation of Equipment
Inspect all equipment and supplies. If a product is expired, is defective, or has compromised integrity, remove it from
patient use, label it as expired or defective, and report the expiration or defect as directed by your facility.
Implementation
Review the patient's medical record for cancer diagnosis, grading, and staging; treatment regimen; history of
surgical procedures; and other conditions that can increase the risk of constipation. 1
Gather and prepare the necessary equipment and supplies.
Perform hand hygiene. 5 6 7 8 9 10
Put on gloves, a gown, a mask with a face shield or a mask and goggles, as needed, to comply with standard
precautions. 11 12 13
Confirm the patient's identity using at least two patient identifiers. 14
Provide privacy. 15 16 17 18
Obtain the patient's vital signs.
Obtain a dietary history from the patient to assess fluid and fiber intake. 1
Assess the patient's GI status, including the characteristics of bowel sounds, if present. Assess for abdominal
distention, pain, and cramping. 1
https://procedures.lww.com/lnp/view.do?pId=1440722&disciplineId=493
2/13


04/02/2022
Lippincott Procedures - Constipation management, oncology
Ask the patient about elimination patterns, including the date of the last bowel movement, the frequency and
character of stools (amount, color, consistency, and presence of blood), and the use of laxatives, stool softeners,
and other measures to enhance bowel function. 1
For suspected ileus or mechanical obstruction, arrange for an abdominal X-ray as ordered. 1 4
Assist with maintaining the patient's usual bowel habits during hospitalization. 1
When the patient has the urge to defecate, provide a private, quiet, comfortable environment. Assist the patient
to the toilet or commode and provide assistive devices, if needed, because assuming an upright position facilitates
bowel evacuation. 19 Avoid using a bedpan whenever possible.
If the patient has the urge to defecate but can't pass stool, perform a digital rectal examination (unless
contraindicated) to check for a low fecal impaction. If the patient's condition allows, perform manual disimpaction
after administering an analgesic, a sedative, or both, as prescribed, following safe medication
practices. 20 21 22 23 The practitioner may also order an oil retention enema to soften hard stool. (See the "Fecal
impaction removal, digital" and "Enema administration" procedures.) 4
Clinical alert: Don't perform digital rectal examination, perform stoma manipulation, or administer suppositories or
enemas to a patient with myelosuppression because doing so can increase the risk of infection and bleeding. 1
If the patient reports nausea, vomiting, anorexia, cramping, or abdominal distention and passes liquid stool,
suspect an impaction high in the ascending or transverse colon. 1 4 Administer an oral laxative and an enema
(unless contraindicated), as needed and prescribed, following safe medication practices 20 21 22 23 to relieve the
impaction. 4
Monitor laboratory test results to detect possible causes of constipation, such as hypercalcemia, hypokalemia,
hypothyroidism, and diabetes mellitus. Treat the cause as prescribed. 4 Notify the practitioner of critical test
results within your facility's established time frame so that the patient can be treated promptly. 24
Encourage adequate fluid intake (3,000 mL of fluid per day, unless medically contraindicated). 1 Note that warm
or hot liquids may help stimulate bowel movement. Discourage the patient from drinking coffee, tea, and
grapefruit juice because they have a diuretic effect.
For a patient who has adequate fluid intake, isn't in the late stages of cancer, and doesn't have structural bowel
obstruction, encourage increasing the amount of fiber in the diet because fiber facilitates the passage of feces
through the intestines and reduces the risk of fecal impaction. 1 Advise the patient to slowly increase fiber intake
by adding 3 to 4 g/day and then increasing to 6 to 10 g/day to prevent fiber intolerance. High-fiber foods include
bran, beans, seeds, nuts, vegetables, fruits, and whole grains. 1
https://procedures.lww.com/lnp/view.do?pId=1440722&disciplineId=493
3/13
link to page 15
04/02/2022
Lippincott Procedures - Constipation management, oncology
Use mealtimes to establish a bowel routine to take advantage of the gastrocolic reflex that naturally occurs 5 to
15 minutes after eating. 19
Record the patient's bowel movements and initiate an individualized bowel management regimen if the patient
doesn't have a bowel movement for 3 days.
Administer medications, as prescribed, following safe medication administration practices. 20 21 22 23 (See
Medications used to manage constipation.)
MEDICATIONS USED TO MANAGE CONSTIPATION
Various medications can be used to manage constipation in patients with cancer. The particular agent should be
chosen based on the patient's history, condition, and therapeutic regimen.
Medication
Mechanism of action
Special considerations
Bulk-forming laxatives
Cause water retention in the stool
Must be taken with 200 to 300
(psyllium)
mL of water
May cause flatulence, abdominal
distention, bloating, mechanical
obstruction, and anaphylactic
reactions
Should be used cautiously in
patients with severe constipation
and advanced cancer
Emollient suppositories
Coat and soften stool
Can lead to perianal irritation in
(glycerin) 4
excessive doses
May be effective in relieving fecal
impaction
https://procedures.lww.com/lnp/view.do?pId=1440722&disciplineId=493
4/13
04/02/2022
Lippincott Procedures - Constipation management, oncology
Iso-osmotic laxatives
Block water absorption from stool in the large
Are available with or without
(polyethylene glycol)
intestine, thus making stools softer
electrolytes (solution form)
Are used to treat persistent
constipation
Osmotic laxatives
Soften stool by attracting and retaining water in
Usually take effect in 24 to 72
(sorbitol, lactulose) 4
the bowel
hours
May cause abdominal pain or
cramping, flatulence, and
abdominal distention
Peripherally acting opioid Prevent opioids from binding to the mu-receptors
Are used for opioid-induced
agonists
of the GI tract, thereby relieving opioid-induced
constipation in patients with
(methylnaltrexone) 4
constipation while maintaining pain control
advanced cancer who are
receiving palliative care
Shouldn't be used in patients with
postoperative ileus or a
mechanical bowel obstruction
May cause flatulence, abdominal
pain, and nausea
Prokinetic agents
Stimulate peristalsis
Are used to combat delayed
(metoclopramide) 4
gastric emptying
Usually are taken before meals
and at bedtime
Shouldn't be used in patients with
large abdominal tumors or bowel
https://procedures.lww.com/lnp/view.do?pId=1440722&disciplineId=493
5/13
04/02/2022
Lippincott Procedures - Constipation management, oncology
obstruction
Saline laxatives (saline
Draw fluid into the gut by osmosis, which in turn
Can cause dehydration with
mixture containing
softens stool and stimulates peristalsis
repeated use
magnesium salts or
sulfate ions)
Shouldn't be used in patients who
can't tolerate fluid loss or can't
maintain adequate daily fluid
intake
Stimulant laxatives
Stimulate motility in the colon
Are used most commonly as part
(bisacodyl, senna) 4
of a prophylactic bowel regimen
May be given two or three times
per day to achieve an unforced
bowel movement every 1 to 2
days
May cause abdominal discomfort,
electrolyte imbalances,
hepatotoxicity, and allergic
reactions
Encourage the patient to exercise regularly, as tolerated, to promote GI motility. 1 4 If the patient can't exercise,
encourage an increase in physical activity, as tolerated, or provide passive exercise to promote the urge to
defecate. 1
Consult a practitioner specially trained in aromatherapy (if available at your facility) because abdominal massage
using essential oils, such as rosemary, peppermint, and lemon, may help relieve constipation. 25
If the patient receives opioids to manage pain, collaborate with the health care team about using alternative
medications to decrease constipation. For example, use an opioid agonist-opioid antagonist combination drug
(such as oxycodone and naloxone) to relieve pain with fewer constipating effects. 1 2
https://procedures.lww.com/lnp/view.do?pId=1440722&disciplineId=493
6/13
link to page 18


04/02/2022
Lippincott Procedures - Constipation management, oncology
Teach the patient abdominal exercises and diaphragmatic breathing to increase muscle tone and subsequently aid
defecation.
Remove and discard your personal protective equipment, if worn. 13
Perform hand hygiene. 5 6 7 8 9 10
Clean and disinfect your stethoscope using a disinfectant pad. 26 27
Perform hand hygiene. 5 6 7 8 9 10
Grade the severity of the patient's constipation using a facility-approved tool. (See Grading constipation severity.)
SCROLL
GRADING CONSTIPATION SEVERITY
A grading system commonly helps describe the severity of adverse events related to cancer therapy. To grade the
severity of a patient's constipation, you can use the Common Terminology Criteria for Adverse Events, developed by
the National Cancer Institute. 28 The tool provides consistent terms for adverse events that result from therapy and
consists of five grades:
Grade 1 — Occasional or intermittent symptoms require occasional use of stool softeners, laxatives, dietary
modifications, or enemas.
Grade 2 — Persistent symptoms require regular use of enemas or laxatives and limit instrumental activities of
daily living (ADLs).
Grade 3 — Obstipation requires manual evacuation and limits self-care ADLs.
Grade 4 — Life-threatening complications require urgent intervention.
Grade 5 — Death results from the adverse event.
From U.S. Department of Health and Human Services, National Institutes of Health, & National Cancer Institute.
(2017). Common terminology criteria for adverse events (CTCAE): Version 5.0. Retrieved October 2021 from
https://ctep.cancer.gov/protocolDevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_8.5x11.pdf
Document the procedure. 29 30 31 32
https://procedures.lww.com/lnp/view.do?pId=1440722&disciplineId=493
7/13
link to page 23







04/02/2022
Lippincott Procedures - Constipation management, oncology
Special Considerations
Because vinca alkaloids decrease GI motility, patients receiving these agents should use a combination laxative-
stool softener to prevent constipation. 1
Patient Teaching
Teach the patient and family (if applicable) about measures to prevent constipation, such as increasing physical activity
(as tolerated), drinking 3,000 mL of fluid per day (unless medically contraindicated), and increasing fiber intake. 1
Instruct the patient about the importance of developing a routine bowel regimen. Advise the patient to report
constipation. Teach about the complications that can occur if constipation is allowed to persist. Stress the importance of
notifying the practitioner if 3 days pass without a bowel movement. 1
Complications
Failure to manage constipation adequately may cause such complications as rectal bleeding, fluid and electrolyte
imbalances, fecal impaction, bowel obstruction or perforation, and sepsis. 1
Documentation
Document your assessment findings; the patient's intake and output, including the characteristics of any bowel
movements; and the constipation severity grade. Record your interventions and the patient's response to those
interventions. Document teaching provided to the patient and family (if applicable), their understanding of that
teaching, and any need for follow-up teaching.
Related Procedures
Confusion management, long-term care
Diarrhea management, oncology
Hypercalcemia emergency patient care, oncology
Syndrome of inappropriate antidiuretic hormone secretion, emergency patient care, oncology
References
(Rating System for the Hierarchy of Evidence for Intervention/Treatment Questions)
https://procedures.lww.com/lnp/view.do?pId=1440722&disciplineId=493
8/13
04/02/2022
Lippincott Procedures - Constipation management, oncology
1. Olsen, M. M., et al. (Eds.). (2019). Chemotherapy and immunotherapy guidelines and recommendations for
practice. Oncology Nursing Society.
2. Javi, B., & Marsicano, E. (2018). Constipation: Evaluation and management. Missouri Medicine, 115(3), 236-240.
Retrieved October 2021 from http://www.omagdigital.com/publication/?
m=&l=1&i=512824&p=62&ver=html5(Level I)
3. Lentz, J., & McMillan, S. C. (2010). The impact of opioid-induced constipation on patients near the end of life:
Perspectives of patients, family caregivers, and nurses. Journal of Hospice and Palliative Nursing, 12(1), 29–38.
Retrieved October 2021 from
https://journals.lww.com/jhpn/Fulltext/2010/01000/The_Impact_of_Opioid_Induced_Constipation_on.10.aspx(Level
VI)
4. Dans, M., et al. (2017). NCCN guidelines insights: Palliative care, version 2.2017. Journal of the National
Comprehensive Cancer Network, 15(8), 989–997. Retrieved October 2021 from
https://jnccn.org/view/journals/jnccn/15/8/article-p989.xml (Level V)
5. The Joint Commission. (2021). Standard NPSG.07.01.01. Comprehensive accreditation manual for hospitals. (Level
VII)
6. Centers for Disease Control and Prevention. (2002). Guideline for hand hygiene in health-care settings:
Recommendations of the Healthcare Infection Control Practices Advisory Committee and the
HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. MMWR Recommendations and Reports, 51(RR-16), 1–45.
Retrieved October 2021 from https://www.cdc.gov/mmwr/pdf/rr/rr5116.pdf (Level II)
7. World Health Organization (WHO). (2009). WHO guidelines on hand hygiene in health care: First global patient
safety challenge, clean care is safer care. Retrieved October 2021 from
https://apps.who.int/iris/bitstream/handle/10665/44102/9789241597906_eng.pdf?sequence=1 (Level IV)
8. Centers for Medicare and Medicaid Services. (2020). Condition of participation: Infection control. 42 C.F.R. §
482.42.
9. Accreditation Association for Hospitals and Health Systems. (2020). Standard 07.01.21. Healthcare Facilities
Accreditation Program: Accreditation requirements for acute care hospitals. (Level VII)
10. DNV GL-Healthcare USA, Inc. (2020). IC.1.SR.1. NIAHO® accreditation requirements, interpretive guidelines and
surveyor guidance – revision 20.0. (Level VII)
11. Accreditation Association for Hospitals and Health Systems. (2020). Standard 07.01.10. Healthcare Facilities
Accreditation Program: Accreditation requirements for acute care hospitals. (Level VII)
https://procedures.lww.com/lnp/view.do?pId=1440722&disciplineId=493
9/13
04/02/2022
Lippincott Procedures - Constipation management, oncology
12. Siegel, J. D., et al. (2007, revised 2019). 2007 guideline for isolation precautions: Preventing transmission of
infectious agents in healthcare settings. Retrieved October 2021 from
https://www.cdc.gov/infectioncontrol/pdf/guidelines/isolation-guidelines-H.pdf (Level II)
13. Occupational Safety and Health Administration. (2012). Bloodborne pathogens, standard number 1910.1030.
Retrieved October 2021 from https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.1030
(Level VII)
14. The Joint Commission. (2021). Standard NPSG.01.01.01. Comprehensive accreditation manual for hospitals. (Level
VII)
15. Accreditation Association for Hospitals and Health Systems. (2020). Standard 15.01.16. Healthcare Facilities
Accreditation Program: Accreditation requirements for acute care hospitals.(Level VII)
16. Centers for Medicare and Medicaid Services. (2020). Condition of participation: Patient's rights. 42 C.F.R. §
482.13(c)(1).
17. DNV GL-Healthcare USA, Inc. (2020). PR.2.SR.5. NIAHO® accreditation requirements, interpretive guidelines and
surveyor guidance – revision 20.0. (Level VII)
18. The Joint Commission. (2021). Standard RI.01.01.01. Comprehensive accreditation manual for hospitals. (Level
VII)
19. McKay, S. L., et al. (2012). Evidence-based practice guideline: Management of constipation. Journal of
Gerontological Nursing, 38(7), 9–15. Retrieved October 2021 from https://doi.org/10.3928/00989134-20120608-
01
Abstract |
Complete Reference
20. The Joint Commission. (2021). Standard MM.06.01.01. Comprehensive accreditation manual for hospitals. (Level
VII)
21. Centers for Medicare and Medicaid Services. (2020). Condition of participation: Nursing services. 42 C.F.R. §
482.23(c).
22. Accreditation Association for Hospitals and Health Systems. (2020). Standard 16.01.03. Healthcare Facilities
Accreditation Program: Accreditation requirements for acute care hospitals. (Level VII)
23. DNV GL-Healthcare USA, Inc. (2020). MM.1.SR.3. NIAHO® accreditation requirements, interpretive guidelines and
surveyor guidance – revision 20.0.(Level VII)
https://procedures.lww.com/lnp/view.do?pId=1440722&disciplineId=493
10/13


04/02/2022
Lippincott Procedures - Constipation management, oncology
24. The Joint Commission. (2021). Standard NPSG.02.03.01. Comprehensive accreditation manual for hospitals. (Level
VII)
25. Lai, T. K. T., et al. (2011). Effectiveness of aroma massage on advanced cancer patients with constipation: A pilot
study. Complementary Therapies in Clinical Practice, 17(1), 37–43. Retrieved October 2021 from
https://doi.org/10.1016/j.ctcp.2010.02.004(Level II)
Abstract |
Complete Reference
26. Accreditation Association for Hospitals and Health Systems. (2020). Standard 07.02.03. Healthcare Facilities
Accreditation Program: Accreditation requirements for acute care hospitals.(Level VII)
27. Rutala, W. A., et al. (2008, revised 2019). Guideline for disinfection and sterilization in healthcare facilities, 2008.
Retrieved October 2021 from https://www.cdc.gov/infectioncontrol/pdf/guidelines/disinfection-guidelines-H.pdf
(Level I)
28. U.S. Department of Health and Human Services, et al. (2017). Common terminology criteria for adverse events
(CTCAE): Version 5.0. Retrieved October 2021 from
https://ctep.cancer.gov/protocolDevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_8.5x11.pdf
(Level VII)
29. The Joint Commission. (2021). Standard RC.01.03.01. Comprehensive accreditation manual for hospitals. (Level
VII)
30. Centers for Medicare and Medicaid Services. (2020). Condition of participation: Medical record services. 42 C.F.R.
§ 482.24(b).
31. Accreditation Association for Hospitals and Health Systems. (2020). Standard 10.00.03. Healthcare Facilities
Accreditation Program: Accreditation requirements for acute care hospitals.(Level VII)
32. DNV GL-Healthcare USA, Inc. (2020). MR.2.SR.1. NIAHO® accreditation requirements, interpretive guidelines and
surveyor guidance – revision 20.0. (Level VII)
Additional References
Cherwin, C., & Kwekkeboom, K. (2016). Prevalence, duration, severity, and distress of chemotherapy-related
gastrointestinal symptoms in patients with a hematologic malignancy. Oncology Nursing Forum, 43(5), 561–571.
Retrieved October 2021 from https://doi.org/10.1188/16.ONF.43-05AP
Abstract |
Complete Reference |
Ovid Full Text
https://procedures.lww.com/lnp/view.do?pId=1440722&disciplineId=493
11/13
04/02/2022
Lippincott Procedures - Constipation management, oncology
Gonzales, L. K., et al. (2016). Adjusting bowel regimens when prescribing opioids in women receiving palliative
care in the acute care setting. American Journal of Hospice and Palliative Care, 33(7), 663–668. Retrieved October
2021 from
https://doi.org/10.1177/1049909115584754
Abstract |
Complete Reference |
Ovid Full Text
National Cancer Institute. (2020). Gastrointestinal complications (PDQ®): Health professional version. Retrieved
October 2021 from https://www.cancer.gov/about-cancer/treatment/side-effects/constipation/GI-complications-
hp-pdq
Vallerand, A. H. (2017). Opioid-induced constipation. Journal for Nurse Practitioners, 13(2) , 170–174.e3.
Retrieved October 2021 from https://doi.org/10.1016/j.nurpra.2016.11.006
Younes, W. O., & Tawalbeh, L. I. (2017). Bowel management: Constipation among patients with cancer. Journal
of Palliative Care and Medicine, 7(4), 1–6. Retrieved October 2021 from https://www.omicsonline.org/open-
access/bowel-management-constipation-among-patients-with-cancer-2165-7386-1000310.pdf
Rating System for the Hierarchy of Evidence for Intervention/Treatment Questions
The following leveling system is from Evidence-Based Practice in Nursing and Healthcare: A Guide to Best Practice
(2 ed.) by Bernadette Mazurek Melnyk and Ellen Fineout-Overholt.
nd
Level I:
Evidence from a systematic review or meta-analysis of all relevant randomized controlled trials
(RCTs)
Level II:
Evidence obtained from well-designed RCTs
Level III: Evidence obtained from well-designed controlled trials without randomization
Level IV: Evidence from well-designed case-control and cohort studies
Level V:
Evidence from systematic reviews of descriptive and qualitative studies
Level VI: Evidence from single descriptive or qualitative studies
Level VII: Evidence from the opinion of authorities and/or reports of expert committees
Modified from Guyatt, G. & Rennie, D. (2002). Users' Guides to the Medical Literature. Chicago, IL: American Medical Association;
Harris, R.P., Hefland, M., Woolf, S.H., Lohr, K.N., Mulrow, C.D., Teutsch, S.M., et al. (2001). Current Methods of the U.S. Preventive
Services Task Force: A Review of the Process. American Journal of Preventive Medicine, 20, 21-35.
IP Address: 202.20.63.252, Server: AUSE1PLNSWEB3.WKRainier.com, Session: 96FA380264DFF530DA3FDAF4F210B654
https://procedures.lww.com/lnp/view.do?pId=1440722&disciplineId=493
12/13
04/02/2022
Lippincott Procedures - Constipation management, oncology
©
2022 Wolters Kluwer Health, Inc. and/or its subsidiaries. All rights reserved. License Agreement & Disclaimer Privacy Statement
https://procedures.lww.com/lnp/view.do?pId=1440722&disciplineId=493
13/13
Document Outline