Service Delivery Model
Complexity:
Simple
Low complexity
High complexity
Long-term
No ACC intervention
ACC refers to a
ACC is key
maintenance
provider
Coordinator
Services already in
place
Suited to
Medical fees only
Some rehabilitation
Client needs a
•
Long term
these support
Short but necessary
intervention is
range of support:
stable outcome
scenarios:
time off work – will
needed, but no risk
•
Serious Injury
•
Long-term
return to work
flags:
•
difficult to
Home Support
•
quick referral
obtain new job or
within benchmarks
to arrange stay-at-
“flags”
•
Accidental
work
•
rehabilitation
death claims
•
simple
barriers
•
Lump-sum /
alternative job
Independence
placement
allowance
•
Package of
Care
Client contact:
Primary health
Rehabilitation
ACC case manager
• ACC
provider has main
provider
/ coordinator
coordinator, when
client contact - eg.
•
has face- to-
• has face-to-face
required
GPs
face contact
contact
•
No active
•
leads
•
leads
rehabilitation
rehabilitation plan
rehabilitation plan
needed.
development
development
ACC’s core
•
Accept cover
•
Timely service
•
Complex
•
Efficient
role:
•
Pay entitlement
activation
service
payment
efficiently
•
Cost and
coordination·
•
Check in to
decide to invest in
•
Lead
monitor
•
Advise on
plans
rehabilitation plan
secondary
•
Monitor for
development and
prevention
outliers and flags
delivery
•
•
Monitor
Multidisciplinar
providers
y support
Level of risk
No risk and low
•
No significant
•
Risk of high
•
Long term
and liability
liability
risk flags – but …
liability if not
ACC liability – but
for ACC:
•
Fast recovery
intensively managed
this is accepted
reduces ACC
and timely
liability
outcomes not
achieved
Barriers facing long term unemployed, injured, or disabled
workers returning to work.
Report on international literature search
Compiled for ACC by Fiona Knight
16 January 2004
Table of Contents
1
PURPOSE .................................................................................................................................................... 6
BACKGROUND ..................................................................................................................................................... 6
METHOD ............................................................................................................................................................. 7
ORDER OF THE REPORT........................................................................................................................................ 7
2
PART 1: FACTORS IMPACTING ON RETURN TO WORK .............................................................. 8
LENGTH OF TIME OUT OF THE WORK-FORCE ........................................................................................................ 8
THE CONCEPT OF DISABILITY .............................................................................................................................. 8
3
PART 2: BARRIERS AFFECTING RETURN TO WORK ................................................................. 10
A
PERSONAL FACTORS ............................................................................................................................... 10
Attitudinal barriers ...................................................................................................................................... 10
(a)
Personal responses to stressful life events ......................................................................................... 11
(b)
Response to negative experiences ...................................................................................................... 11
(c)
Loss of status ...................................................................................................................................... 12
(d)
Lack of confidence ............................................................................................................................. 12
(e)
Apprehension regarding re-employment ............................................................................................ 12
PERSONAL ABILITIES ......................................................................................................................................... 13
(a) Capacity to change. .............................................................................................................................. 13
(b)
Personal expectations ........................................................................................................................ 14
(c)
Education ........................................................................................................................................... 14
EMPLOYABILITY ............................................................................................................................................... 16
HEALTH FACTORS ............................................................................................................................................. 17
(a)
Pain management ............................................................................................................................... 17
(b)
Use of cigarettes, drugs, and alcohol ................................................................................................. 18
(c) Mental health ........................................................................................................................................ 19
REFUSAL TO ACCEPT JOBS ................................................................................................................................. 20
AGE, GENDER, ETHNICITY ................................................................................................................................. 20
(a) Age ........................................................................................................................................................ 20
(b)
Gender ............................................................................................................................................... 22
(c)
ethnicity .............................................................................................................................................. 22
TYPE OF DISABILITY / INJURY ............................................................................................................................ 24
PRE-INJURY CIRCUMSTANCES ........................................................................................................................... 25
(a)
Family circumstances ........................................................................................................................ 25
(b)
Job satisfaction .................................................................................................................................. 26
(c)
Job history .......................................................................................................................................... 27
(d) criminal record .................................................................................................................................... 27
(e) obesity ................................................................................................................................................... 27
B
EXTERNAL FACTORS ................................................................................................................................ 27
PERCEPTION OF EMPLOYERS / LACK OF KNOWLEDGE ........................................................................................ 27
JOB ADAPTATIONS ............................................................................................................................................. 29
CASE MANAGEMENT/ REHABILITATION ISSUES ................................................................................................. 30
(a)
Behavioural dimension ...................................................................................................................... 30
(b)
Cognitive dimension ........................................................................................................................... 30
(c)
The affective dimension ...................................................................................................................... 31
(c)
Environmental .................................................................................................................................... 31
LAWYERS’/ ADVOCATES’ ATTITUDES ................................................................................................................ 31
FOCUS ON DISABILITY (RATHER THAN ABILITY) ................................................................................................ 32
CO-WORKER ATTITUDES ................................................................................................................................... 32
TRANSPORT ISSUES ........................................................................................................................................... 33
RETAINING EMPLOYMENT ................................................................................................................................. 33
SELF-EMPLOYMENT .......................................................................................................................................... 35
Page 2 of 144
LABOUR MARKET CONDITIONS .......................................................................................................................... 35
COMPENSATION ENTITLEMENT ......................................................................................................................... 36
CONCLUDING REMARKS .................................................................................................................................... 37
4
PART 3: PROGRAMMES AND INITIATIVES TO REMOVE BARRIERS ..................................... 39
ADDRESSING LENGTH OF TIME OUT OF THE WORK FORCE ................................................................................. 39
(a)
Unemployed ....................................................................................................................................... 39
(b)
Disabled / injured workers ................................................................................................................. 39
ADDRESSING THE CONCEPT OF DISABILITY ....................................................................................................... 40
ADDRESSING PERSONAL ISSUES ........................................................................................................................ 41
(a)
Personal responses to stressful life events ......................................................................................... 41
(b)
Response to negative experiences ...................................................................................................... 41
(c)
Loss of status ..................................................................................................................................... 42
(d)
Lack of confidence ............................................................................................................................. 43
(e)
Apprehensions regarding re-employment .......................................................................................... 44
PERSONAL ABILITIES AND ATTRIBUTES ............................................................................................................. 45
(a)
capacity to change ............................................................................................................................. 45
(B)
PERSONAL EXPECTATIONS ....................................................................................................................... 46
(c)
Education ........................................................................................................................................... 47
(d)
Ability to speak the local language .................................................................................................... 48
EMPLOYABILITY ............................................................................................................................................... 49
ADDRESSING HEALTH FACTORS ........................................................................................................................ 51
(a)
Pain management ............................................................................................................................... 51
(B)
USE OF CIGARETTES, DRUGS AND ALCOHOL ............................................................................................ 53
(c)
Mental health ..................................................................................................................................... 53
(d)
Evidence-based Return to Work Guidelines ....................................................................................... 54
REFUSAL TO ACCEPT JOBS ................................................................................................................................. 54
AGE, GENDER, ETHNICITY ................................................................................................................................. 56
(a)
Age ..................................................................................................................................................... 56
(b)
Gender ............................................................................................................................................... 59
(c)
Ethnicity ............................................................................................................................................. 61
TYPE OF DISABILITY .......................................................................................................................................... 62
(a)
Mental health problems ..................................................................................................................... 62
(b)
People with traumatic brain injury (TBI) .......................................................................................... 64
(c)
People with hearing problems ........................................................................................................... 65
(d)
People with sight problems ................................................................................................................ 65
(e)
People with back problems ................................................................................................................ 66
(f)
People with serious injuries ............................................................................................................... 67
(g)
People with spinal injuries ................................................................................................................. 67
(h)
Other injuries / disabilities ................................................................................................................ 68
PROBLEMS ARISING FROM PRE-INJURY CIRCUMSTANCES .................................................................................. 68
(a) Family circumstances ........................................................................................................................ 68
(b)
Job satisfaction .................................................................................................................................. 68
(c)
Job history .......................................................................................................................................... 68
(d)
Relocation .......................................................................................................................................... 69
(e)
Criminal records ................................................................................................................................ 70
(f)
Obesity ............................................................................................................................................... 70
ATTITUDES OF EMPLOYERS ............................................................................................................................... 71
(a)
The Disability symbol ........................................................................................................................ 71
(b)
Duration of unemployment ................................................................................................................. 72
(c)
Educating employers regarding disabilities ...................................................................................... 73
(d)
Understanding return to work programmes ....................................................................................... 73
JOB ADAPTATIONS ............................................................................................................................................. 74
(a)
Supported employment ....................................................................................................................... 74
(b)
Assistive technology ........................................................................................................................... 76
(c)
Modification of job duties .................................................................................................................. 76
(d)
Teleworking ....................................................................................................................................... 77
(e)
Work trials ......................................................................................................................................... 79
Page 3 of 144
CASE MANAGEMENT / REHABILITATION ISSUES ................................................................................................. 79
ADDRESSING LAWYER AND ADVOCATE ATTITUDES .......................................................................................... 82
FOCUS ON ABILITY RATHER THAN DISABILITY .................................................................................................. 84
ADDRESSING CO-WORKER ATTITUDES .............................................................................................................. 84
ADDRESSING TRANSPORT ISSUES ...................................................................................................................... 85
RETAINING EMPLOYMENT ................................................................................................................................. 86
(a)
Earnings supplements / financial assistance to employees ................................................................ 87
(b)
Wage subsidies for employees ............................................................................................................ 87
(c)
Retention incentives for employers and /or employees ...................................................................... 87
(d)
On-job support ................................................................................................................................... 88
(e)
Protection of employment .................................................................................................................. 89
(f)
Quota systems .................................................................................................................................... 89
(g)
Levy systems ....................................................................................................................................... 90
SELF-EMPLOYMENT .......................................................................................................................................... 90
Operating within prevailing labour market conditions ............................................................................... 93
MULTI-TARGETED PROGRAMMES ..................................................................................................................... 95
RESULTS BASED FUNDING ................................................................................................................................. 96
CONCLUDING REMARKS .................................................................................................................................... 97
5
PART 4: BEST PRACTICE ................................................................................................................... 100
EVALUATION OF PROGRAMMES ....................................................................................................................... 101
PRINCIPLES OF GOOD INTERVENTION DESIGN .................................................................................................. 102
1 Recruitment of participants is the start of the intervention ................................................................... 102
2 View intervention as a social influence ................................................................................................. 102
3 Target motivation, skills, knowledge and resources for coping ............................................................ 103
4 Build self-sufficiency ............................................................................................................................. 103
5 To be successful requires the confidence to try to succeed.................................................................... 103
6 Allow for individual differences............................................................................................................. 103
7 Use active teaching and learning methods, rather than didactic techniques ........................................ 103
8 Blend active learning with model demonstration, graduated utilisation of skills and positive feedback
................................................................................................................................................................... 103
9 Inoculate against setbacks ..................................................................................................................... 104
PREDICTING WHO MIGHT BECOME LONG TERM UNEMPLOYED ......................................................................... 104
MODIFIED WORK DUTIES ................................................................................................................................. 106
DEMAND-SIDE JOB DEVELOPMENT .................................................................................................................. 106
MAINTAINING EMPLOYMENT .......................................................................................................................... 107
BUSINESS PARTNERSHIP .................................................................................................................................. 108
HUMAN CAPABILITY FRAMEWORK ................................................................................................................. 110
THE CURRENT NEW ZEALAND LABOUR MARKET ............................................................................................ 112
HELPING LONG TERM CLAIMANTS ................................................................................................................... 113
HELPING NEWLY INJURED ............................................................................................................................... 113
CASE MANAGEMENT ....................................................................................................................................... 114
POLICY DEVELOPMENT ................................................................................................................................... 115
APPENDICES ................................................................................................................................................... 117
APPENDIX ONE: HOW TO RELATE TO PEOPLE WITH DISABILITIES ............................................................... 117
APPENDIX TWO: OBSTACLES TO RETURN TO WORK QUESTIONNAIRE......................................................... 122
APPENDIX THREE: IDENTIFYING BARRIERS TO REHABILITATION .............................................................. 124
APPENDIX FOUR: IDENTIFYING PEOPLE NEEDING ASSISTANCE WITH JOB RETENTION ................................ 124
APPENDIX FIVE: EVALUATION OF SELECTED EMPLOYMENT AND TRAINING PROGRAMMES ........................ 129
BIBLIOGRAPHY ............................................................................................................................................... 131
Page 4 of 144
Acknowledgements
I would like to thank several ACC staff for their assistance in the development of this
project:
• Helen Brodie and her staff in Information Services, who inter-loaned much of the
resource material for me;
• Ezrai Fae, Laura Ager, Denise Udy, Raewyn Cole, Raj Krishnan and Caro Henckels
who provided valuable comments on the draft report, and suggestions for
incorporation in the report; and
• Donna Engel, who assisted with the production of the report.
Disclaimer
Any errors and omissions in the report are mine. Those views and opinions stated but not
sourced are mine, and do not necessarily reflect those of ACC.
Page 5 of 144
link to page 7 link to page 7
Introduction
1
Purpose
1.1
The purpose of this report is to:
•
Identify the barriers affecting return to work for people who have been out
of work for long periods, whether due to injury or unemployment, based on
an appraisal of international research and interventions;
•
Summarise programmes and initiatives which address these barriers; and
•
Recommend initiatives to remove these barriers for ACC long term
claimants.
Background
1.2
There are currently about 14,000 long term claimants with ACC. While there has
been a significant reduction in the numbers of long term claimants over the last few
years, recently there has been a decline in the rate of reduction. This partly reflects
the impact of the Injury Prevention, Rehabilitation, and Compensation Act 2001,
which required additional assessment of long term claimants before they could
return to independence.
1.3
Other factors affecting the numbers of long term claimants include:
•
As a result of advances in road safety, technology, drug development and
rehabilitation techniques, more people are surviving what would previously
have been fatal accidents, but they sustain serious injuries which take longer
times to heal.
1
•
People injured at a young age still have significant life expectancies. Young
adult males, with such long life expectancies, are a particularly high risk
group in sustaining severe injuries, although research indicates that in
general younger age at injury is associated with good recovery.
1.4
This project was commissioned in the expectation that many of the problems faced
by these long term claimants are similar to those facing long term unemployed,
such as lack of work skills and attitudes, low self-esteem, poor employability, and
negative perceptions and expectations of employers. Researchers have recently
established a relationship between depression and welfare reliance, although
insufficient work has yet been done to quantify this relationship.
2
1.5
This project aims to identify the barriers hindering return to work, and to
investigate overseas practices that deal with them, with a view to identifying
appropriate programmes for use in New Zealand. Such programmes, if successful,
could be expected to enhance significantly the lives of long term claimants.
1 Yasuda et al: 2001 p 853
2 Kalil et al, August 1998 p 12
Page 6 of 144
link to page 8
1.6
Research into individuals with spinal cord injuries indicated that those who were
employed post-injury reported more satisfaction with their lives, required fewer
medical treatments, and rated their overall adjustment higher than individuals who
were not employed
3. There is abundant similar evidence to support making efforts
to help injured workers regain and retain employment. This literature search is
designed to identify ways in which ACC can help its long-term claimants gain
similar life satisfaction.
Method
1.7
The literature search focused on Internet resources and inter-loans sourced through
ACC’s Information Services team. Initial key words included
(long-term)
unemployment, re-employment, barriers, return to work, disabled workers,
unemployable, and
work-ready. Subsequent internet research focused on the actual
barriers identified, and how to address these.
1.8
A consistent pattern emerged in the barriers identified, supporting the original
premise that similar problems face the long term unemployed and those out of
work for long periods due to injury.
1.9
Two significant factors which impact on return to work were identified:
a) Length of time out of the workforce, and
b) The concept of disability.
1.10 While these are closely inter-related, and provide the focus for this report, each
factor is first discussed separately.
1.11 The barriers identified have been addressed simply as barriers against return to
work, regardless of whether it was identified as a barrier to a long term unemployed
/ disabled / injured person. For many barriers, they are the same barriers facing
the long term unemployed , disabled people, and injured people.
A full bibliography of source material is included.
Order of the report
The report is in five main sections:
i)
An introductory section identifying general factors impacting on return to
work after a period out of the work-force;
ii)
The barriers affecting return to work;
iii)
A description of appropriate programmes used overseas to overcome
barriers affecting return to work;
iv)
Analysis of different initiatives and a summary of best practice
v)
recommendations for ACC to assist long term claimants return to work.
3 Yasuda, et al 2002 Article summary
Page 7 of 144
link to page 9 link to page 9 link to page 9 link to page 9 link to page 9 link to page 9 link to page 9
2
Part 1: Factors impacting on return to work
Length of time out of the work-force
2.1
International research concludes that the longer a person is out of work and
receiving some form of benefit or compensation payments, the less chance they
have of returning to full time work. The motivation to find work deteriorates over
time
4. According to Regan and Stanley of the UK Institute of Public Policy
Research, (IPPR) “once a person has been on the benefit for 12 months, the average
duration of their claim will be eight years, with only a one in five chance of
returning to work within five years”.
5 There is considerable evidence that the
longer people remain in receipt of financial assistance, either their mental and
physical health is likely to decline, or they enjoy their changed lifestyle which does
not incorporate being at work.
2.2
An orthopaedic physician’s study of over 100 injured workers found that those who
lost no workdays, or returned to work within 15 workdays of sustaining the injury
were still in employment two years later.
6
2.3
There are other reported risks when an injured worker is out of work for a long
time. For example, in America, because lost time has become routine and
expected even for relatively minor injuries, the Texas Workers Compensation
Commission cautions employers to the likelihood of malingering or of fraudulent
claims.
7
2.4
Notwithstanding these concerns, most people who claim financial assistance
following injury or illness expect to return to work.
8 Up to 40% of such people do
not see their health problems as an obstacle to finding work, but cite a wide range
of other obstacles instead. Each of these obstacles is investigated below.
2.5
An ACC survey of exited claimants showed that about half those not working
considered it was due to their health. Other reasons included age (and ensuing
retirement), family circumstances, employer reluctance to hire people with back
injuries, pregnancy, redundancy, and the lack of suitable / available jobs.
9
The concept of disability
2.6
There is a complex relationship between disability, poverty, low skills and
worklessness. The IPPR found that people who become disabled are more likely to
have been at an economic disadvantage before they became disabled.
10 They are
then more likely to move into low paid, low status jobs, to be in manual
occupations, and to have lower average hourly earnings than their non-disabled
peers, even taking into account age, education, and occupation. The chance of
becoming unemployed again is higher: 33% for people with disabilities compared
4 NZ Employment Service 1996
5 Regan and Stanley: 2003 p 58
6 Melhorn 1996 pp18-30
7 Texas Workers’ Compensation Commission website: <www.twcc.state.tx.us/commission/divisions/rtw>
8 Pathways to Work 2002 p 11
9 BRC January 2003 Appendix 3 Table 4
10 Regan and Stanley 2003 p 57
Page 8 of 144
link to page 10 link to page 10 link to page 10 link to page 10
with 20% for those without disabilities, despite evidence
11 that people with
disabilities have a better attendance record, stay longer in a job and have fewer
accidents in the workplace than the non-disabled.
2.7
In economic terms, as a disability reduces a worker’s productivity, it also weakens
their relative value on the labour market, and power to compete with other job-
seekers.
12 What may be a temporary impairment more easily converts to chronic
disability and dependence when there is a surplus of skills, and as a consequence,
unemployment and disability are overlapping contingencies. If someone with a
temporary impairment cannot find a suitable job, it is likely that the labour market
conditions will interact with their health condition to produce chronic disability.
Whether the resulting unemployability is due to unemployment or disability is then
hard to distinguish.
2.8
Behavioural elements are significant determinants of chronic disability
13. These
include:
•
The recognition of symptoms of impairments;
•
The perception of their incapacitating effects; and
•
The choice of coping strategy.
2.9
The first step on the road to disability is the recognition of the symptoms of an
impairment by the person and/or significant others. The impaired worker will then
try to adapt their condition in a way that is socially acceptable and in agreement
with their own preferences. Workers will define themselves as disabled if they
perceive themselves being impaired beyond remedy, and if they experience a
substantial reduction in work performance. They will be more inclined to do so if
the financial and psychological consequences of disability are not severe.
2.10 The response to injury can be either positive or negative: vocational rehabilitation
and return to work, or chronic disability and persistent dependency. The form of
response will be influenced by the reactions of external parties including
employers, family and household members, case managers, and health
professionals.
2.11 In choosing their response, an injured person will weigh the psychological and
pecuniary benefits and risks. Returning to work brings a person the stress of
employment, having to cope with the vagaries of the labour market and assuming
personal responsibility for one’s life and financial state. Dependency provides
financial stability and exemption from such stresses at the risk of external parties
not legitimising the disability, or of stigmatising the choice as morally inferior. The
proclivity to assume the disabled role is stronger when the perceived costs are
lower and the benefits higher. This can partly explain the prevalence of illness and
disability in low income, low education groups.
14
11 Wilmott
12 Aarts and de Jong 1992 p 62
13 Aarts and de Jong 1992 p 58
14 Luft, Harold S: 1975 pp 43 - 57
Page 9 of 144
link to page 11 link to page 11 link to page 11 link to page 11
3
Part 2: Barriers affecting return to work
3.1
OECD figures show that in every country unemployment was higher in 1989 than
in 1975, even though employment rose rapidly in the 1980s and in 1989 there were
more job vacancies. This led to rising wage inflation, increased interest rates, and
an abrupt end to the boom.
15 This implies there was a failure during the 1980s to
mobilise the unemployed. The 1990s provided a controlled experiment identifying
the factors leading to unemployment – some countries radically changed their
treatment of unemployed people while others did not. The various economic
practices implemented to address the numbers of unemployed have been generally
well documented but few have focused on the actual barriers facing individuals.
3.2
Many of the barriers facing a long term injured or unemployed person returning to
work are directly related to the individual. The way individuals cope with being out
of work has a direct relationship with their chances of returning to work. As
individuals react differently to the above factors, barriers against return to work are
established. These are described as personal barriers, compared with external
barriers which are imposed on the person outside their personal circumstances.
3.3
A British inquiry into inequalities in health cited being out of work as a potentially
major risk to both physical and mental health through:
•
Isolation, social exclusion and stigma;
•
Changing health related behaviour;
•
Disruption to future work career; and
•
Trapping people on lower incomes than available through work.
16
3.4
Most research on personal barriers to return to work focuses on demographic
characteristics, education and work experience. Recent research has identified
factors such as depression, substance abuse and even domestic violence as factors
that hinder long term employment prospects.
17 This research therefore has looked
further at barriers such as psychological functioning, stressful interpersonal
relationships, psychiatric disorders, and personal circumstances. Many of these
factors feature widely in the low-income and welfare populations.
A Personal factors
Attitudinal barriers
3.5
Unemployment, injury, and disability can have negative effects on psychological
and physiological well being. Job loss is a stressful event that threatens a person’s
sense of well being, takes away daily routines, lessens the sense of control people
have over their own lives, and creates changes in perceptions, emotions and
behaviours.
18 It can have deleterious emotional, behavioural, and physical effects.
15 Layard 2003 p 3
16 Acheson D (Chair) Independent Inquiry into Inequalities in Health Report (1998)
17 Zuckerman and Kalil 2000 Barriers to work section
18 Leana and Feldman 1995 p 1386
Page 10 of 144
link to page 12 link to page 12 link to page 12 link to page 12 link to page 12 link to page 12 link to page 12
It entails the loss of a valued role in society…often results in economic hardship
and corrodes one’s sense of mastery, personal identity and close relationship.
19
3.6
Job loss also represents a turning point in life. Some job losers will successful claim
a new work role, while others will be overwhelmed by the “cascade” of negative
financial events, an eroded sense of mastery, will suffer discouragement and
depression and may become a burden or source of stress for the families .
20
3.7
To balance this, there is substantial research indicating that the risks of depressive
symptoms, and the lack of motivation to undertake positive job search, are able to
be addressed by social interventions.
21
(a) Personal responses to stressful life events
3.8
People vary greatly in how they manage stress and uncertainty in their every day
lives. Each individual has available to differing degrees resources that help buffer
them from stressful situations or to lower the stress they would otherwise
experience. These include:
•
Individual skills, such as problem solving and social skills;
•
Levels of support (such as financial or family); and
•
Energy levels, such as physical health and positive outlook on life.
22
3.9
The greater a person’s reservoir of coping resources, the greater the likelihood that
they will cope with stress, uncertainty, and new situations. Conversely, fear or
worry of a negative interpersonal reaction can help that unwanted event to
happen.
23 Activities geared towards obtaining re-employment (such as job search
and retraining) are themselves quite stressful
24.
(b) Response to negative experiences
3.10 Social cognitive theory states that failure experiences can under-mine self-efficacy
and can lower outcome expectancies, eventually resulting in learned helplessness.
Many people without jobs feel frustration and discouragement over their failure to
get a job, and this can lead to negative perceptions of themselves. This negativity
then pervades their expectations of employment and sense of self-worth. They
may blame themselves for their injury or unemployment. The more depressed a
person is when beginning a job search, the less likely they are to:
•
Take the steps necessary to find a new job;
•
Keep their spirits up in the face of any rejections associated with job search
activities, and
•
Present themselves to potential employers in a positive light
25.
19 Price, Vinokur and Friedland 1995 p 22
20 ibid
21 Caplan, Vinokur and Price 1997 p 345
22 Lazarus and Folkman (1984)
23 Peale NV: The Power of Positive Thinking 1952
24 Leana and Feldman (1995): p 1384
25 ibid p 1383
Page 11 of 144
link to page 13 link to page 13 link to page 13 link to page 13 link to page 13 link to page 13
3.11 If a person was already pre-disposed to anxiety and depression, these factors will
impact on his or her acceptance of the injury and view of the future.
26
(c) Loss of status
3.12 Related to this is the concern over loss of status. A British trial to assist people
move off the Incapacity Benefit into employment
27 had mixed results when some of
the older beneficiaries refused to participate in some aspects of the trial as they
considered them “patronising and unsuitable for people who had years of
employment experience”. They were unwilling to consider “work which was
deemed to be insulting to their abilities.” This is in reality a failure of the
programme to meet the clients’ needs, and serves as a reminder that one size does
not fit all. Successful interventions are those designed to fit the needs of the
clients, not the needs of the agencies / experts.
(d) Lack of confidence
3.13 The British Department for Work and Pensions has researched various initiatives to
help return incapacity beneficiaries to work and, in one study, found that nearly
half of those beneficiaries actively seeking work had low confidence about working.
More than a third considered it unlikely that they would get a job because of their
health problems, and half of them thought that there weren’t job opportunities
available locally for people like them
28. A Canadian study found evidence of lack
of confidence because of age: “ If I did go back to work, given that I’m 48 years old,
who would hire me?”
29
(e) Apprehension regarding re-employment
3.14 Fear of the effect of re-employment on their injury or health, and of re-injury is
another common barrier for long term injured or ill workers against returning to
work. These are often unexpressed and sometimes unrecognised fears. “ If I knew
I could do it {work} then I would…but I’m so uncertain about it…what affect
would it have on your health”.
30 Losing a job through restructuring or continuing
ill-health creates another perceived potential stress of applying for unemployment
or disability benefits that acts as a disincentive to start seeking a job.
3.15 Fear of leaving the security of a benefit to take up paid employment is a significant
barrier
31. A British survey of more than 1600 beneficiaries revealed their top three
concerns were financial: having enough money to live on, coping financially until
the first pay (usually at the end of the month), and paying the mortgage/rent.
There was, again, a great deal of concern about reclaiming the benefit if the job did
not work out or last, due to the perceived complexities and capriciousness of the
rules. Fears that the job might not pay well, or that they would lose some of their
entitlements were also important concerns.
26 New York State Workers’ Compensation Board p 32
27 Heenan 2002 p 392
28 DWP: Short-term effects of voluntary participation in ONE
29 <www.returntowork.org/voices.html>
30 <www.returntowork.org/voices.html>
31 Woodland, Mandy and Miller 2003: p 64
Page 12 of 144
link to page 14 link to page 14 link to page 14 link to page 14
3.16 These fears were borne out by Harries and Woodfield’s research
32 on the
transitional experiences of people moving from benefit to paid employment. The
greatest disruption was the change in income cycles from weekly or fortnightly to
monthly. Making a monthly pay packet last for a monthly basis can be very
challenging. Often, too, there were additional costs related to employment, such as
childcare, travel, clothing and toiletries.
3.17 Perceptions of the likelihood of being able to move off income support are likely to
affect whether people actually do so. British research showed nearly two-thirds of
respondents felt trapped on income support
33. Family type, education, and ability
to “make ends meet” have a major effect on the likelihood of a welfare claimant
feeling trapped, whereas having a health or disability problem does not. Perception
of the local labour market was also a strong influence: nearly four-fifths of the
respondents believed their chances of finding a full time permanent job in their
areas was not very good. Lastly, workers who attach less value to employment
have significantly greater periods of unemployment
34.
Personal abilities
3.18 Research has identified several personal attributes (whether innate in the worker or
cultivated as a skill) which assist people cope with the stresses of injury and long
term unemployment. The converse is that the lack of these attributes helps create
barriers against return to work.
(a) Capacity to change.
3.19 With changes in technology, closure of work premises, changes in consumer
demand, some types of jobs are no longer available. These types of changes in the
labour market require workers and job-seekers to change as well. Some types of
injury rule out a return to pre-injury occupation, especially for manual workers. If
they are to return to work, these workers will have no option but to change their
occupation. Whether they succeed in finding employment will, to a large degree,
depend on their willingness to change and their ability to change.
3.20 Willingness to change is often seen as a generational issue: as people age, their
tolerance to change lessens and their resistance to change grows. Changing jobs
can put people outside their comfort zones and increase their stress levels,
especially when older people see youngsters performing tasks that they themselves
are unable to do.
3.21 The ability to learn is a key aspect of capacity to change. Employers involved in a
Philadelphia welfare-to-work scheme repeatedly stressed soft skills including good
attitudes, good work habits and ability to learn. “If some-one meets our criteria, we
can teach them the specific skills they need for our site”
35.
3.22 The US National Multiple Sclerosis Society has proven that changing physical job
demands and working conditions has helped MS sufferers cope with the effects of
32 Harries and Woodfield 2002 p 32
33 Shaw, et al 1996 p 122
34 WCRI Research brief 1996 Vol 12 No9 p 3
35 Hangley and Loizillon 2002 p 6
Page 13 of 144
link to page 15 link to page 15 link to page 15 link to page 15 link to page 15 link to page 15 link to page 15 link to page 15 link to page 15 link to page 15 link to page 15
their illness and maintain their employment
36. This has a parallel for injured
workers, whose injuries prevent them remaining in their pre-injury occupation.
(b) Personal expectations
3.23 The worker’s expectation of his or her performance is probably one of the biggest
predictors of success in returning to work. The National Multiple Sclerosis Society
has also proven that personal attributes such as hope, personal control and sense of
humour helped MS sufferers cope with the effects of their illness and maintain their
employment. A study conducted with the Commonwealth Employment Service in
Australia, found a significant relationship between those who blamed themselves
and those remaining unemployed
37.
3.24 Acceptance of residual “scars” from injury is an important ability facing those who
return to work. Developing self-awareness and acceptance of deficits resulting
from traumatic brain injury is the key aspect in the process of rehabilitation, and
those unable to do this will not be able to become productive in the community
38.
(c) Education
3.25 Basic literacy and numeracy skills are key requirements for most jobs
39. Those with
numeracy and/or literacy problems tend to take longer to regain employment after
injury or long term unemployment. More than half the beneficiaries (whether on
unemployment or invalid benefit) in one study
40 had no school qualifications at all,
and more than three quarters of them had left school by the age of 16. An
American study identified limited proficiency in English as a further barrier
41. In
this study, 41% of the TANF (Temporary Assistance for Needy Families) caseload
in Los Angeles County had limited proficiency in English, reflecting the fact that
17% of the case load were foreign-born.
3.26 Poor English skills were identified in a study of New Zealand Employment Service
long-term clients,
42 as well as in a study of its own claimant group by ACC’s then
subsidiary Catalyst
43. Claimants who could neither read nor write English could
not understand any information given to them by the two agencies. Statistics NZ
figures from the 1996 Census show that less than 2% of New Zealand residents do
not speak any English, compared with about 5% of the American population,
according to US Census 2000 data
44. Studies in the US have shown a strong
connection between language ability, employment and earnings.
45
3.27 New Zealand and international studies cite low levels of education as a significant
barrier to regaining employment.
46 In America, the lack of a high school diploma
can make it difficult for individuals to find jobs, either because the diploma is a
36 source
37 Waters and Moore 2001 p 601
38 Ben-Yishay and Lakin: Structured group treatment for brain injury survivors
39 DWP: Well enough to work?
40 Woodland, Mandy and Miller 2003: p 60
41 Goldberg 2002 p 4
42 NZ Employment Service 1996
43 Pack Margaret: internal ACC report 2002
44 Wrigley et al August 2003
45 ibid
46 NZ Employment Service 1996
Page 14 of 144
link to page 16 link to page 16 link to page 16 link to page 16 link to page 16 link to page 16 link to page 16
pre-requisite for the job, or because individuals without the skills of a high school
graduate cannot perform the duties associated with many jobs.
47 A Michigan study
showed that only 39% of women with no high school qualification worked at least
20 hours a week, compared with 66% of women with a high school qualification
48.
A 1996 study of employers’ entry-level job requirements found that most required
employees to perform one or more of these following skills on a daily basis:
•
Reading and writing paragraphs;
•
Dealing with customers;
•
Doing arithmetic; and
•
Using computers
49.
3.28 Other American studies indicated that these skills were beyond the abilities of the
average welfare recipient or high school drop-out, and therefore reduced markedly
their ability to gain any employment
50. The American Testing Service estimated
that 40% of welfare recipients had such low levels of literacy that they were unable
to complete tasks such as completing applications for social security.
51
3.29 Compounding this barrier to employment is that many people lacking literacy skills
are very aware of the lack, and the problems it can create. Over time, they have
developed sometimes quite sophisticated techniques to conceal the lack so that
even case managers and career advisers are unaware of their lack of literacy skills.
3.30 Higher education / higher intelligence are important factors. In Canada,
technological skills and advanced education are becoming minimum requirements
for obtaining and retaining employment, while jobs in areas such as manufacturing
are becoming scarce
52. As products and job skills become outdated, those with
computer, maths and literacy skills are favoured. Most studies have found that
better educated workers are more likely to return to work than less educated
workers, and this is backed up by the most recent BRC New Zealand survey of long
term claimants who had exited from the ACC scheme.
53
3.31 Reasons for the higher rates of return to work for those better educated include:
•
A physical impairment is less likely to have an impact as better educated
workers jobs are usually not physically demanding;
•
Better educated workers usually have more control over the manner in
which they perform their jobs, so are able to adapt their activities to
accommodate physical limitations; and
•
Generally employers have invested more in better educated employees
which provides an incentive to make their own accommodations in order to
retain these workers.
47 Goldberg, 2002 p 4
48 Danziger et al, 2000 p 32
49 Holzer 1996
50 Danziger et al, 2000. P 5
51 Brown 2001 p 88
52 Bunch and Crawford, 1998 p 25
53 BRC research report: Return to sustainable earnings January 2003
Page 15 of 144
link to page 17 link to page 17 link to page 17 link to page 17 link to page 17 link to page 17 link to page 17 link to page 17
3.32 More than two-thirds of the respondents in the New Zealand Employment Service
survey of long term unemployed in 1996 acknowledged that lacked appropriate
skills or work experience, while 22% admitted they had literacy or numeracy
problems.
54
3.33 In 1997, New Zealand participated in the International Adult Literacy Survey (IAS),
which was the first internationally comparable estimate of literacy skills in the
adult population. The IALS tested respondents from 12 OECD countries on prose
comprehension, comprehension of graphs, timetables, and charts, and applying
arithmetic operations. The results showed that abut one in five workers had
pressing literacy needs. Almost half of all adults aged 16 – 65 were estimated to be
at the lowest levels of ability.
55
Employability
3.34 Employability is identified as another barrier against return to work
56. While there
is no standard definition of employability, it encompasses gaining and maintaining
employment, having and deploying the appropriate knowledge, attitude and skills,
and presentation (both of qualifications and experience, and during job interviews)
that employers value. It is having job skills and credentials which cut horizontally
across all industries and vertically across all jobs from entry level to chief executive.
Since it can be difficult for employers to obtain reliable information on
employability, many rely upon general impressions of the people concerned and
stereotypes of group to which they belong
57.
3.35 Several American studies found that many of the longer term unemployed were
simply not “work-ready” in that they did not understand or follow workplace
norms or behaviours
58. Many participants in special programmes failed because
they did not understand the importance of punctuality, the seriousness of
absenteeism, and either resented or misunderstood the lines of authority and
responsibility in the workplace.
3.36 That employers value generic employability skills above specific occupational skills
is a well supported finding, and applies to all size companies, to the public and
private sectors, and at all levels of management.
59 Studies continue to confirm the
need for employees to have social skills, positive attitudes about work, and basic
communications skills. Other research showed that employers discharge or fail to
promote workers because of behaviour reflecting an inadequate work value or
attitude, rather than because of a deficiency in job skills or technical knowledge.
60
3.37 A New Zealand trial programme
61 targeted to assist long term unemployed was
based on the contention that many long term unemployed had entrenched personal
and social problems that inhibited their ability to participate in the labour market.
The actual barriers identified during the development of the programme included:
54 Parker 1997 pp 68-9
55 Department of Labour p 27-8
56 Hillage J and Pollard E (1998) Executive summary
57 van den berg and van der Veer p 178
58 Danziger et al, 2000 p 5
59 Cotton p3
60 Gregson and Bettis 1991
61 Wehipeihana p 5
Page 16 of 144
link to page 18 link to page 18 link to page 18 link to page 18 link to page 18 link to page 18
•
Alcohol or drug dependency problems;
•
Anger management problems;
•
Disruptive or dysfunctional family situations;
•
The psychological consequences of domestic violence or abuse, either
historical or current;
•
Illiteracy - often well disguised or hidden;
•
A bad reputation in the local small community; and
•
Unrealistic notions about the income generating potential of hobbies or
artistic pursuits.
3.38 For some participants in the programme, the barriers were not immediately
apparent to the facilitators, or known or acknowledged by the participant. The
process of identifying barriers was described as “akin to peeling an onion – as soon
as one barrier was identified and overcome, another deeper issue would rise in its
place…the surface barriers to employment were often mere symptoms of much
more deep seated problems”.
3.39 One of the facilitators for the NZ programme expressed concern that case managers
are not able to see their clients often enough, or for long enough, for barriers such
as these to become evident. Further, the computerised assessment tools as used by
Work and Income cannot take into account any problem or issue that is not
employment related. The lack of follow-up after attendance at programmes often
left participants feeling even less motivated than they were before starting
programmes
62.
Health factors
(a) Pain management
3.40 Coping with pain has long been cited as a reason not to work. Pain-related
behaviours that communicate a person’s pain to others have often been supported
inadvertently by the healthcare system
63. Patients in pain may get increased
support and sympathy when they express suffering, which then increases “pain
behaviour”. One of the goals of pain rehabilitation should be to reduce the effects
of demotivating factors for patients for return to work. Families can inadvertently
reinforce an injured person’s sick behaviour and delay any return to work simply
because they are trying to help some-one they love
64
3.41 Multi-disciplinary pain management programmes give promising results in helping
injured workers back to work
65 66, with one limited study
67 showing that such a
programme was more effective for short-term patients (up to 12 months) than long
term patients. American studies show that increasing patients’ own resources to
deal with pain situations can be an effective way of increasing self-confidence and
62 ibid p 24
63 Gard and Sandberg 1998.
64 McIntosh, Melles and Hall 1995 p 199
65 Morley et al: …randomised control trials of cognitive behaviour therapy for chronic pain
66 Flor et al: Efficacy of multidisciplinary pain treatment centers
67 Marhold, Linton and Melin 2002: p 73
Page 17 of 144
link to page 19 link to page 19 link to page 19 link to page 19 link to page 19 link to page 19 link to page 19
improving motivation to return to work
68. More research is scheduled to assess the
effects on long term patients. In New South Wales, it is accepted that a significant
proportion of back injury cases will never recover completely and that their back
pain will need to be controlled and adapted to.
69
(b) Use of cigarettes, drugs, and alcohol
3.42 Smoking is an activity which can impact negatively on an injured worker’s return to
work. Smokers are already at risk of lung cancer, heart disease, emphysema, and a
shorter life expectancy. US Army research during an eight week basic training
programme with new recruits
70 showed that, even after controlling for other factors
which might influence the risk of injury, the smokers were 1.5 times more likely to
suffer fractures, sprains and other physical injuries than non-smokers. They had
also had more previous injuries and illnesses, were less physically active, and were
less physically fit than the non-smokers. Risk of injury for smokers was high,
despite the fact that recruits were forbidden from smoking during the training
period.
3.43 Alcohol is connected with over half of all traumatic brain injuries. If some-one
used alcohol or other drugs before they were injured, there is a good chance that
the problem will continue afterwards.
71
3.44 Injured workers are already at risk of infection and other health problems: smoking
increases the likelihood, placing them at even higher risks. Rehabilitation
specialists dealing with people with spinal cord injuries
72 advise them to cease
smoking because of:
•
Difficulties in breathing, especially difficulties in expelling air because of the
build-up of mucus and other secretions in the lungs;
•
Increased chances of developing stomach ulcers, poor circulation, pressure
sores and bladder cancer;
•
Decreases in the body’s supply of vitamin C, so skin wounds heal more
slowly; and
•
An impaired ability to cough, leading to respiratory diseases (20% of
quadriplegics die because of an inability to cough).
3.45 There is also a higher prevalence of smoking, exposure to passive smoking, and a
heavier consumption of alcohol among people who are unemployed.
73
3.46 Drug and alcohol related problems also feature as a barrier to re-employment of
long-term unemployed. While the exact definitions of drugs and alcohol problems
vary widely, and accurate estimates of affected numbers are hard to obtain, there is
general consensus that dependency and abuse does create problems, especially in
keeping a job.
74 Former alcohol and drug abusers continue to have low self-esteem
68 Gard and Sandberg 1998
69 Mills and Thornton 1998 p 594
70 Gardner John W: Press statement Smoking linked to physical injuries, 16 March 2000
71 CTS Rehabilitation Specialists Programme website: http://p2001.health.org/RS01/MODULE4PM.htm
72 CTS Rehabilitation Specialists Programme website: http://p2001.health.org/RS01/MODULE4PM.htm
73 Elkeles and Seifert 1997 pp 41-45
74 Institute for Research on Poverty: The New face of Welfare
Page 18 of 144
link to page 20 link to page 20 link to page 20 link to page 20 link to page 20
which hampers successful employment and weakens their ability to make
successful transitions from welfare to work.
3.47 In a random analysis of 250 case files, ACC subsidiary Catalyst found addiction
issues. Claimants had self-medicated using prescription and /or recreational drugs
and alcohol to manage pain. The ensuing dependency on those substances
hampered rehabilitation.
75
(c) Mental health
3.48 Mental health is a less recognised barrier to return to work, and research is still
underway to identify what mental health problems affect people’s ability to return
to work in order to make recommendations for policies to address this.
3.49 Studies suggest that low income single mothers are particularly at risk of significant
mental health problems when they lose their jobs
76. Importantly, however women
in this group are no more likely than their employed counterparts to be alcohol or
drug dependent.
77
3.50 The term “post traumatic stress disorder” (PTSD) was adopted in 1980 to describe
the pattern of symptoms exhibited by some people who experienced a traumatic
event. Traumatic events range from high profile disasters / bombings to personal
events such as assault, robbery, motor vehicle crash or an accident. Any or all of
three types of symptoms may be experienced by PTSD sufferers including:
•
Persistent flashbacks;
•
Avoidance of any reminders of the event; and
•
Increased alertness /hyper vigilance.
3.51 Although these reactions do not always lead to a diagnosis of PTSD, the trauma
symptoms that individuals experience can be severe enough to affect people’s day
to day lives and their ability to work.
78
3.52 People with existing mental illnesses are generally thwarted by three main barriers:
a)
Their psychiatric professionals tell them they won’t have to work, or cannot
work because of their illness;
b)
People are afraid of losing their benefits; and
c)
People have difficulty communicating with their employers, whether to tell
them about their illness, and how to do that.
79
3.53 Health professionals in New South Wales have identified that the costs of private
psychiatric services are high, while publicly funded mental health services may give
low priority to problems such as anxiety, depression, emotional stability and social
75 Pack 2003 p 13
76 Tainter 1998 p 1
77 DeGroat 1998 Press statement 23 November 1998
78 Rick, Young and Guppy Executive summary
79 Granger Barbara of Matrix Research Institute, on website <www.matrixresearch.org>
Page 19 of 144
link to page 21 link to page 21 link to page 21 link to page 21 link to page 21 link to page 21 link to page 21
isolation.
80 In many cases, more unemployed people live in geographic areas
where public health services may be in limited supply.
3.54 There is growing evidence that under-employment and inadequate employment
also lead to poor health and mental health outcomes.
81 Under-employment
includes:
•
Working fewer hours than desired
•
Being underpaid
•
Being unable to find work that fits the individual’s skills and education.
3.55 These all constitute barriers against return to sustainable employment, and are
addressed elsewhere in this report.
Refusal to accept jobs
3.56 Some men do not take part-time or temporary jobs because such jobs do not pay
much more than they get remaining on welfare benefits
82, while others with
industry specific experience are likely to wait for re-employment in jobs similar to
the ones they used to have, rather than accept a less well paid job in another
industry.
83 Some people price themselves out of jobs by refusing to accept the
levels of wages offered.
3.57 Most jurisdictions require injured workers to co-operate in their rehabilitation.
Some workers use their right of review of their individual Return to work /
Rehabilitation plans to stall a return to work. Workers respond to incentives to
exaggerate or falsify claims of work-related injuries, including that numbers of
claims filed increases with benefits available, and some workers overstate the
limiting effects of injuries in order to delay return to work.
84 Following a study of
3700 workers with back problems, the researchers commented on “the relative ease
with which back pain can be overstated by patients seeking disability benefits and
time off work.”
85
Age, gender, ethnicity
(a) Age
3.58 Older workers are much less likely to return to work than younger workers
86.
American experience of the corporate downsizing in the late 1980 and early 1990s
was that proportionately more older workers were laid off, and less investment was
made in training or retraining older workers. These practices put older workers at
a disadvantage, even before they have an injury and seek re-employment or
retraining. As people move into their 50s and 60s, they are more likely to
experience health related problems, and an injury can have the effect of moving
them into early retirement.
80 Harris et al 1998 p 292-3
81 Price 2000 p 5
82 Borooah 2001 Section 4.1
83 McCormick B: Unemployment Structure and the Unemployment Puzzle 1991
84 Johnson, Baldwin and Butler 1998 pp 39 - 62
85 ibid p 28
86 Baldwin and Johnson 1998 pp39 - 62
Page 20 of 144
link to page 22 link to page 22 link to page 22 link to page 22 link to page 22
3.59 In contrast, the majority of executives and leaders are older adults.
87 Work
performance does not decline with age until well into the seventies and beyond.
Given that there are no major health problems, most people remain at the same
level of ability up to very late life. There are, however, age related changes in the
central nervous system which may impact on speed of processing information and
efficiency of processing complex information. The correlation is generally more
between cognitive ability and work performance. Learning, memory, intelligence
and speed are related to overall cognitive ability. Given that most jobs do not
involve maximum levels of performance, most older workers can perform their
work tasks satisfactorily.
3.60 Age does affect individuals differently: older workers tend to prefer more
responsibility, interesting work, and attention demands
88 while younger workers
prefer autonomy and social opportunities. Some studies have shown that younger
workers may lack the knowledge to make accurate judgements about the likelihood
of efforts paying off.
3.61 Human Resources Development Canada
89 identified a specific list of barriers faced
by older workers attempting to return to the workforce:
•
Lack of job search skills – older workers tend to have relatively steady
employment histories, and so have not used the skills needed for a
successful job search. Thus their job search techniques tend to be outdated,
and their approaches generally less innovative than younger people;
•
Absence of relevant skills for positions in the growth industries – this
includes levels of literacy, numeracy, and technical and computer skills;
•
Level of formal education. In today’s environment, low educational
attainment greatly hampers the abilities of workers to market themselves to
prospective employers;
•
Older workers are also generally less willing to relocate for an employment
opportunity than younger individuals;
•
Related to this is the unwillingness of many financial institutions to approve
long term mortgages to individuals with limited years of employment
remaining to them.; and
•
Capacity for acquiring training and professional development, or perceived
capacity for skills upgrading.
3.62 While any one of these may relate to any person seeking to return to work after an
absence, older workers tend to face several of them concurrently. Some older
workers feel social pressure to withdraw from the workforce in order to provide job
openings for younger workers, and thus to reduce the unemployment rates among
younger individuals
90. A British survey found that more than half the beneficiaries
over 55 years of age did not want to work
91. However, while many displaced
workers choose retirement over job search and/or retraining, a considerable
number are simply not financially or emotionally prepared for retirement.
87 Sterns and Miklos: p 255
88 Phillips, Barrett and Rush: job structure and age satisfaction
89 Human Resources Development Canada Technical Report #1: 1997 Section 1.1
90 HRDC: Lessons learned – a review of older worker adjustment programs 1997 Section 7.2
91 Woodland, Mandy and Miller 2003: p 22
Page 21 of 144
link to page 23 link to page 23 link to page 23 link to page 23 link to page 23 link to page 23 link to page 23 link to page 23
3.63 A Canadian study on the needs of older workers indicates that the older individuals
who participate in active approaches to improving re-employment opportunities
appear to benefit from programmes which are more client centred. Programmes
which have not addressed the specific employment barriers faced by older workers
have been found to have little, if any, impact on these people gaining employment.
3.64 Regardless of gender, older people with disabilities are less likely to participate in
the labour market. In Canada, nearly three-quarters of those with disabilities aged
between 55 and 64 years were not in the labour force compared with only 30% for
those aged 15 – 24 years. In general, the high rate of non participation in the
labour force for the older age group was attributed to age related factors more than
disability related factors
92.
(b) Gender
3.65 Most US studies found that men return to work sooner than women
93 although this
is not supported by Canadian studies. Married men are more likely to return to
work than unmarried males or women, and unmarried women are more likely to
return to work than married women. One study found that gender does not affect
the probability of returning to work, but among those who return, women were
more likely to experience multiple periods of work absence and unsuccessful return
to work, and that part of this may reflect a need for services different from those
provided to men.
94 Women are more likely than men to report pain problems
which can inhibit ability to work.
95
3.66 In general, the reduced demand for unskilled labour in industrialised countries has
a disproportionate effect on male joblessness.
96 Add to this that unemployment is
concentrated among men with few or no educational qualifications, the other
personal factors described elsewhere in this paper have a dominant effect. New
Zealand data is consistent with this international trend.
97
(c) ethnicity
3.67 An Australian study found a disproportionate number of Arab state immigrants
(56% injured compared with 10% in the Australian population) and Mediterranean
country immigrants (28 % compared with 12%)compared with Anglo Saxon
heritage (16% compared with 64%) in his study of 50 incapacitated back cases
98.
American research into the relationship between ethnicity and return to work for
traumatic brain injured workers is inconsistent.
3.68 While some studies found that race was related to failure to return to work, the
results of other studies were less positive
99. (While 13% of the minority group
returned to work post a traumatic brain injury compared with 30% of the white
group, only 45% were working at the time of injury compared with 60% of the
92 Bunch and Crawford p 40.
93 Johnson and Ondrich 1990 p 585
94 Butler, Johnson, and Baldwin, 1995 pp 72-84
95 Marhold et al (2002) p74
96 Borooah, 2001 Section 1
97 According to Parker, prior to undertaking a survey of very long term job seekers in June 1996, 74% of all
job seekers registered with the NZ Employment Service for more than 52 weeks were male.
98 C Landon Smith: 1977 p 1076
99 Yasuda et al 2001 p 854
Page 22 of 144
link to page 24 link to page 24 link to page 24 link to page 24 link to page 24 link to page 24 link to page 24
white group. This means that less than a third of the minority group returned to
work, compared with half the white population.)
3.69 The finding of employer audit studies that African-Americans and Latinos were less
likely to receive job offers than are whites with comparable credentials
100 is backed
up by qualitative studies. In the Netherlands, unemployment has reached
unprecedented levels amongst immigrants, political refugees, caravan-dwellers and
gypsies
101. While researchers admit there are certain real problems (language
difficulties, insufficient or incompatible educational qualifications, and cultural
differences) which contribute to the weak position of such groups, there are
undoubtedly imagined problems due to gender and race stereotyping.
3.70 Canadian research has identified that immigrant, refugee and racial minorities are
virtually invisible to the health authorities, and therefore they do not receive
appropriate assistance or healthcare.
102 103 Studies actually state that “racism
continues to be a barrier to employment”
104, despite legal requirements for equity
and against discrimination.
3.71 In 1996, just over half of all job seekers registered with the New Zealand
Employment Service were of NZ European ethnicity, and 35% Maori.
105 ACC’s
own statistics show that Maori aged 15 – 39 are over-represented amongst
claimants compared with non-Maori.
106 They are also over-represented (by 200%)
in sensitive claims in Auckland, Wellington and Napier cities, in rubgy accidents,
and in serious injury claims. Sixty percent of Maori adults earn $20,000 or less per
annum.
100 Danziger et al, 2000 p 5
101 ven den Berg and van der Veer: The myth of unemployable people
102 ACEWH
103 White J website <www.pwhce.ca/ptsd-immigrant.htm>
104 Bunch and Crawford 1998 p 28
105 Parker 1997 p 65
106 ACC Fourth Quarterly Maori Report 2002/3
Page 23 of 144
link to page 25 link to page 25 link to page 25 link to page 25 link to page 25
3.72 Occupational groups for Maori are shown in the table below:
5.0%
4.5%
4.0%
3.5%
3.0%
2.5%
2.0%
1.5%
1.0%
0.5%
0.0%
ng
ng
ly
s
e
e
e
ni
ing
tion
ion
ishi
rade
rade
ant
anc
vices
enc
at
vices
vices
Mi
tur
upp
torag
vices
ac
S
truc
e T
l T
er
ur
er
ef
er
ervices
er
ai
taur
duc
nd F
uf
er
al
ns
D
S
S
at
ons
et
es
nd S
s S
E
ty S
C
es
R
ion S
Man
nd I
ther
hol
nd R
rt a
cat
ines
ional
estry a
W
a
po
ni
e a
us
ion and
or
and W
nc
ommuni
reat
and o
F
as
strat
C
ec
e,
afes
C
Trans
ommu
Fina
ini
d R
tur
C
rty and B
ion,
dm
th and
ersonal
tricity, G
A
al an
P
gricul
rope
nt
eal
A
lec
P
tur
E
H
ul
nme
C
er
ccommodat
ov
A
G
Maori
Other ethnic groups
One third of the Pacific peoples and “other ethnicity” respondents to the New
Zealand Employment Survey reported that they had trouble speaking English.
Type of disability / injury
3.73 Type of disability is a more important influence on return to work than severity.
Persons with amputations or bruises or contusions were more likely to return to
work sooner than people with sprains, dislocations or fractures
107. A Canadian
survey indicated that workers with soft tissue injuries felt they had greater
difficulties than amputees or people with clearly visible disabilities.
108
3.74 Back problems are reportedly the single most costly workplace injury.
109 Nearly
80% of all adults can expect to experience a disabling episode of back pain at least
once in their lives. In New South Wales, back injuries account for 31% of all
workplace injuries.
110 Several studies indicate malingering, exaggeration or false
claims of workplace back injuries, including an Australian study by a senior
surgical registrar who found that in 38 out of 50 back injury cases studied,
consultants doubted the genuineness of symptoms or manifestation of clinical
signs.
3.75 Other studies show that many workers with back injuries who return to work are
unable to continue that employment because of functional limitations associated
with their condition
111. For workers who return to work in less than one month,
those with neck or back injuries return more quickly than those with leg, arm
107 Johnson and Ondrich 1990 p 584
108 Canadian Injured Workers Alliance: 1995 p 35
109 Johnson, Baldwin and Butler 1998 p 39 - 62
110 Mills and Thornton 1998 p 594
111 ibid
Page 24 of 144
link to page 26 link to page 26 link to page 26 link to page 26 link to page 26 link to page 26 link to page 26 link to page 26 link to page 26
injuries etc
112. But among longer duration injuries, those with neck or back
injuries return more slowly.
3.76 Women have been found more likely than men to develop Post Traumatic Stress
Disorder (PTSD) when exposed to a trauma, and low income women are even more
likely than the general population to do so. The prevalence of PTSD is wider than
was previously believed
113, but as yet, there are few studies of its impact on return
to work, other than the considerable general evidence that psychiatric disorders are
associated with lower rates of employment
114.
Pre-injury circumstances
3.77 Workers who attach less value to employment, whose education and skills levels
are low, or whose industries involve casual / intermittent employment have
significantly longer durations off work. Those with one spell of unemployment in
the middle of the year prior to injury took 34% longer to return to work. Knowing
this employment history can help identify those workers at risk of long term
unemployment when an injury occurs.
3.78 Likewise, workers with less than six months tenure or more than 10 years job
tenure returned to work more slowly.
115 The Washington Community Jobs
Program reports that 75% of its programme participants have poor work histories
which hinder them from securing stable unsubsidised employment.
116
(a) Family circumstances
3.79 Family circumstances, such as marital status or having a dependent or disabled
child or spouse can also influence the ability and motivation of an injured worker
to return to work. Single people were more likely never to have worked than those
who were currently or had been married or cohabiting. Nearly ten percent of one
study’s respondents did not want to work because they wanted to look after their
children, and more than three quarters did not want to work because of their
health
117.
3.80 A New Zealand study by Work and Income indicates that “dysfunctional family and
spousal relationships often have a significant impact on some clients’ abilities to
find and sustain suitable employment”
118. This is endorsed by several American
studies
119 which also note that women who are in abusive relationships encounter
increased interference from their male partners as they attempt to move from
welfare into work. Other US research
120 indicates that between a fifth and a quarter
of welfare respondents have children with health, learning, or emotional problems
which inhibit their parents’ ability to work.
112 WCRI Research brief Vol 12 no 9
113 Kalil et al, August 1998 p 10
114 ibid p 9
115 WCRI Research brief Vol 12 no 9
116 Transitional Jobs, March 2003
117 Woodland, Mandy and Miller 2003 pp21-23
118 Wehipeihana, June 2000 p 22
119 Kahlil et al, August 1998 pp11-12
120 Goldberg, 2002 p 3
Page 25 of 144
link to page 27 link to page 27 link to page 27 link to page 27 link to page 27 link to page 27
3.81 Belgium has identified childcare as one of the most important obstacles for long
term unemployed women to re-enter the labour market.
121 American research into
barriers facing welfare recipients trying to gain employment identified that needs
for specialised childcare, and classified this as:
•
Non-standard-hours care – early mornings, evenings, nights, weekends, and
for shifts longer than eight hours;
•
Sick-child care, for those too sick to attend school or day care; and
•
Special needs care for children with physical, emotional, or mental
disabilities.
122
3.82 The problem of non-standard-hours childcare is especially relevant to New Zealand
with recent changes in the labour market towards increased casualisation of the
labour force and the increase in the size of the service sector.
3.83 The American study team also identified 16 employment liabilities, of which four
were significantly related to a welfare recipient’s employment status: recent work
experience, a health problem, two or more arrests in the past six years, and a child
care problem. Recipients with a childcare problem had only a 30% chance of
working 30 or more hours per week.
3.84 Spouses and partners can alter their work / non-work situations when their
partners becomes unemployed / injured, or work fewer hours than planned.
Known as “the added worker effect”
123 there is a tendency for other household
members capable of work to enter the labour market if the primary income earner
becomes unemployed. This occurs only at lower income levels. The more
financially attractive a husband’s compensation payments are for injury / health
disability, the more likely his partner / spouse is to remain at home to care for her
husband. Married women change their hours worked or decide to seek work
depending on the level of their husbands’ earnings, but on average husbands do not
respond similarly to their wives’ earnings.
124
(b) Job satisfaction
3.85 Job dissatisfaction also can create a barrier to return to work. A study in the
aircraft industry found that if a worker did not like their job or had had difficulties
with fellow workers or superiors, it greatly reduced the chances of the employee
returning to that workplace
125. The Texas Workers Compensation Commission
126 actually warns employers that “the stage is often set for extended lost time long
before any injury occurs…with adversarial relationships between supervisors and
employees…negative relationships with co-workers, disciplinary or pay issues,
workload concerns or job dissatisfaction that tend to interfere with or delay return
to work. An employee who is satisfied with his or her job and employment
situation is self motivated to return to work as quickly as possible”.
121 Geers 1992 p 62
122 Mathematica Policy Research
123 Gardner John A p 56
124 ibid
125 Hendler: website: <www.mensanaclinic.com/articles/return_to_work_barriers.htm>
126 Texas WCC website: <www.twcc.state.tx.us/commission/divisions/rtw>
Page 26 of 144
link to page 28 link to page 28 link to page 28 link to page 28
3.86 A recent New Zealand survey found that just over half the employees surveyed
complained about their bosses, saying that poor management was a bigger bugbear
than poor salary, hours worked, work environment or job prospects.
127
(c) Job history
3.87 American research found that most workers with at least one year’s job tenure
returned to their pre-injury employer, but for those who did not return, the
duration off work was lengthened by a factor of 2 – 3. Workers at small firms
were much less likely to return to their pre-injury employer, thereby incurring
longer periods off work
128.
(d) criminal record
3.88 People with criminal records face a range of barriers to employment, depending on
what crime was committed. People with convictions for crimes against the person
are unlikely to get jobs in people related occupations such as education, healthcare,
passenger transport etc. People with convictions for theft are unlikely to get
positions where handling money or accounting is required. Even in occupations
that are not formally closed to ex-offenders, employers may screen out applicants
with criminal records.
129
3.89 Individuals with criminal records often have incomplete work histories, low levels
of education and little exposure to the norms and interpersonal relationships of a
typical work-place.
(e) obesity
3.90 Obesity can cause both real and perceived problems in returning to work.
Overweight people are subject to considerable discrimination in employment
decisions, as well as being stereotyped as emotionally impaired, socially
handicapped and possessing negative personality traits.
130 There is also evidence
that obesity hinders the ability of long term unemployed people to undertake
employment with physical activities, not least because the person may not have
maintained their fitness levels or stamina while being out of the workforce.
B External factors
3.91 Many of the problems experienced by long term unemployed or injured people
attempting to return to work are a result of factors beyond their immediate
personal control. This includes other people such as employers, case managers,
rehabilitation specialists, legal advisers etc and situational factors such as labour
market conditions.
Perception of employers / lack of knowledge
3.92 The principal reason cited by injured workers who were not successful in returning
to stable employment was that their employers either declined to re-employ them
127 Manual 2003
128 WCRI Research brief 1996 Vol 12 no 9 p 3
129 Brown 2001 p 82
130 Roehling 1999 pp969 - 1016
Page 27 of 144
link to page 29 link to page 29 link to page 29 link to page 29 link to page 29 link to page 29 link to page 29 link to page 29 link to page 29
(often on the grounds that no suitable work was available), or that the
accommodations they made for the injured worker’s disability were unsuitable.
3.93 Some employers Return-to-work programmes were seen as too aggressive, and
workers felt they were required to return to work too soon. Employees had
negative perceptions that some Return-to-work programmes were designed more to
reduce companies’ workers’ compensation costs than assist the workers
131. One
study reported that 40% of workers who had never worked again after their injuries
had sought re-employment with their pre-injury employers, but were rejected
132.
3.94 Employers can use the duration of unemployment as a signal of worker quality: the
longer the duration, the poorer the inferred quality
133. British employers wanted
the government to reduce the risks to them of recruiting long term unemployed
people
134 whom many perceived as high risk with potentially detrimental
commercial implications. While they reported some unfavourable experiences,
those who considered themselves socially responsible were more positive towards
those unemployed people they considered had used their time productively or who
they perceived as motivated and actively seeking work.
3.95 American employers often regard new hires as probationary
135, and are quick to
dismiss those in low wage jobs for early mistakes made, knowing that there is a
ready supply of replacement applicants with the minimal skills required for the job.
They expect employees to adhere to work schedules, to be punctual, to notify
supervisors of absence through illness, to accept authority gracefully, and to be
accommodating towards customers. Failure to meet these norms can limit job
tenure. Because long term unemployed workers are unaccustomed to these
demands, and some employers enforce them rigorously, dismissals resulting from
unacceptable behaviour can be attributed to shortcomings in both parties.
3.96 Related to this is the worry about discrimination from employers
136. Many
American studies reported different groups experienced discrimination as they
attempted to gain (re-)employment, and these people carried fear of that experience
recurring as they continued their attempts to get jobs.
3.97 Employers also have concerns about their ability to communicate effectively with
people with disabilities, as well as being unfamiliar with the disability and
discrimination legislation
137. This is especially true of hidden or learning
disabilities. This lack of knowledge causes employers to hesitate to discuss the
true needs of the individual with them.
138 For example, some managers are afraid
to ask interview questions that need to be asked if applicants with disabilities really
are going to be considered for job vacancies. Potential employers need to feel
reassured that the applicant is physically able to perform the job’s functions.
139
131 Manitoba League of Persons with Disabilities: Executive Summary
132 Butler, Johnson and Baldwin 1995 pp 72 - 84
133 Borooah, Vani K: 2000 pp3 - 25
134 Snape 1997 Executive summary
135 Hershey and Pavetti, 1997 p 78
136 Kalil et al August 2000 p 20
137 Bunch and Crawford 1998 p 49
138 de Jonge, Rodger and Fitzgibbon 2000
139 Pimentel (undated)
Page 28 of 144
link to page 30 link to page 30 link to page 30 link to page 30 link to page 30 link to page 30
Job adaptations
3.98 Job adaptations provided by employers are important determinants of long-term re-
employment following a workplace injury
140. Benefits include more stable work
histories post-injury, and employee loyalty. Expensive accommodations are rarely
needed by workers with disabilities
141. According to one study, about half of the
accommodations made by employers cost less than US$500 to implement
142
3.99 Despite anti-discrimination legislation in the United States, many employers either
do not, or are not required to, because of small size of the company, make any
accommodations for their injured workers, even though the injuries occurred at
their work-sites. Almost without exception, the workers whose employers
declined to, or were unable to, make any accommodations at their work-site took
longer to return to work, if they returned at all. A British study
143 found that over
one quarter of disabled people who left their jobs because of their disability would
have stayed in work if they were offered adaptations. Fewer than one in five were
actually offered any accommodations. Accommodations include lifts and handrails,
special equipment, and flexible working arrangements including breaks outside the
normal tea and lunch breaks.
144
3.100 Where adaptations are supplied to injured or disabled workers returning to
employment, the non-material adaptations are shown to be more important. A
Dutch study
145 of adaptations provided to both blue and white collar workers
indicated that physical adaptations were very minor compared with other changes
for disabled workers returning to work:
•
Changes in tasks and work content, whether with the pre-injury or other
employer (70%);
•
Change in duration of working hours, such as reduction or elimination of
night working, more regular working hours, reduced working day or
working week, shift changes and rest period (48%);
•
Reducing tempo / speed of work, such as reduced productivity targets, help
from colleagues, self-organised work patterns (41%);
•
Purchase of special devices, such as wheelchairs, transport to or from the
workplace (10%);
•
Training / vocational training, job coaching (7%);
•
Adapting tools / equipment / workstation / lighting / buildings etc (4%); and
•
Other, including help at home in order to get to work, changing the
workplace culture (14%).
3.101 A hidden barrier when injured / disabled workers are having adaptations made at
their workplace is that focusing solely on the technological / physical
accommodations was not enough to ensure success. An Australian study of people
with severe disabilities using computer and technological assistance showed how
140 MLPD: 1999
141 Unger and Kregel 2003
142 Job Accommodation Network
143 Meager et al 1996 Executive summary
144 ibid
145 Nijboer, Grunemann and Andries: 1993
Page 29 of 144
link to page 31 link to page 31 link to page 31 link to page 31 link to page 31
important it was to balance the employer’s and employee’s personal preferences,
and the work environment in order to achieve maximum productivity and
satisfaction.
146 It could be said that this is true of all employment situations.
Case management/ rehabilitation issues
3.102 The case manager and/or the vocational rehabilitation counsellor can have
significant impact on whether clients manage to regain and retain employment.
Rehabilitation counsellors were found to favour negative client factors, such as
incapacities, over the positive factors, and an overemphasis on client incapacity by
rehabilitation counsellors may restrict access for people with disabilities to
employment opportunities
147. Other research has identified the importance of
“client optimism” as a key psychological factor associated with successful return to
work outcomes for people with disabilities.
148
3.103 Setting goals is fundamental to the case management process: case manager and
client identify specific long-term goals and then break them down into the
incremental behaviours required to achieve each goal
149. Kisthardt et al,
150 during
case management training, identified four factors why goals might fail: behavioural,
cognitive, affective, and environmental. All of these failures relate to the case
manager / client interaction.
(a) Behavioural dimension
3.104 Goal-directed activity requires the ability to engage in a series of specific
behaviours, and the level of competency and skill involved in achieving the goal is
paramount. Goal attainment may fail if the individual lacks the required skills to
achieve the goal. Skills required include communication, reading, and filling out
forms, as well as managing activities of daily living. Attempting to achieve too
many goals at once can diffuse the activity and limit the achievement of any, or all,
or the goals. Clients frequently require assistance in prioritising goals and
activities.
(b) Cognitive dimension
3.105 Frequently, clients have not signed up to the identified goals. Case managers
report that clients agree with the goals and then proceed to sabotage them by not
following the agreed action plan. This may reflect more on the client’s lack of a
sense of ownership of the goal than on resistance to treatment or denial of what
they need to do.
3.106 People may also change their minds, as circumstances or personal desires change,
and a goal become meaningless and irrelevant. While this is a normal part of daily
living, some case managers see it as pathological. People may lack the knowledge
and information required to complete a task, but many professionals often assume
that clients have all the knowledge. Lastly, the client’s knowledge of previous failed
attempts may lead to them “talk themselves” out of achievement.
146 de Jonge, Rodger and Ftizgibbon
147 Strohmer, Pellerin and Davidson 1995 pp 82-93
148 Chapin and Kewman, 2001 pp 400 - 416
149 Kisthardt, Gowdy and Rapp: 1992 p 117
150 ibid p 118
Page 30 of 144
link to page 32 link to page 32 link to page 32
(c) The affective dimension
3.107 Goal-directed behaviour is influenced by and in turn influences the way people
feel. Success or failure depend on their feelings of satisfaction, accomplishment,
fulfilment, or joy. When people begin to feel overwhelmed in the process of goal
attainment, they may seek to change direction.
3.108 The affective dimension is also apparent when goals are set too high or too low,
when too many goals are set, and clients feel they are over-extended. Clients may
also fear the results of success such as moving from the security of benefit to
earnings. This may lessen their enthusiasm or commitment to pursue the goal.
Lastly, feelings of loneliness, fear and isolation can effectively block a client’s ability
to engage in goal-planning and attainment.
(c) Environmental
3.109 Goal attainment may fail if the necessary resources are not available, accessible or
accommodating for a person’s needs. These resources include social resources such
as people, goods and services such as money, transport, and housing. Often these
resources are available and accessible but neither the case manager nor client is
aware of this.
Lawyers’/ advocates’ attitudes
3.110 Research consistently shows that those who challenge decisions regarding their
unemployment or injury compensation entitlements are unlikely to return to work.
In Britain, those who appealed against the decision to cease giving them the
incapacity benefit were found to be particularly unlikely to re-enter the job market
(one in ten found work), compared with those who did not appeal (four in ten
found work) and those who left the benefit voluntarily (seven out of ten found
work). Litigation is a negative factor for patients rehabilitation / managing pain /
returning to work
151. Any unresolved conflict between the patient and any one
associated with the injury may present a significant barrier to rehabilitation.
3.111 One study found that patients who believe they are entitled to financial reward
because of an accident have little desire to recover quickly, especially when
attorneys have successfully sued for and put a dollar value to their pain an
suffering
152. When a client’s lawyer advises non co-operation and the fostering of
an adversarial relationship, this works against a client’s rehabilitation and their self-
esteem, and their ability to participate meaningfully in society.
153
3.112 American experience is that too many lawyers are willing to raise adversarial
matters which stand in the way of achieving the vocational rehabilitation plan,
perhaps protecting their own interests rather than the clients’ interests. The
longer the dispute process continues, the less likelihood there is that any form of
151 Frederickson et al 1988 pp 351-3
152 McIntosh, Melles and Hall, 1995 p 199
153 Ehret 1988 pp11-12
Page 31 of 144
link to page 33 link to page 33 link to page 33 link to page 33 link to page 33 link to page 33
rehabilitation will be productive
154. The process of proving that one is totally
disabled may result in a self-fulfilling prophecy.
155
Focus on disability (rather than ability)
3.113 The generally negative results when a job-seeker does not maintain a positive
outlook has already been discussed. This concept is also true when a person is
labelled by their disability, whether by themselves or their family, a case manager, a
medical professional, a lawyer or advocate, their employer or work colleagues. “To
refer to a human being as a paraplegic, a manic-depressive…or a post-traumatic is
to elevate the deficit or deviance to the status of the dominant identity of that
person”.
156 Assessments and interventions based on such pathology-derived
definitions of persons and situations are more likely to perpetuate the pathology
than to modify it.
3.114 Ehret
157 expressed frustration at the NCCI Seminar on Legal Trends affecting
Workers Compensation that few compensation judges actually understand
vocational rehabilitation, and their decisions frustrate rehabilitation by allowing the
claimant to focus on continued disability rather than building on ability. These
negative perceptions create a significant barrier to achieving a successful return to
work.
3.115 The French agency which manages government activities in relation to
employment, training, financial and social assistance for disabled adults was
strongly criticised in the 1980s for its concentration on disability rather than
ability, which had reduced its efficacy.
158
Co-worker attitudes
3.116 Colleagues can create problems for injured workers or former unemployed workers
in retaining employment. These problems include:
•
the worker feeling stigmatised by having been a welfare recipient when co-
workers were unhelpful or unco-operative,
•
supervisors being impatient or not taking time to get to know the abilities of
the new employee,
•
difficulties understanding the work culture in the new environment, and
learning how to relate to people in the right way.
159
154 ibid
155 Marini 2003 p 42
156 Cohen: Intervention and supervision in strengths based social work practice
157 Ehret 1988 p 12
158 Thornton and Lunt 1997 p 95
159 DeBord et al: Executive summary
Page 32 of 144
link to page 34 link to page 34 link to page 34 link to page 34 link to page 34
3.117 Some injured workers report problems with co-workers who are unaware of the
employers’ responsibilities to accommodate injured workers, or did not understand
the limitations created by different injuries.
160
Transport issues
3.118
Transportation costs are often ignored as one of the costs of, and therefore a
barrier to, re-employment, both in terms of time and money, such as for a parent
whose commute includes dropping off a child at childcare. British research on
ways to assist long term unemployed shows that those employers who provide
childcare support or transport for employees report higher employee retention and
improved work performance
161.
3.119 Other studies showed that without financial assistance in getting to work, the
health of many people with disabilities was jeopardised with the stress, risk and
fatigue of exhausting journeys, and their concentration and quality of work suffered
from worry and distraction. For those with developmental disabilities, transport
is the biggest barrier faced in obtaining work.
3.120 Seventy-seven percent of long term unemployed surveyed by the NZ Employment
Service study cited limited mobility as a key barrier to return to work
162. This
incorporated:
•
Having no driving licence;
•
Not having independent means of transport.;
•
Living in an area without public transport;
•
Being unable to move to an area where more jobs were available; and
•
Living in an isolated area.
3.121 The types of barriers varied markedly according to geographical regions: 60% of
survey respondents living in the Gisborne region reported having no driving
licence compared to only 1% of respondents in the West Coast of the South
Island.
163
Retaining employment
3.122 Butler et al
164 tested the long-held premise that when an injured worker first returns
to work after their injury, this means that they are then rehabilitated. Using data
about Ontario workers over a 14 year period, they showed that the effects of
injuries on employment are more lasting that previously considered: 85% of the
workers studied returned to work, but 60% of this group subsequently had one or
more injury related absences from work. Thus in the longer term, the success rate
was only 50%.
160 Sum et al 2001 p 38-9
161 Kellard, Adelman et al 2002 pp 35-7
162 NZ Employment Service 1996
163 Parker 1997 p 67
164 Butler, Johnson and Baldwin, 1995 pp 72 - 84
Page 33 of 144
link to page 35 link to page 35 link to page 35 link to page 35 link to page 35
3.123 Returning to work and keeping a job permanently are two entirely different
matters. In a Canadian study of 113 injured workers in 1995
165, 60% of
respondents had returned to work at least once since being injured, mostly with
their pre-injury employer, but more than half of these people were not working at
the time of the survey.
3.124 In another Canadian study 85% of the workers surveyed returned to work, and
could have been presumed recovered from their injuries
166. In reality, almost 60%
of those who returned to work had one or more injury-related work absences, (i.e.
50% of the survey population) leaving only 35% of the workers surveyed actually
returning to work and staying there.
3.125 While welfare reform world-wide has focused on moving beneficiaries from welfare
into employment, the real challenge emerging now is to ensure these people remain
employed. Just being back at work is a challenge for some newly employed
workers, with the need to work productively, maintain the required hours for the
job, and cope with a new work environment. “ Extensive on-going support is
sometimes needed to ensure the client remains in employment. Abandoning these
clients once they are in paid employment is likely to result in them becoming
unemployed again in a relatively short time”.
167
3.126 The transition to steady employment is often difficult and has many of the same
barriers as gaining re-employment. These include personal and family issues, low
paying jobs, and limited work supports as previously outlined. Given the
challenges that many welfare recipients confront in going to work, it is not
surprising that job loss is common, while steady, full-time employment occurs less
frequently. Many recipients lose their jobs quickly, and spells of unemployment
are often long. Repeated returns to benefits are known to have “scarring” effects
on people, and increase the likelihood of even further spells of unemployment in
the future
168.
3.127 Studies have shown that about one-quarter of (former) welfare recipients who
become employed stop working within three months, and at least half are no longer
working within one year. More than half the mothers surveyed in a New Jersey
study left their jobs for work related reasons, such as being laid off or fired,
receiving low pay or inadequate fringe benefits, disliking the job /its hours / its
location, or switching to another job. The remaining 43% cited personal reasons
such as pregnancy, health or family problems, difficulties with child care,
inadequate transportation, change of residence, termination of health insurance
cover, or incarceration
169. Most of these reasons are already widely acknowledged
as barriers to return to work.
3.128 Economic theory describes the
income compensated substitution effect, which is the
trade-off between increased desired working hours when wages increase against the
cost of using these hours for leisure purposes. For the largest group in the labour
165 Canadian Injured Workers Alliance, 1995 p 64
166 Butler, Johnson and Baldwin, 1995 pp 72 - 84
167 Wehipeihana p 22
168 Kellard, Adelman et al 2002 p 11
169 Thornton and Hershey 1990
Page 34 of 144
link to page 36 link to page 36 link to page 36 link to page 36 link to page 36 link to page 36
force, men aged 25 – 54, time spent working may fall as wages rise, because leisure
time is more desired than the goods that an increase in income can buy
170.
Self-employment
3.129 Both long-term unemployed and long term injured workers are interested in
becoming self-employed as a means of re-entering the workforce. The following
have been identified as barriers to entering and then sustaining self-employment:
•
Difficulties in obtaining start-up capital;
•
Fear of losing the security of benefit or compensation payments;
•
Unhelpful attitudes of advisers, regarding what types of work clients could
or could not undertake; and
•
Lack of access to appropriate training and support, including transport
issues.
171
3.130 In Britain disabled people with vocational qualifications are relatively more likely to
be self-employed, especially those with musculo-skeletal problems, and women
with mental health problems. The types of self-employment undertaken by
disabled and non-disabled people were similar. While earnings from self-
employment are notoriously difficult to measure, when comparing the average
earnings of disabled and non-disabled self-employed people using the same
measures, self employment generated significantly less income for disabled than
non-disabled people.
172
3.131 Views on whether and how disabled people can achieve self-employment vary
widely between vocational counsellors in America, with considerable disagreement
as to the efficacy of self-employment for the self-sufficiency of disabled people, and
mistrust of the business community.
173 Access to traditional business services and
supports is blocked by stereotypes and an absence of creativity. Decisions about a
person’s capacity to sustain self-employment are generally based on assessment of
their disability, rather than on sound business factors. In many cases, it is seen as
the option of last resort.
174
Labour market conditions
3.132 The process of moving into work reflects a complex blend of three principal
factors: personal characteristics of the job seeker, state of the labour market, and
the job / employer. For those who have been out of work for a long period,
regardless of cause, the state of the labour market can have real and perceived
effects. Some researchers cite that poor labour market conditions are directly
associated with an increase in disability benefit applications
175. Labour market
barriers include the availability of work, location, hours or work, and prevailing
financial rates of unemployment / compensation benefits.
170 John A Gardiner: Return to work incentives
171 Boylan and Burchardt, 2003 Executive summary
172 ibid
173 Rizzo 2002 p 97
174 ibid p 98
175 Tate 1992 p 17
Page 35 of 144
link to page 37 link to page 37 link to page 37 link to page 37 link to page 37 link to page 37
3.133 Many industrially injured people are employed in occupations in sectors which are
undergoing substantial changes, resulting in fewer available jobs, and additional
requirements for education. Often these industrial workers have lesser work related
qualifications due to limited education. Additionally, their pre-injury work
experience is likely to be in occupations with high unemployment rates (such as
unskilled manual labour or manufacturing). Those who lose their jobs through
injury have a higher probability of remaining unemployed
176.
3.134 The labour market also encompasses hours of work. Internationally, there has
been an expansion of part-time, short-term, contract and other sorts of casual
labour. It is reported that in Canada over one third of part time workers would
prefer to be in full time employment, and that two fifths of the Canadian labour
market is not full time work
177.
3.135 Income assistance recipients should always be better off, not worse off, by working
rather than remaining unemployed, if there is to be any prospect of their seeking
and retaining employment. British research
178 showed welfare recipients rejecting
lower paid jobs without career prospects. The young welfare recipients rejected
jobs on the grounds that such jobs lead nowhere. Their older counterparts rejected
jobs which compared unfavourably with their previous work, being low status,
unfulfilling or even illegal.
3.136 The higher income benefits are relative to what a person could earn in the labour
market, the stronger the economic incentive to choose the benefit rather than to
work. Researchers estimate that a 20 percent increase in benefits will increase the
average duration of temporary disability by 4% and permanent partial disability by
3 %. Studies show that low-income individuals are more likely to stop working
completely when disability benefit levels increase while others show that limits on
the duration of benefits can create return to work incentives.
179
Compensation entitlement
3.137 Australian, British and Canadian research indicates that people with back injuries
return to work much more quickly if they have no compensation entitlement.
180 181
One study showed a very large difference in the rates of return to work for two
groups of 70 patients with back injuries, one entitled to compensation, the other
not. The median time off work for the former group was twelve months, and for
the latter one week. In that the latter group would be returning to work from
economic necessity, it could be surmised that they would be likely to be more
disabled and experiencing more pain than the compensable patients, but the
reverse is the case. When the median Pain, Disability and Impairment Scores of the
two groups were compared, the non-compensable group showed much better
health status. It could therefore be asserted that in New Zealand, where
compensation is payable regardless of where the injury occurred, this is in itself a
barrier to employment.
176 ibid
177 Bunch and Crawford 1998 p 26
178 Shaw et al 1996 p 75
179 Gardiner 1989: p xiii
180 Greenough and Fraser: 1988 p 954
181 Johnson, Baldwin and Butler 1998 p 28
Page 36 of 144
link to page 38 link to page 38 link to page 38 link to page 38 link to page 38 link to page 38 link to page 38
3.138 Other researchers
182 found that workers compensation benefits actually encouraged
a slower return to work after surgery / injury. “There is no question that the large
disincentive effects of workers compensation disability payments reflect the relative
ease with which back pain can be overstated by patients seeking disability benefits
and time off work”.
183
3.139 In a lump sum settlement, the claimant settles their future compensation benefits
for a lump sum of money. The benefit to this settlement is that the injured worker
can take a lump sum of money and get on with their life. There is a perceived
perverse incentive created by lump sum compensation which motivates an injured
worker to focus on their disability until settlement has been reached, rather than
focus on rehabilitation. Anecdotal evidence that workers do improve markedly after
receiving lump sum payments is supported by studies.
184
Concluding remarks
3.140 American studies found that welfare recipients often have multiple barriers and
liabilities to gaining employment and that the likelihood of employment decreases
as the number of liabilities increases. A multi-variate analysis predicted that the
welfare recipients with no employment liabilities had a 58% chance of working 30
hours or more per week, and this dropped to 33-35% if they had up to three
employment liabilities.
185
3.141 Except in the most severe cases, the direct physical effects of injury do not
completely determine whether an injured worker returns to stable employment
186 Instead patterns of post-injury employment are determined by a set of influences
that include workers’ characteristics and workplace accommodations that offset the
limiting effects of impairments. Successful disability management requires a
combined effort by all interested parties: employers, insurers, unions, and workers.
3.142 Injured workers at greatest risk of employment instability are female, have below
average education, have a back injury, and do not receive job accommodations
from their employers
187. Getting long term unemployed back into work remains
one of the most serious and intractable problems facing the EU today, and the
debate for them is where should the policy intervention lie
188. There are two
options:
•
Making the long term unemployed more employable by giving them
education and training in the areas identified above; or
•
Finding jobs for them, and putting the emphasis on inducements for
employers, with the expectation that the desired employment attributes will
be developed .
The major handicap for the long term unemployed is that they are unemployed.
182 Filan: The effect of workers’ or Third party compensation on return to work after hand surgery
183 Johnson, Baldwin and Butler 1998 p 28
184 Greenough and Fraser 1988 p 947
185 .Kirby, Fraker, Pavette and Kovac: June 2003 Executive summary
186 Butler, Johnson and Baldwin, 1995 pp 72 - 84
187 ibid Summary
188 Borooah, 2001 p 5
Page 37 of 144
link to page 39
3.143 Two studies on the results of probably the largest and most complete survey of
injured workers ever conducted, by the Ontario Workers’ Compensation Board,
indicate the following:
•
The majority of permanently impaired workers returned to their pre-injury
employer, generally receiving the pre-injury wage as well as adaptations to
facilitate their return to work; and
•
Those impaired workers who moved to a different employer earned wages
significantly lower than their pre-injury rate.
3.144 What is less reported is that both sets of workers experienced extremely high initial
rates of turnover
189. While the workers claimed that they were “physically unable
to do the job”, there was insufficient data or analysis to demonstrate that there was
a deterioration of health relative to that which existed at the time of re-
employment. Rather, it was hypothesised that employers retain injured workers
with some uncertainty about their abilities to perform full duties, and when
productivity does not improve at the end of any “probationary” period, the
employment relationship is terminated. The conclusion therefore should be that
paying more attention to dealing with the non-injury issues would have greatly
reduced these problems. In other words, had the barriers faced by long term
unemployed workers returning to work (as outlined above) been addressed, many
more of these workers would have retained sustainable employment.
189 Cater 2000 p 76
Page 38 of 144
link to page 40 link to page 40 link to page 40
4
Part 3: Programmes and initiatives to remove barriers
4.1
Many countries have grappled for decades with the problem of moving people from
welfare to work, whether they are unemployed or disabled. A wide variety of
programmes have been initiated, debated, reviewed, rejected and re-instated.
Creating effective return to work programmes for unemployed or injured / disabled
workers is easier said than done. Many supervisors would rather not take injured
or disabled workers back on a modified duty basis, preferring to wait until workers
can perform their regular jobs. For some employers, the nature of the work or the
workplace can present obstacles to developing safe modified work alternatives. The
state of the economy has an impact – many employers struggle to retain fully
functioning staff let alone accommodate workers with impairments.
190
4.2
This section reviews some return to work initiatives and evaluations which have
been undertaken. It also includes actions which can be taken by individuals, case
managers or providers to address individual barriers.
Addressing length of time out of the work force
(a) Unemployed
4.3
Return to work programmes for unemployed people fit into two categories
addressing:
•
Workers made redundant / facing retrenchment. The benefits of returning
these people to employment as soon as possible are well recognised, as are
the difficulties in maintaining their work skills and commitment in the
absence of employment. Those who do not return to work promptly risk
lapsing into the second category below, or long term unemployed; and
•
People in receipt of welfare payments, many of whom may be long term
beneficiaries, and thus requiring quite different forms of assistance.
4.4
The various programmes and initiatives dealing with early return to work are, in
general, established return to work programmes but implemented at specific
appropriate times, such as when notice of redundancy or retrenchment is given,
and before a worker ceases employment with that employer.
(b) Disabled / injured workers
4.5
Return to work is cited as probably one of the best aids to recovery and to
preventing the patient’s deterioration into chronic disability. In Britain, the best
clinical management for back pain is to continue an active life rather than waiting
till the pain disappears completely: this will mean faster recovery and fewer long
term problems.
191 An important conclusion of an Australian study was that back
injury patients are in general likely to benefit because of, rather than in spite of,
returning to work.
192
190 Kremer 2003 p 39
191 Waddell and Burton: Occupational health guidelines for the management of low back pain.
192 Gun and Fraser 1992 p 4
Page 39 of 144
link to page 41 link to page 41 link to page 41 link to page 41 link to page 41 link to page 41
4.6
An early return to work is considered a major objective of cardiac rehabilitation for
most people of working age.
193 For people with mental health problems, working
aids their confidence, motivation and future health.
194 Melhorn
195 found that
having no lost workdays or returning to work early (within 15 working days) was
the most important element of “work survivability” (retaining employment for at
least two years after the injury).
4.7
Early Return to Work programmes for people recovering from illness such as
strokes or from an injury cover a range of actions, including:
•
Modified / lighter duties;
•
Reduced hours;
•
On job support; and
•
Retraining.
4.8
Facilitating early return to work has become a major policy goal in Sweden, with
the responsibility placed squarely on employers and employees. This is achievable
as 75% of employees work either for large companies with on-site medical staff or
for a company with an affiliation with a medical centre.
196 This includes
maintaining personal communications with the injured workers during the
hospitalisation / recovery phase, which is seen as a positive action by both workers
(who like the personal touch) and case managers (who see it as motivational).
4.9
Programmes to help long term unemployed return to work are covered in the
programmes and initiatives listed below.
Addressing the concept of disability
4.10 However one defines disability, it is clear that the population of people with
disabilities is diverse. People with disabilities, by and large, have more in common
with the general population than with each other. In Canada, the focus has been
shifting from the provision of specialised services for people with disabilities to the
use of mainstream services, programs and facilities. This is in part because the
disability “system” has become fragmented, often with a lack of co-ordination.
197
Disability specific services are often needed only when regular programmes are
unable or unwilling to accommodate people with disabilities.
4.11 Higher individual satisfaction and quality of life occurs when people with
disabilities are able to make use of generic programmes and services in the
community.
198 In general, the commonest impediments to the employment of
people with disabilities are non-employment issues, such as transport, education,
training, and on job support, or personal attributes and attitudes. These are
addressed in the programmes listed below.
193 Jones and West: Cardiac Rehabilitation
194 Duckworth: Disabled person’s perspective.
195 Melhorn 1996 p 63
196 Sim 1999, p 45
197 Perrin 1999 p 14
198 ibid p 122
Page 40 of 144
link to page 42 link to page 42 link to page 42 link to page 42
Addressing personal issues
(a) Personal responses to stressful life events
4.12 To understand work-related stress, we must first consider stress itself. Every-one is
under stress – there is no such thing as a stress-free life, or a stress-free job. Every-
one is exposed to daily pressures, and most people cope with, even flourish on,
moderate amounts of stress without suffering any ill effects. If people feel that in
control, stress can be experienced as a challenge, which drives them to perform
well.
199
4.13 The principal difference between healthy challenge and unhealthy stress is the
reality or the perception of the person being able to control or influence the
outcome. When the sense of control is lost and coping mechanisms break down, a
potentially healthy challenge can become dangerous stress. Unrecognised and
untreated, this stress can affect work productivity and attendance, attitude as well
as physical and mental health.
4.14 There are two types of programmes teaching stress management techniques:
problem focused coping and symptom focused coping. Problem focused coping
techniques aim to control or eliminate the cause of stress, while symptom focused
coping techniques include activities to alleviate the consequences of the stressful
event but without addressing the actual problem.
200
4.15 In dealing with job loss, the commonest problem focused techniques include job
search activity, retraining, or even geographical relocation to obtain re-
employment, and these are judged fairly effective in succeeding (mainly because
these sorts of strategies open up additional opportunities for jobs). These activities
may however themselves cause further stress, and require some symptom focused
techniques as well. Both types of coping techniques are important, and if used
properly, can have very beneficial consequences for physical and mental health.
201
4.16 Training in stress management is widely available in books, on cassette tapes,
videos, training courses, and on the Internet, in whatever format the potential user
would like. It was therefore surprising to find very little mention of it in the
various international programmes to help either long-term unemployed or injured
workers return to work.
4.17 Job-search Clubs are cited as a good means of reducing stress (as well as assisting
attendees to find jobs).
202
(b) Response to negative experiences
4.18 Responses to negative experiences can include a progression through shock,
frustration, discouragement, self-blame, low self-esteem, lower expectations of
outcomes, and even learned helplessness. Unless preventative action is taken at the
time of the negative event, and it is successful, many people will reach a level of
negativity which is hard to move.
199 Pimentel 2001
200 Leana and Feldman 1995 p 1384
201 Susan Folkman in press release 4 December 2002 on death of Richard Lazarus
202 Bayer 2002 on www.fiveoclockclub.com
Page 41 of 144
link to page 43 link to page 43 link to page 43 link to page 43 link to page 43
4.19 A series of American studies has shown that patients who engage in forms of denial
(of the seriousness or even the existence of a medical problem) recover better and
more quickly from surgery than patients who do not. While this is contrary to
orthodox wisdom, it is now proven that false beliefs can have very beneficial
consequences to health and wellbeing. The same authors, however, cautions that
denial can be destructive to the denier, in that it may prevent seeking appropriate
medical attention, and reduce the value of any rehabilitation.
203 In some situations,
those in denial may be family and friends (such as those who supply alcoholics
with alcohol), or even rehabilitation professionals, who are unable to help a patient
facing a bleak and depressing future.
4.20 Interventions helpful in denial situations include:
•
Counselling tools such as unconditional positive regard, accurate empathy,
and confronting;
•
Accepting the client as an individual;
•
Relationship building, recognising the client’s anxieties;
•
Helping the client understand the denial and its underlying cause; and then
•
Helping the client eliminate their denial.
204
4.21 The power of positive thinking is a well established and successful concept, but one
difficult to impose on another party at the time of a negative experience. Most
programmes to assist long term unemployed return to work include training in
aspects of positive thinking, such as developing self-esteem, although this is
generally more difficult to accomplish at that time.
4.22 Learning how to handle the negativity has proved to be a successful concept in a
Canadian study of unemployed managers who had given up seeking employment,
but who had previously had job search training. The managers were taught how to
deal with repeated rejections in job searches and this helped them develop a
positive attitude, that they could and would succeed in their job search.
205 In
Michigan, it is described as “fortifying the job seeker’s ability to resist
demoralisation”.
206 There are various ways of achieving this.
(c) Loss of status
4.23 Addressing the concerns about status is a difficult issue, as this concern generally
reflects attitudinal or personality traits, financial requirements and commitments,
lack of confidence or fear for the future, or an underlying desire not to return to
work. Achieving a job with the same status may not be possible due to the
vagaries of the labour market, attitudes of employers, location, and the skills of the
worker becoming outdated ( as happens very quickly in the information technology
(IT) industry). In general, it is a male problem, as men often measure themselves
by their professional achievements: their sense of self-worth is directly linked with
their job satisfaction.
207
203 Lazarus 1983 pp 1 - 30
204 Stewart and Gomez p 5
205 Millman and Latham p 95
206 Caplan, Vinokur and Price 1997 p 343
207 Bayer Press release 2002
Page 42 of 144
link to page 44 link to page 44 link to page 44 link to page 44 link to page 44 link to page 44 link to page 44
4.24 In some cases, whether in the same or a new industry, the worker needs to restart
at a lower level on the career ladder than pre-injury / pre-unemployment. In the
IT industry, the worker needs to regain employment at any level, simply in order to
maintain their skills and keep up to date with new developments.
208 Although it
can be more stressful seeking better employment while already working, it is
generally agreed by recruitment specialists that it is easier for a person to get
another job when they already have one. This can provide the proof of up-to-date
job skills.
4.25 If a worker does take a lower level job, it can be tough on both self-esteem and ego.
Explaining on a curriculum vitae (CV) the presence of low level jobs in the middle
of an executive career is often difficult and undesirable. The CV could be
formatted around functional activities and achievements, rather than a
chronological list of jobs. In the current flexible labour market, gaps in careers are
not unusual, but the important issue is to retain polished skills.
4.26 Human Resources Development Canada indicates that it is quite normal for a
person looking for gainful employment to start with high expectations, leaving
room for later concessions to lower level employment.
209 This is corroborated by
staff at employment agencies.
210
(d) Lack of confidence
4.27 The likelihood of gaining re-employment depends more on having the self-
confidence to seek out jobs than on the actual skills used in doing so. Those with
an inner confidence in their ability to handle difficult situations return to working
life faster than those who expect others to help them through their difficulties.
211 Cognitive behavioural training programmes have proved successful such as one
where participants were trained in assertiveness, networking and contact building
skills to build their self-esteem, self-efficacy and confidence. Their mental wellbeing
improved – and nearly half the group also found a job.
212
4.28 The Prince’s Trust in Britain was established to help young people aged 14- 30 to
develop confidence and skills in order to get into work and start their own
businesses. The major programme is a 12 week programme to develop the
participants’ confidence, motivation and skills through teamwork in the
community. Over 73% of the 74,000 participants since 1990 have found work or
entered full time education or training.
213
4.29 The Lone Parents Organisation actively encourages lone parents to return to part
time work so to polish their social skills, develop self-discipline and confidence,
and the ability to judge how much stress they can efficiently work with before
tackling the challenge of full time employment.
214 This was to help them avoid the
syndrome that many long term lone parents who returned to full time employment
ended up back on benefits within three months. The Lone Parents Organisation
208 Southgate 2003
209 website: www.hrdc-drhc.gc.ca
210 Graves 2003
211 Millet Swedish National institute for Working life Newsletter No 3 2001
212 Proudfoot et al 1997 pp 96 - 100
213 The Prince’s Trust Factsheet June 2003
214 Lone Parents’ website: www.lone-parents.org.uk
Page 43 of 144
link to page 45 link to page 45 link to page 45 link to page 45
web-site provides a comprehensive “self-help diary” designed to build self-esteem,
confidence and social skills.
4.30 Germany established a system of social enterprises in the early 1980s, which
provided both employment and developed the confidence of the workers.
215 Known as “self-help firms”, they provide normal jobs with regular contracts and
wages for people with disabilities (generally with psychiatric disabilities) in firms
where non-disabled people are also employed. The firms are generally small,
employing up to 20 workers. Studies show that about 40% of employees with
disabilities moved through these firms to become employed in the general labour
market, while there was a drop-out rate of 20%.
216
4.31 The JOBS trial at the Michigan Prevention Research Center introduced a unique
feature in its programme to assist the unemployed: the trainers for the programmes
are themselves recruited form the ranks of the unemployed. Such people are
typically counsellors or teachers, and those with social and emotional competencies
themselves, such as flexibility, empathy, self-confidence and positive outlook.
They also have good speaking and listening skills, facilitation skills, and the ability
to manage conflict constructively. They undergo their own specific training.
217
(e) Apprehensions regarding re-employment
4.32 The transition from welfare to work is a stressful time for claimants, with fears
about coping financially, about re-injuring oneself, and the hassles of returning to
welfare if the job does not work out.
4.33 The British government has several programmes to ease the transition from welfare
to work.
218
•
The Job grant provides £100 for claimants moving off benefits into work for
at least 16 hours per week for a minimum of five weeks;
•
The Lone Parent Run-on gives a two week extension of welfare payments for
people moving into work who had been receiving benefits for at least six
months;
•
The Housing Benefit Run-on provides an extension of the Housing Benefit
for four weeks after the claimant leaves welfare for work. The claimant most
have been on welfare for six months, and have received a Housing benefit as
part of their payments. There is very similar Council Tax Run-on, a
Mortgage Interest run-on and an Income Support Mortgage Interest 52 week
link; and
•
Rapid Reclaim streamlines the process of reclaiming benefits for people who
returned to work that lasted for up to 12 weeks.
215 The concept of “work integration co-operatives” was first developed in Italy in the 1970s, when the
patients of a psychiatric clinic rebelled against working unpaid, and set up a co-operative to do the same
work under contract. The founders of the co-operatives were often parents, staff of the institutions, and
municipalities and local health or church organisations.
216 Thornton and Lunt 1997 p 134
217 Price and Vinokur 1995 pp 759 - 769
218 Woodland, Mandy and Miller 2003 p 8
Page 44 of 144
link to page 46 link to page 46 link to page 46 link to page 46
4.34 Behavioural and attitudinal change was positively associated with the amount of
anticipated financial assistance: as the amount of financial assistance increased, so
did the level of job search activity and the levels of confidence. A point of concern,
however, was that many potential recipients were unaware of their eligibility for
this assistance, and therefore the uptake was lower than it might have been. Poor
administration in some places reduced the beneficial impact.
219
4.35 The Job Grant was an unexpected bonus for most people, but was valued highly for
its psychological, as well as financial, effects. It provided much needed motivation
through to stability of household finances. For those who were expecting, any
delays in its arrival did cause financial problems, and lessened the benefit.
220 Newly employed workers who received the run-on payments were able to budget
more effectively, and expressed greater feeling of confidence. An appropriate
length for the transitional period was not established.
Personal abilities and attributes
4.36 Australian research on what employers want in their staff indicated personality and
attitude to be key attributes. Reliability was rated as the most important (at 66%),
willingness to work second (at 62%), and relevant work skills third at 52%.
(Relevant previous work experience was rated at only 40%, and presentation at
31%).
221 How to acquire these skills is addressed below.
(a) capacity to change
4.37 The capacity to change is seen as increasingly important as the nature of jobs and
the labour market continues to change. As the world of work is complex and
challenging, the Canadian government decided that the key skills needed for a high
quality work-force would be generic foundational skills rather than skills specific to
certain occupations, levels of responsibility or limited to today’s jobs.
They defined the Employability Skills Profile as:
•
People who can communicate, think, and continue to learn throughout their
lives;
•
People who can demonstrate positive attitudes and behaviours,
responsibility, and adaptability; and
•
People who can work with others.
222
All these attributes are deemed learnable, and can be learned at any age.
4.38 The concept of lifelong learning has been endorsed by the OECD as a means of
helping its member countries anticipate and benefit from economic and social
changes. Lifelong employability (defined as the capacity to be productive and to
219 Harries and Woodfield 2002 p 114
220 Harries and Woodfield 2002 p 108
221 Department of Employment and Work Relations 2001 p 2
222 McLaughlin 1992
Page 45 of 144
link to page 47 link to page 47
hold rewarding jobs during one’s working life) is no longer guaranteed by the
education and training received by people in childhood and youth.
223
4.39 Lifelong learning is far broader than “second-chance” education and/or training for
adults. It is based on the premise that every-one should be able, motivated and
actively encouraged to learn throughout life, through programmes such as Skills for
Life, unit standard based qualifications on the New Zealand National Qualifications
Framework, Internet based training or group courses.
4.40 Capacity to change incorporates adaptability, flexibility, versatility, resilience,
responsiveness, resourcefulness. It also incorporates attitude and/or state of mind.
4.41 David Noer, an international authority on the changing world of work, has defined
four types of individuals as they attempt to cope with change in a workplace or in
their own careers. These are posited around the individual’s capacity for change
and their comfort level:
Entrenched
Learners
ge
an 30 – 60%
10 - ? %
o ch
ty t Overwhelmed
BSers
aci
ap 30 – 60%
10 – 20%
C
Comfort level
4.42 Faced with an uncertain climate of rapid, unsettling change, both individuals and
organizations tend to react in predictable, self-defeating ways: they feel
overwhelmed and victimized, they dig in their heels and work harder as though
nothing's changed, or they try to fake their way along. According to Noer, the only
response that works is the positive willingness to learn and meet change head-on.
224
4.43 There are books, courses, and Internet based material available to help people
develop their attitude and capacity to learn. As with most skills, however, the
individual must have the willingness to learn before they will be able to learn.
(b) Personal expectations
4.44 Three critical internal resources are needed for an individual to cope with job loss
and /or stress. These are:
223 McKenzie and Wurzburg 1997 p 13
224 Noer 1999 Abstract
Page 46 of 144
link to page 48 link to page 48 link to page 48 link to page 48 link to page 48 link to page 48
•
Knowledge of the procedures that are effective in handling the stress – in
this case, how to find job leads, how to be interviewed;
•
Having the behavioural skills to use the above knowledge; and
•
Having the energy and motivation to put the knowledge and skills into
action.
225
4.45 Research shows that workers’ expectations of slower recovery or of greater
uncertainty in their future are consistently associated with longer periods off work
and receiving benefits.
226 This is a useful predictor of people who need additional
assistance in order to return to work.
(c) Education
4.46 Training programmes have proved successful in raising levels of literacy and
numeracy for long term unemployed. Part of their success is the provision of
ancillary services (which have already been identified in this report as necessary to
help achieve return to work) such as childcare, transportation, flexible hours for
training sessions. Improving the quality of trainers is important, as is using a
range of instructional approaches, and adapting the curriculum to ensure it is
relevant to participants.
227
4.47 Learning disabilities impact on the development of listening, reading, writing,
reasoning and numeracy skills. The US Department of Labor estimates that
between 50 and 80% of adults with low reading levels are “learning disabled”.
They present characteristics such as:
•
Difficulty planning and prioritising;
•
Using imprecise language or misusing terminology;
•
Writing illegibly; and
•
Having difficulty filling out forms.
228
4.48 The limited success of many programmes to develop basic education skills in
America has been attributed to not taking enough account of learning disabilities,
or the special needs of adult learners.
229 The Oklahoma Adult Education and
Literacy programme includes staff training in
•
Improving awareness and understanding of adults with learning disabilities,
and recognising the characteristics of learning disabilities;
•
Recognising self esteem and social skill issues and providing ways to foster
development;
•
Understanding the differences between screening, assessment and diagnosis,
and being able to apply appropriate screening; and
•
Using specific techniques for people with learning disabilities.
230
225 Caplan, Vinokur and Price 1997 p 353
226 Cole, Mondloch and Hogg-Johnson 2002p 750
227 Brown 2001 p 90
228 ibid p 89
229 ibid p 90
230 Brown 2001 p 94
Page 47 of 144
link to page 49 link to page 49 link to page 49
4.49 Recent research has identified that approximately 15% of employees spend time on
personal money matters on the job, and that negatively affects productivity. If
employees have control over their finances, they are less likely to be stressed, will
need less time to deal with their money matters at work, be more motivated and
have better morale than those with money troubles.
231 Comprehensive financial
education programmes have proven to be effective.
Financial education programmes typically include:
•
Understanding tax requirements;
•
Budgeting for items such as childcare or transport;
•
Savings and credit records;
•
Potential challenges such as credit cards, hire purchase, bounced cheques
and easy loans; and
•
Understanding financial institutions.
4.50 In Portugal, assistance is given to disabled people aged 16 or older to obtain a
professional qualification which will allow them to hold a job and to progress
professionally in- the normal job market. Such training can be on or off job.
232
(d) Ability to speak the local language
4.51 Language barriers can be removed or reduced with training. There are two subtly
distinct needs: ability to speak the official language of a country, and ability to
express oneself in words. American experience of running Job Clubs in different
languages is very positive
233. Incorporating teaching English as a second language
in work-skills or vocational training courses was also successful. In both examples,
the motivation and success of participants increased markedly.
4.52 Language may not be a barrier to obtaining some jobs (such as book-keeping), and
it may be a benefit to have speakers of other languages in jobs where staff interact
constantly with the general public (such as tourism / travel ).
4.53 The need to address cultural differences is not always recognised as a potential
barrier: in general this is best addressed at case manager level when following up
clients in their new employment. There are cultural assessment tools available,
such as that of the University of Michigan. It is designed to help providers
understand the beliefs, values and practices of clients and patients which may
impact on their care and rehabilitation. Issues to be considered include:
•
Level of ethnic identity;
•
Use of informal network and supportive institutions in the ethnic/cultural ;
•
Community values orientation;
•
Language and communication process;
231 Smart Solutions September 2000 Issue 4 p 2
232 Thornton and Lunt 1997 p 215
233 Brown 2001 p 97
Page 48 of 144
link to page 50 link to page 50 link to page 50 link to page 50
•
Migration experience;
•
Self concept and self esteem;
•
Influence of religion/spirituality on the belief system and behaviour patterns;
•
Views and concerns about discrimination and institutional racism;
•
Views about the role that ethnicity plays;
•
Educational level and employment experiences;
•
Habits, customs, beliefs;
•
Importance and impact associated with physical characteristics;
•
Cultural health beliefs and practices; and
•
Current socio-economic status.
234
4.54 Other strategies which have proven successful include:
•
Identifying jobs for which language is not a barrier, such as independent
work, account, and manual labour, and
•
Facilitate the interview process with interpretation and support;
•
Identifying jobs where another language is an asset, such as in tourism and
customer service positions;
•
Looking out for jobs where the supervisor is bilingual, or at least one other
staff speaks the same language;
•
Using job coaches to facilitate the transition to work; and
•
Promoting workplace training in ESOL.
235
4.55 It is important to include training in the “soft skills” required in navigating
workplace culture. Workplace simulations and role-plays of “sticky” situations
have proven successful in helping newcomers understand workplace cultures and
finding ways of fitting in without giving up one’s own identity or being taken
advantage of.
236
4.56 A listing of eleven good practice programmes identified consistent placement rates
above 80% and job retention rates between 60 and 90%.
237
Employability
4.57 While there are many programmes to assist unemployed workers develop their
employability, most of these address only some of the problems. Good examples
include the Canadian Federal Government’s Employability Improvement
Programme which has a client centred approach, and offers a flexible choice of
services including counselling, training and work experience. The project-based
training module provides integrated classroom and on the job training and work
experience. Project co-ordinators arrange appropriate employment activities which
may include skills training, life skills, job search and job placement. A review of
234 Isaacs and Benjamin 1991
235 Brown 2001 p 99
236 Wrigley et al 2003 p 23
237 Wrigley etal pp43- 62
Page 49 of 144
link to page 51 link to page 51 link to page 51 link to page 51 link to page 51 link to page 51
the programme in 1998 indicated that participants gained and retained
employment at higher income levels than previously experienced.
238
4.58 The Hong Kong Employees Retraining Board provides retraining courses and
services to enhance the employability of the unemployed and the potentially
unemployed. The Board supplies free full-time training courses, and heavily
subsidised part-time courses. Specifically at the request of employers, courses
include modules on “soft skills” such as work attitude, service culture, teamwork,
communications skills, and work commitment. They also cover basic computer
skills and occupational safety and health. A study in August 1999 of retrainees who
completed their training in January and February 1999 found that 84% were still
employed, nearly half of them with the same employer.
239
4.59 Employability skills can be taught and learned. Researchers have focused on
identifying successful practices in existing programmes and offer the following
conclusions:
•
Employability skills are best learned when they are included among
instructional goals and are explicitly taught;
•
Employability skills and traits are very amenable to being taught;
•
The best method is to raise consciousness about values, attitudes and
worker responsibilities, using strategies such as role play/ simulation,
problem solving, and group discussions rather than lectures;
•
Instructors should assume the role of facilitators / coaches so that students
take much of the responsibility for their own learning; and
•
Instructors should hold and communicate high expectations for the learning
outcomes, including punctuality, dependability, thoroughness, decision
making capability and co-operation.
240
4.60 There are many programmes available on the Internet for self-training in work
habits, attitudes and values, employability, or in affective competency for
professional training sessions. One example is the Denver Workforce Initiative,
whose
Workin’ it out programme helps entry-level workers understand the
unspoken rules of the workplace, and develop basic communication and problem-
solving skills.
241 Other American programmes for people with limited English
include training in cultural differences such as:
•
Intonation;
•
How to indicate you do not understand; and
•
How to fit in socially at work.
242
4.61 Part time work has been shown quite widely and consistently to prepare people for
future moves into full time work.
243 Researchers advise policy makers to consider
238 HDRC 1998
239 Kwong 1998 pp 1-6
240 Cotton 2001 pp 7-13
241 Relave 2000
242 Wrigley et al 2003 p 23
243 Evans et al p 107
Page 50 of 144
link to page 52 link to page 52 link to page 52
providing greater support for part-time employment because of these benefits.
Voluntary work is one good way of achieving this.
4.62 In Britain voluntary work is a permitted activity for people receiving incapacity
benefits. This is seen as helpful for people on the way into or back to work. It
provides opportunities to test interests and try out skills and to gain experience in
social interaction. As there is no direct effect on the level of benefit, it is also
perceived as risk-free.
244 Appropriate voluntary work included:
•
Helping children read at school
•
Community work
•
Assisting at play-centres or schools
•
Work in the office of a disability organisation
4.63 This voluntary work is required to have prior approval, but subsequent research
has shown a range of unapproved and unreported voluntary activities done by
beneficiaries “as a favour” or “just helping out”. These activities included:
•
Work for a residents’ association
•
Community support groups
•
Advocacy and self-help groups
•
Youth clubs
•
Driving elderly or disabled people
•
Performing arts
4.64 Working in charity shops was seen as retrograde and likely to inhibit
rehabilitation.
245
Addressing health factors
(a) Pain management
4.65 Pain management programmes were initiated in the 1970s. Typically they have
been multidisciplinary in nature, and the overwhelming majority have been based
on operant and cognitive principles.
246 Recent American programmes have been
more psychological in nature rather than merely exercise regimes. The relevance
of specific muscles is usually given less prominence than enhancing functional
activities.
4.66 Pain management programmes include:
•
Medication rationalisation and withdrawal;
•
Education about pain;
244 Corden and Sainsbury 2001 p 37
245 ibid p 38
246 Nicholas p 5
Page 51 of 144
link to page 53 link to page 53 link to page 53 link to page 53 link to page 53 link to page 53 link to page 53 link to page 53
•
Training in pain coping strategies (such as activity pacing, goal setting);
•
Relaxation techniques;
•
Turning unhelpful beliefs and thoughts positive,;
•
Upgrading more pleasurable activities; and
•
Encouraging the patients to take responsibility for managing their pain and
recognising their achievements.
247 This is especially important as research
shows that working with one’s own resources for pain management can be
an effective way of increasing self-confidence and thus improve motivation
to work.
248
4.67 Most programmes also include the involvement of family and friends, particularly
to educate them about refraining from unintentional reinforcement of pain
behaviours. The healthcare system can also reinforce negative pain behaviour, as it
provides services and attention contingent upon pain. Pain rehabilitation is likely
to be more effective, when it focuses on the positive.
249
4.68 Researchers generally agree that pain management is quite distinct from work
hardening (incorporating physical conditioning, work simulation, and education to
build strength and endurance, and improve function while helping to prevent re-
injury) and work conditioning (work hardening but without the educational
content).
250 Research on all three programme types indicated that programmes
which include a cognitive-behavioural approach can reduce the number of sick
days lost quite significantly for people with chronic back pain, but there was no
evidence of their efficacy for acute back pain.
251 252 Effective pain management can
also increase the general activity level of people, and thus their quality of life.
4.69 Cognitive behaviour therapy is an important tool in the rehabilitation of patients
with pain. It includes identifying and using all motivating factors for return to
work, as well as reducing the effects of demotivating behaviours. Motivation can
change the perception of pain, according to the “gate-control” theory.
253 According
to this theory, different aspects of an individual’s life can open or close the transfer
of pain signals. Cognitive factors such as increased concentration and motivation
may also help to close the “pain gate”.
4.70 Where pain management treatment programmes have been less successful may be
because the workplace was seen as “something to return to” rather than an integral
part of a comprehensive intervention.
254 Pain management programmes must take
account of both physical and psychosocial risk factors in the workplace (such as
high time pressures, monotonous tasks, job dissatisfaction, low social support).
247 ibid p 6
248 Gard and Sandberg (1998) p 101
249 ibid p 102
250 PTRC website www.ptrc-tx.com
251 Schonstein et al 2003 Abstract
252 Marhold, Linton and Mellin 2000 p 162
253 Melzack and Wall 1965 pp971-9
254 Marhold, Linton and Melin 2001 p 155
Page 52 of 144
link to page 54 link to page 54 link to page 54 link to page 54 link to page 54 link to page 54 link to page 54
(b) Use of cigarettes, drugs and alcohol
4.71 Studies have shown that between 6 and 37 percent of welfare recipients have a
substance abuse problem which interferes with employment and job retention.
255 Addressing substance abuse and mental health problems presents governments
with unique challenges regarding screening and assessment, service co-ordination,
treatment capacity, and funding for services. Access to treatment can be difficult
because service delivery systems are often fragmented. The solution to this is
interagency co-ordination.
4.72 In America, smoking cessation programmes are an allowable deductible medical
expense, as well as treatment and other costs related to alcoholism.
256
(c) Mental health
4.73 The need to prevent poor mental health while job seekers remained unemployed
has been firmly established in many studies such as in Britain
257 and in the United
states. In a Michigan study
258 results showed that intervention was particularly
beneficial for people at high risk of developing depressive symptoms. (High risk
was defined as having a high combined index of depression, financial hardship, and
low social assertiveness at first interview.) The high risk participants showed
significantly lower levels of both the incidence and the prevalence of severe
depressive episodes, even two and a half years after the intervention.
259
4.74 Most people who experience a traumatic event do not go on to suffer from post
traumatic stress disorder (PTSD), but many are likely to experience some of the
symptoms such as flashbacks or hyper-arousal. This is considered a normal
reaction in the short term, and for most people, such symptoms will reduce within
a few weeks. For most workplace traumas, fewer than 25% of the staff are likely to
be affected in the longer term.
260
4.75 Currently there are two main strategies for managing PTSD: diffusing and
debriefing. Diffusing is the term used generically to describe employees getting
together after an incident to discuss and make sense of what happened. In many
instances, this happens informally. The aim of diffusing is to help people come to
terms with what has happened, to offer reassurance and support, and to ensure
they are aware of other help available.
4.76 Psychological debriefing, a structured group process for reviewing events involving
intense re-exposure to the incident, is the most commonly used form of
intervention
261 and yet it is difficult to evaluate whether it is successful in reducing
trauma symptoms. There is a risk of secondary traumatisation with the intense re-
exposure to the incident. The benefits of debriefing were found to be the
development of management systems for dealing with incidents, and allowing staff
the opportunity to diffuse.
255 Danziger et al 2000 p 6
256 Krentzman 2003
257 Riddell 2002 p 45
258 Caplan, Vinokur and Price 1997 p 348
259 Caplan, Vinokur and Price 1997 p 348
260 Rick and Briner 2000 p3
261 Rick, Young and Guppy, 1998, Executive summary
Page 53 of 144
link to page 55 link to page 55 link to page 55
4.77 A series of British case studies found that organisations with a range of practices
and procedures for managing trauma in the workplace were less likely to have
incidents occurring and harm was minimised where incidents did occur.
262 These
include risk assessment, training and education, rehearsal of critical incident
procedures, clearly defined practices and policies for managing incidents, clear
guidance on dealing with the immediate aftermath of an incident, as well as longer
term support for employees.
(d) Evidence-based Return to Work Guidelines
4.78 Evidence based guidelines are derived from sources which pool reported cases and
compile data on various types of treatments, length of time off work, modified
work possibilities, and identify factors specifically impacting on return to work.
They have been derived to provide doctors, case managers, employers and workers
with realistic benchmarks for managing the return to work process. They are a key
factor in communications, ensuring that all share the same information and
assumptions. Research indicates that doctors appreciate having evidence based
guidelines to compare their patients with, as this enables them to come to their
own decisions rather than having some-one else’s view imposed on them.
263
4.79 Disability duration guidelines are the focal point of the return to work process.
Already, the use of such guidelines have produced significant and tangible results
across the board.
264 This includes a positive impact on the mental, physiological,
emotional and financial well-being of a worker, their family, co-workers, employers
and insurers.
Refusal to accept jobs
4.80 Whether unemployed people really want to work and the extent to which they
search for work has been the subject of much debate. Commitment to work tends
to be related to age (those over 55 years) and education (lower levels of education
reduces people’s longer term commitment to employment, especially women).
4.81 When dealing with refusal to accept job offers and options, it is important to
consider the reasons for the refusal. These include:
•
The remuneration is less than the person is receiving on benefit or through
compensation payments;
•
The worker wishes only to work in the same industry / the same type of job;
•
The person does not want to return to work;
•
Lack of confidence in their skills / ability to cope with work after an injury;
and
•
Loss of status.
4.82 How to address some of these reasons is dealt with elsewhere in this report (as in
dealing with the loss of remuneration, loss of confidence and loss of status).
262 ibid
263 Stutzman 2001 p 36
264 ibid p 38
Page 54 of 144
link to page 56 link to page 56 link to page 56
4.83 Researchers are divided on the effectiveness of requiring unemployed / injured
workers to accept job offers or lose their benefit payments. Knab et al found that
requirements to participate in mandatory welfare-to-work programmes can increase
employment and earnings, and reduce welfare income, independent of actual
participation in the programme. Usually these independent effects of participation
requirements are not known, because programme impacts are measured on those
who actually turned up to participate.
265 Not surprisingly, response to a mandate
increases with the strength of enforcement and the level of penalties for non-
compliance.
4.84 Most American states have laws saying that if a claimant for unemployment benefits
refuses an offer of suitable work, without good cause, the claimant must be
disqualified from receiving unemployment benefits. The British Government
believes harsh sanctions are necessary to break the cycle of benefit dependency and
long-term unemployment, which remain endemic in some parts of the country.
4.85 In 2001, nearly one in five children lived in a household where no one was in paid
work - double the proportion in 1979 and four times that in 1968.
4.86 The British Library Information Services states that the sanctions regime under
both the Jobseekers Allowance and the New Deal for Young People continues to
cause hardship to many unemployed young people who frequently have only the
haziest idea of what they have been accused. In practice sanctions were seen as the
sorts of things the powerful do to the socially excluded, and, because of this, they
have little effect on job-seeking behaviour. The most socially excluded among the
young unemployed appear to be the most likely to suffer sanctions.
266
4.87 Sanctions to force people to take jobs have been compared with healthcare: Imagine
a world where registering with your GP entailed signing a "healthseekers'
agreement" promising not to smoke, eat fatty food or go without exercise - and a
health service that would refuse to treat you if you had broken it, or, additionally,
failed to comply with a series of "for your own good" health and fitness measures.
There is no ethical difference between this scenario and that of the benefit
sanctions now in place: if we see healthcare as a universal social right, whatever
people's behaviour, surely a level of basic subsistence - the means to live - must be
too?
267
4.88 The Canadian government rules for benefits state that although a claimant is
expected to lower wage expectations as the period of unemployment lengthens, this
must not be taken to mean that the minimum wages paid in the labour market or
wages paid to an inexperienced worker become, at a certain point in time,
acceptable to any worker. In certain cases, employment at those wages is defined as
unsuitable; in fact, the "good employers", referred to in the legal provisions dealing
with refusal of work, generally recognise pay rates based on an individual's
qualifications.
4.89 They state that once a reasonable period of unemployment has elapsed since the
commencement of the benefit period, the claimant must be prepared to accept the
wage rates currently paid to workers in the same occupation and having the same
265 Knab et al 2000 p 20
266 Bivand 1999 pp12-15
267 Williamson Judith in The Guardian April 2002, available on www.societyguardian.co.uk
Page 55 of 144
link to page 57 link to page 57 link to page 57 link to page 57 link to page 57
qualifications. For employment opportunities in other than the usual occupation,
the claimant must be prepared to accept the rates paid to a person with similar
abilities; depending on the circumstances, they may mean the rates paid to
inexperienced workers.
268
4.90 The end solution is stated bluntly by recruitment specialists: “Today's job seekers
must lower their expectations. They need to commit themselves to working their
way up another career ladder, changing careers, taking part time positions or even
doing temporary work until a better position is found. They must change their
mindset and stop complaining that there aren't any jobs out there!"
269
Age, gender, ethnicity
(a) Age
4.91 Lifelong learning is an important part of British government policy, driven largely
by concern about the general skill and qualification levels of the economically
active population.
270 To remain competitive in the labour market, people need to
continually update and learn new skills, and it is recognised that participation in
learning has much wider benefits.
4.92 A British study of the impact of learning on older people concluded:
•
An improvement in self-confidence, self-esteem, satisfaction with life and
ability to cope with everyday life;
•
Improved ability to stand up for oneself;
•
Improved ability to take responsibility;
•
More people in poor health or disabled reported improvements in life than
those in good health;
•
25% declared they had done enough learning in their life; and
•
22% felt they were too old to learn.
4.93 Overall, this research supports the training / retraining of older workers for
employment. Another reason to support this training is a seemingly international
lack of the suitable skills for employment: the Hudson Institute forecast in the early
1990s that millions of new workers lack the basic skills essential for employment,
and that a gap was emerging between education and skill levels of new workers and
employers’ skill requirements. This was forcing employers to look to non-
traditional workers, finding in older persons “a vast resource of talent and
experience”
271
4.94 In Hong Kong, the Employees Retraining Board has special programmes for older
workers, originated through concern for the vulnerability of elderly workers with
low education attainment and low skills.
272 They see training and retraining as a
continuous and lifelong process for all.
268 HRDC Rule 10.5.4
269 Graves 2003
270 Dench and Regan 2000 Executive summary
271 American Association of Retired Persons 1993 p 4
272 Kwong 2000 p4
Page 56 of 144
link to page 58 link to page 58
4.95 Research has identified some best practice in training / retraining older workers,
which also includes placement in part-time employment. While there is no
consistent definition of the older worker, in terms of chronological age, functional
ability, and psycho-social characteristics, this merely serves to emphasise the
individuality of older workers and the need to be flexible towards training,
retaining and employment.
4.96 There are a number of research findings that indicate that being old may not be the
reason for someone being a poor learner, rather it could be due to learning and
other individual differences, such as not having been involved in learning activities
for some time.
273
4.97 Traditional training methodologies for older workers include:
•
Interactive training (based on the assumption that older workers do not
function well in school type environments);
•
Activity learning (which reduces descriptions and memorisation, and
involves tasks of graded difficulty, but results of studies were inconclusive);
•
Discovery learning (learning through doing, rather than through verbal or
physical instruction, which proved to be very effective but time consuming
for the trainer);
•
Comprehension, reflex, attitude, memory and procedure (cramp) technique
(which incorporates all the previous methods of learning, and proved very
helpful to older men); and
•
Programmed instruction (which provides immediate feedback and positive
reinforcement, and is aligned to behaviour modification).
4.98 Recommended actions to assist successful training of older workers include:
•
Trainability testing, checking out a person’s ability to learn a short task
before investing time and resources into training.
274 The approach has three
steps:
•
Teaching the worker a task, using standardised instructions and
demonstration techniques;
•
The worker performs the task unaided; and
•
Errors are recorded on a standardised checklist, performance is
graded and trainability rating established.
•
Changing the attitudes of supervisors and managers, as older workers tend
to fear failure and/or inability to compete. Recognise that in many cases,
these people and the trainers may be younger than the older trainee;
•
Base training on job or task analysis;
•
Allow adequate time for mastery of skills, by moving from simple to
complex tasks, and include demonstration of mastery of skills. Computer
training is the best example of this need;
•
Recognise that older workers generally require longer to reach proficiency
than younger workers by allowing longer periods for study and to complete
273 Sterns and Doverspike p 313
274 Sterns and Doverspike p 310
Page 57 of 144
link to page 59 link to page 59 link to page 59 link to page 59 link to page 59
tasks and tests, and have slower rates of presentation (although there is
other research which indicates no difference in learning times between
groups of workers in their twenties and in their fifties
275);
•
Ensure the training environment is comfortable for the older trainee;
•
Ensure the training builds on the existing skills, knowledge and abilities of
the trainee, and use material that is both familiar and relevant to them;
•
Ensure they are motivated to be trained and to learn; and
•
Even with self-paced training, older trainees tend to need more support and
interventions from the trainer. Care must be taken, however, to maintain
their sense of status and self esteem.
4.99 Lastly, it is timely to remember that with the current pace of technological change,
many new skills are becoming obsolete within a few years, and that regardless of
age, workers’ skills will need updating roughly every five years.
276
4.100 Despite all this, there are not many labour market adjustment programmes
specifically targeted for older workers, although it is suggested that governments
will need to pay more attention to this segment of the labour market as the working
population ages. Those programmes that have started have been successful. For
example Sweden has achieved a 90% labour market participation rate among older
individuals while keeping overall unemployment rates down to 5%. Training
programmes in the United States which were more personalised and included
ongoing counselling and assessment activities were effective in encouraging the re-
employment of older workers.
277
4.101 Finland has established two new programmes to encourage greater participation in
the labour force of older workers. The first, the “Carrot Project”, involves the
provision of help and advice to companies with at least 40% of their workforce over
the age of 45 and includes an audit of the staff’s work ability. Changing
management style is seen as a key lever in this project along with developing
participation in change management.
278 The second, the Maintenance of Work
Ability (MWA) Barometer, was established out of the need to decide the extent,
content, and functionality of the activity to maintain work ability in work places.
Three quarters of companies report undertaking MWA activities, which contribute
to business success as well as help facilitate the recruitment of labour in times of
shortage, and are used in managing the progress of senior managers.
279
4.102 The normal ageing process encompasses physical, neurological and sensory
changes, all of which the older worker adapts to. Simple ergonomic changes
which assist older workers retain their efficiency and their employment include:
•
Improving lighting;
•
Implement colour coding schemes to reduce need to use fine print;
•
Supply magnifiers where appropriate;
275 Murrell and Humphries 1978 pp 363 - 365
276 Sterns and Doverspike p 325
277 HRDC 1997 Section 7.2
278 FNPAW 2000 p 4
279 ibid p 4
Page 58 of 144
link to page 60 link to page 60 link to page 60 link to page 60 link to page 60
•
Ensure instructions are given clearly and audibly;
•
Ensure safety warnings are clear, including safety markings in any vehicular
areas; and
•
Recognise changes in older workers’ flexibility, strength, speed and reaction
times.
280
4.103 Grey Skills Home and Employment Services have been established throughout New
Zealand to provide temporary assignments for people aged over 40. The network
provides services such as home property maintenance services. The success of the
system is apparent in the fact that it is the largest home services group in NZ with
over 400 service providers (all aged over 40).
4.104 The philosophy of Grey Skills is:
Towards a world where age is no barrier to success. An organisation for people who
have had their rights infringed because of their age; to recognise and acknowledge their
intrinsic value, and help them find quality employment with quality employers.281
(b) Gender
4.105 Gender based research is focused only on the problems faced by women, largely
because of the significant numbers of lone parent families headed by women. Job
loss for this group occurs frequently because of the nature of jobs they find, the
generally low technical and personal skills they bring to jobs, and the pressures and
disruptions of their personal lives as they juggle responsibilities between their
children and their employers.
282 The pattern of rapid job loss / job acquisition is
repeated often.
4.106 There is also the issue of wanting to return to work. One quarter of unemployed
German women with children only want to return work at a later date - even if they
were offered a job immediately, they would not take it, according to the German
Department of Work and Income.
283
4.107 There are not many programmes specifically for long- term unemployed or injured
women attempting to return to work. The few programmes that exist are related to
affirmative action programmes to increase the participation of women in the labour
force generally. Ireland had long had a lower female participation rate in the
workforce than most other countries (less than 60% of women in the 25-54 age
group compared with 75% in the United Kingdom and over 80% in Sweden).
284 The FAS (the Irish Training and Employment Authority) developed specific
programmes under the banner Women in Focus, starting in 1990. This includes:
•
Incentives to employers to employ and train women apprentices;
•
Training programmes for women only on return to work skills;
•
Specific job skills, and specialist skills required by individual firms;
•
Career development;
280 Larson 2001 pp 67 - 68
281 Grey Skills website: <www.employment.co.nz/grey%20skills>
282 Hershey and Pavetti p 74
283 press statement sourced through Internet
284 press statement from Irish Hotels Federation 22 February 2000.
Page 59 of 144
link to page 61 link to page 61 link to page 61 link to page 61
•
Training for “traveller women”;
•
Community skills development;
•
Home care;
•
Care of the disabled; and
•
Updating of skills.
4.108 They also developed a new childcare worker training programme for unemployed
women to meet the growing demand.
285 According to the OECD, these
programmes have been successful: The rate of employment among females in
Ireland increased by 15 percentage points from 1994 to 2002, and the rate of
employment for young women aged 25-29 at 78% is higher than in most OECD
countries.
286
4.109 Sweden also has introduced major gender equality initiatives for all ages, ranging
from gender equality in schooling, working life, to health, and violence. Specific
work initiatives include a programme to support women starting up and running
their own businesses.
287
4.110 Australia has a Return to Work programme which assists people who have been
unemployed for more than two years, particularly women, with information
technology skills and other assistance to enable them to re-enter the labour force.
288
They also have a Small Business Enterprise Culture Programme which fosters skills
development initiatives and mentoring services for small business and supports
women in small business.
4.111 The UK New Deal for Lone Parents is a voluntary welfare to work programme
designed to increase the participation of lone parents into paid work, and to
improve their job readiness and employment opportunities. In that most of the
317,000 participants over four years were female (94%), the results give an accurate
portrayal of effectiveness of programmes for women. The programme incorporates
a Personal Adviser (PA) for each participant. PAs provided the following assistance
as required to make the transition to work:
•
Learning about the client so that they can provide support and help to find a
job that the client will enjoy;
•
A “better-off calculation” to ascertain how much better the person would be
in a job;
•
Drawing up an action plan to help the client get that job;
•
Practical and specific help in looking for and applying for suitable jobs;
•
Help in accessing training;
•
Help in accessing childcare;
•
Help with expenses during the job search;
285 FAS website: www.fas.ie
286 OECD: Babies and Bosses press release November 2003.
287 Regeringskansliet Factsheet: Some gender equality initiatives in 2002
288 Australian Budget Report 2000
Page 60 of 144
link to page 62 link to page 62 link to page 62 link to page 62
•
In-work financial planning advice on benefits available while in
employment; and
•
Continued help and advice after the client has found work.
4.112 PAs have a high degree of flexibility and autonomy to enable them to tailor services
to meet the individual needs of each client. The programme operates within a
wider suite of measures to increase employment rates among lone parents.
4.113 The programme has been widely evaluated. There is a growth in repeat
participation, and a third of all participants being on the programme for a second
time or more.
289 Any of being male, old, non-white, or having many / young
children appeared to reduce chances of leaving the programme for work, but
interestingly, those with the most disadvantages had better return to work rates
than those with fewer impediments to return to work.
290 The jobs gained were
generally of good quality and sustainability, and gave good satisfaction to
participants.
(c) Ethnicity
4.114 There are few programmes which address the issues regarding return to work of
different ethnic groups, probably because most countries have anti-discrimination
legislation which covers discrimination based on ethnicity, and this is assumed to
be sufficient. A British study cited two examples of addressing ethnic issues, one
being the provision of in-work support to Maori and Pacific peoples in New
Zealand, and the other a Finnish programme focused on the immigrant population.
In the latter programme to support the transition into employment, immigrants are
provided with two job coaches – one a native Finn and the other also an immigrant
– to support the worker and employer. Beyond the transition stage they may
receive further training such as for specific workplace language or workplace
culture.
291
4.115 The Luxembourg National Plan for Vocational Training and Integration covers all
vocational training measures for unemployed workers, with the aim of providing
them with the qualifications required by the labour market for those who do not
have specific vocational training or their qualifications are insufficient or
unsuitable. Priority is given to those with special difficulties of vocational (re-)
integration such as disabled people, women, and migrants.
292
4.116 American states are developing programmes, largely in response to the growing
Hispanic population. Courses have also been provided for Chinese, Ethiopian,
Liberian, Somali, Bosnian, Eastern European, Hmong, Vietnamese, and Sudanese
students.
4.117 Three types of programme have been identified:
•
Bilingual, where skills training is taught in the native language of the
participants;
•
Integrated, which teach both english and skills training concurrently; and
289 Evans et al 2003 p 95
290 ibid p 99
291 Kellard et al 2002 p 85
292 Thornton and Lunt 1997p 230
Page 61 of 144
link to page 63 link to page 63 link to page 63 link to page 63 link to page 63 link to page 63 link to page 63 link to page 63
•
Sequential, where individuals begin with english language classes and
progress to skills training after a certain level of proficiency in english is
reached.
293
Generally, courses require participants to be literate in their own native language.
4.118 As a result of the 1996 survey of long term unemployed, funding was provided to
purchase training in English for Speakers of Other Languages (ESOL) for up to 500
unemployed job seekers in 1996/7 and 1997/8.
294
Type of disability
4.119 Type of disability is a more important influence on return to work than severity.
People with amputations, bruises and contusions are more likely to return to work
sooner than people with sprains, dislocations and fractures.
295 Partly this reflects
the physical demands of a job, as low skilled manual workers with sprains and
fractures are less able to return to work promptly.
4.120 There is considerable research exploring which type of vocational rehabilitation
works best for different disabilities.
(a) Mental health problems
4.121 There is no doubt that people with severe and enduring mental health problems
benefit from work.
296 It can be a significant factor in keeping people out of hospital
and reducing their use of medication and out-patient services. Getting people into
work quickly after periods of hospitalisation is critical to successful treatment.
297
Research results on successful rehabilitation include:
•
An individual placement and support (IPS) programme for people with
severe mental disorders in an inner-city context s were shown to be more
effective than an enhanced vocational rehabilitation (EVR) programme.
This was due to the rapid job search methods of the IPS programme
compared with the stepwise approach of the EVR;
298
•
Supported employment is more effective than pre-vocational training;
299
•
People with mental health problems are more likely to obtain and retain
work if they are placed in work which accords with their stated
preferences;
300 and
•
The chances of gaining employment are likely to be linked not only to
appropriate vocational rehabilitation services and the local labour market,
but also to work disincentives in the disability pension system. A crucial
factor was the “earnings disregard”: the amount of earned income a disabled
293 Wrigley et al 2003 p 43
294 Parker 1997 p 72
295 Johnson and Ondrich 1990 p 584
296 Schneider 1998 pp 812 - 894
297 Riddell 2002 p 45
298 Drake et al 1999 pp 627-633
299 Crowther et al 2001 p 207
300 Mueser et al 2001 pp 411-417
Page 62 of 144
link to page 64 link to page 64 link to page 64 link to page 64 link to page 64
worker may receive before his or her governmental benefits are reduced or
discontinued.
301
4.122 There are various publications and web-sites dedicated to assisting people with
psychiatric illnesses manage their relationship with work and employers, but few
courses. Boston University’s Center for Psychiatric Rehabilitation offers many
services, including what it describes as “ the only site designed exclusively to
provide information…for people with psychiatric disabilities”.
302
4.123 Research indicates that while there are some generalisations which can be made
about which tasks or skills are likely or unlikely to be performed by people with
type of mental illness, each case must be assessed individually.
•
Problems with memory are associated with people with schizophrenia,
depression and anxiety;
•
Inability to maintain speed at performing assembly level tasks is associated
with depressions and obsessive compulsive disorder;
•
Difficulty staying with a project until completion is associated with those in
the manic phase of bipolar disorder, attention hyperactivity disorder,
schizophrenia, and histrionic personality disorder;
•
Lack of reliability / punctuality is associated with agorophobia, somatization
disorder, avoidant personality disorder, antisocial personality disorder,
major depression, and borderline personality disorder;
•
Taking pride in doing a good job, and staying with the task can be
problematic for people with antisocial personality disorder, schizoid and
passive-aggressive personality disorder, and major depression; and
•
Difficulty maintaining interpersonal relationships at work may reflect
bipolar disorder, post traumatic stress disorder, antisocial personality
disorder, passive-aggressive personality disorder, schizoid personality
disorder, borderline personality disorder and narcissistic personality
disorder.
303
4.124 It is important to remember the cyclical nature of several mental illnesses, and that
the number and dose of prescribed medications and their side effects must also be
considered when planning employment. Providing on-job support systems is a
critical part of maintaining the employment of people with mental health problems,
such as being alert to signs of medical non-compliance, and managing employment
issues like supervisor and co-worker support, job appropriate job-matching,
flexible working schedules where necessary and providing feedback
constructively.
304 Supported employment is more effective than pre-vocational
training at helping people with severe mental illness to obtain competitive
employment.
305
301 Warner 2001 pp405-9
302 website ,www.bu.edu/SARPSYCH/jobschool/main.html>
303 Marini 2003 p 40
304 ibid p 41
305 Crowther et al 2001 p 207
Page 63 of 144
link to page 65 link to page 65 link to page 65 link to page 65 link to page 65 link to page 65 link to page 65
(b) People with traumatic brain injury (TBI)
4.125 Neurological outcomes of head injury include memory impairment, personality
disturbance, decreased motor control, fatigue, speech and language difficulty,
attention and concentration deficit, and lack of initiative.
306 While researchers
disagree on what are the most effective programmes to assist these people return to
work, it is useful to summarise those which variously have been found to be
effective:
•
Developing awareness and acceptance of any deficits resulting from the
brain injury – people unable to do this will not be able to become productive
in the community
307. Return to work is influenced less by the severity of
the injury than by the relationship to functional independence;
308
•
Supported employment. This should include learning how to lessen
memory problems, (by learning new ways to achieve tasks or learning
strategies to recall information more accurately) and error correction
processes. Care must be taken lest the worker becomes overly reliant on
their support;
•
Individualised return to work programmes, including components like
assessment and vocational evaluation, simulated work, work hardening and
training develop stamina, transitional employment, vocational counselling,
job-seeking/ keeping skills training, job development, job analysis, job
placement, one the job training and support; and
•
Group cognitive skills training, with the development of thinking skills
related to problem solving, concentration / attention, decision making,
remembering names and faces, study skills, functional mnemonics, goal
setting, non-verbal perception, test taking strategies. In this project,
members of the group successfully tutored each other.
309
4.126 Research has identified that individuals with TBI rated most difficult to assist
tended to be younger, have functional limitations such as visual and fine motor
impairments, and lacked numerous work-related skills.
310 Job coaching has been
proven to be successful for those with cognitive or behavioural problems.
311 Understanding and then managing unacceptable behaviour is key to retaining
employment, whether the person recognises that the behaviour is inappropriate, or
they have chosen to behave that way.
312
4.127 Lastly, the professional support person for the worker with TBI needs to fade their
presence and assistance gradually, basing this on the performance data they have
been collecting as they assist the worker. It is important to retain a long term
relationship of “touching base” with the worker’s supervisor to assess whether any
further assistance is required.
306 Riddell p 48
307 Yasuda et al 2001 p 856
308 Greenspan et al 1996 p 207
309 Parente and Stapleton 1999 pp13 - 20
310 Yasuda et al 2001 p 857
311 Brantner 1992 p 3
312 Yasuda et al 2001 p 681
Page 64 of 144
link to page 66 link to page 66 link to page 66 link to page 66
(c) People with hearing problems
4.128 Many deaf people lack generic employment skills, and have ongoing problems with
communications. It is sometimes assumed that employing an interpreter will be
sufficient measure to negotiate workplace adjustments with an employer and to
establish communications with co-workers.
313
4.129 The best way of ensuring people with hearing problems retain their employment is
to have a job coach during the initial period of employment. This is not always
easy to do as such job coaches require the following skills:
•
Expertise in deafness and manual communication methods;
•
Knowledge of other disabling conditions;
•
Observation, assessment and reporting skills ;
•
Teaching skills;
•
Knowledge of appropriate legislation; and
•
Knowledge of rehabilitation technology and job modification options.
4.130 Use of sign language helps many people with hearing problems. Belgium has
recently decreed that sign language is their fourth national language, but their
challenge is now to implement the change in the fields of education and training,
employment, culture, information and health. American Sign Language is the
fourth most commonly used language in the United States and earlier in 2003
Britain recognised British sign language as a language in its own right.
4.131 Research has identified that more attention post employment placement would be
beneficial, to assist workers establish and maintain communications with co-
workers. This is best achieved using a job coach rather than an interpreter.
314
(d) People with sight problems
4.132 Italy reserves employment in both public and private organisations specifically for
blind people who are registered on a professional roll managed by the Labour
Ministry. Blind people in Italy work mainly in telephone switchboard operation,
masseur physiotherapy and teaching. Technology refresher courses and sighted
assistance are provided as appropriate. These provisions have proved so successful
that it is unnecessary to look sheltered employment to meet the occupational needs
of blind people.
315 In the US, assistance is given to train and license blind people to
operate vending facilities on federal and other property.
316
4.133 Light engineering, shorthand and typing, and switchboard operation, the
traditional areas of employment for blind and partially sighted people, are declining
at a marked rate, being replaced by call centres, customer service, and computer
programming. This latter has been assisted by the development of synthetic speech
and voice recognition technology. Expansion of employment opportunities for the
blind depends partly on finding quick solutions to access new technologies, and
313 Riddell p 49
314 ibid
315 Thornton and Lunt 1997 p 174
316 ibid p 281
Page 65 of 144
link to page 67 link to page 67 link to page 67 link to page 67 link to page 67
partly on addressing the continuing prejudice of employers about hiring people
who have difficulty seeing.
317
4.134 Again, post employment placement support is essential, best performed by a job
coach.
318
(e) People with back problems
4.135 A comprehensive 6 nation longitudinal study on people with back problems found
that early interventions /return to work were more beneficial than later
interventions.
319 All people studied had been out of work for at least three months
due to their back problems, and if they had not returned to work by the end of 12
months out of work, they were unlikely to return at all.
4.136 This research was supported by a Swedish study which found that the treatment
programme was more effective for workers who had been on sick-leave for back
problems for only a short time than for those who had been off-work for a long
time.
320 Those on short-term sick leave increased their ability to control and
decrease pain, reduced their disability and impairment, and increased their general
activity level, compared with a control group.
4.137 Australian research indicates that back injury patients are in general likely to
benefit because of, rather than in spite of, returning to work.
321
4.138 Key actions for rehabilitation are:
Step 1
•
Accurate assessment of injury, including symptoms, signs, patient’s capacity
and the patient’s psychological state;
•
Early communication with the key parties – patient (about their condition,
recovery time, and early return to work), employer (about strategies for
return to work), treating professionals (about treatments), family / union
representatives where appropriate (may need to recognise cultural and
language difficulties) , specialists for second opinions where required, and
rehabilitation counsellors; and
•
Reducing pain.
Step 2
•
Determination of reduced hours / lighter duties; and
•
Addressing psychosocial factors, and increasing patients’ own resources to
deal with pain situations.
Step 3
317 Jackman 2001 p 2-3
318 Riddell 2002 p 50
319 Bloch and Prins 2001
320 Marhold et al (2001) p 162
321 Gun and Fraser 1992 p 4
Page 66 of 144
link to page 68 link to page 68 link to page 68 link to page 68 link to page 68 link to page 68 link to page 68
•
Training in the functional capacities needed in work and life situations.
This includes handling difficulties at return-to-work such as fatigue and
anxiety.
4.139 A Dutch study on return-to-work interventions for people with low back pain
concluded that physical exercises were a key component, and that the most
effective was graded physical activity based on a behavioural concept.
322
4.140 The psychosocial factors vary, but include job satisfaction, and low social support
in the workplace. The patient’s own belief about their work return is important.
323 Good relationships with colleagues are a strong motivating factor for return to
work but bad relationships with supervisors were a demotivating factor.
324 These
need to be addressed as part of the vocational rehabilitation plan. As stated
elsewhere in this report, if the injured worker was not happy in their previous job,
it is probably better that they consider and/or implement a career change, or at least
a change of employer.
4.141 One of the difficulties in dealing with clients with back problems is that the severity
of pain is very subjective. Constant medical assessment consolidates the syndrome
of the disabled back. Diagnosis can be imprecise and inaccurate, despite the
assistance that sophisticated methods of diagnosis can provide. The conclusion is
that it is better to orient attention towards rehabilitation rather than on dubious
diagnostic aids such as X-rays.
325
(f) People with serious injuries
4.142 While severity of disability has a bearing on labour force participation, this is not
due to the severity of the injury but to attitudes of employers. High rates of
discrimination are reported by people with moderate to severe levels of disability.
326 There are many examples in literature illustrating the potential of individuals with
sever disabilities to work, given appropriate supports.
327 The fact that such
employment is possible, however, does not mean that it is easily obtained.
(g) People with spinal injuries
4.143 Recent research on employment outcomes for people with spinal injuries reported
that more individuals started with a new employer rather than returning to their
pre-injury employer. Those who returned to their pre-injury employer returned to
work much earlier than those who found new employment.
328 There was a
significant relationship between gender and type of work: men were twice as likely
to be in paid employment, whereas women were in non-paid roles such as
voluntary work, education, and home-makers. Age was also relevant: people
injured before the age of 18 had an employment rate of 69% whereas those injured
after 45 had an employment rate of only 9%.
322 Staal et al 2002 p 264
323 Marhold et al (2002)
324 Gard and Sandberg 1998 p 106
325 Landon Smith 1977 pp 1076-7
326 Bunch and Crawford 1998 p 33
327 Perrin p 17
328 Yasuda et al 2002 summary
Page 67 of 144
link to page 69 link to page 69 link to page 69 link to page 69
4.144 Those who were employed reported receiving fewer medical treatments, completed
more years of education, were more satisfied with their lives and rated their overall
adjustment higher than individuals who were not employed.
4.145 The important conclusions from the research are the ability of people with spinal
injuries to regain employment, and the benefits of being employed.
(h) Other injuries / disabilities
4.146 Spain provides special assistance for people suffering from toxic syndrome, whether
they lost their job as a result of getting toxic syndrome, or who are unemployed
and suffering from the syndrome, or have been undergoing treatment for more than
a year.
329
Problems arising from pre-injury circumstances
(a) Family circumstances
4.147 Belgium provides a childcare allowance for unemployed women undergoing
vocation training, recognising the importance of this to encourage long term
unemployed women to re-enter the labour market.
330 In Hawkes Bay in New
Zealand, Work and Income found that providing a free childcare service helped
reduce numbers of unemployed at the same time as satisfying the labour demands
of seasonal industries.
331
4.148 A British study on job retention programmes in OECD countries found that the
provision of childcare provided benefits in terms of job retention and improved
work performance. Childcare needed to be flexible and meet both employees’ and
employers’ requirements. In the United States, subsidised childcare is available for
up to 24 months to welfare recipients moving into employment, and some states
are encouraging both providers of childcare and employers to extend childcare
services into non-standard hours and for emergency situations. Assistance is also
provided in some states to transport the children to childcare providers.
332
(b) Job satisfaction
4.149 While there are no formal programmes to remove the barrier of low job satisfaction
in their previous jobs, often the programmes which address other issues such as
poor work skills and attitudes will help the unemployed /injured workers achieve
better job satisfaction in their new jobs. Such initiatives are outlined elsewhere in
this paper. If it transpires that the unemployed /injured worker was not happy in
their previous job, it is appropriate for them to take the opportunity to consider
and/or implement a career change.
(c) Job history
4.150 While there are no programmes to address job history retrospectively, some
countries do address the issue of maintaining a work history while unemployed.
329 Thornton and Lunt 1997 p 235
330 Geers 1992 p 62
331 East Coast Regional News June 2002
332 Kellard et al 2002 pp 33-4
Page 68 of 144
link to page 70 link to page 70
Denmark has formal requirements for people of employable age without work who
receive some income support to be
active.333 The primary purpose of this is to bring
people back into employment by developing their human capital: i.e. enhancing
their qualifications and employability. It is the responsibility of the individual to
improve his or her qualifications, working ability and ability to be self-sufficient. In
principal, activation is a non-permanent situation, although there are some in the
more disadvantaged groups who have been moving between schemes for some
time.
4.151 Activity, which must be formally organised, may include:
•
Work activity which leads to some product or service, with a wage subsidy
in public or private enterprises, in voluntary organisations, or in special
institutions set up for social assistance recipients;
•
Training or education activity, such as introductory courses, job training,
and counselling;
•
Activities of a social nature, including exchange of experience with other
people in similar situation; and
•
A mix of the above.
Individual activity, such as childcare or gardening, is not accepted as an active
measure.
4.152 The evaluation of the UK New Deal for Lone Parents noted that there are some
people who “cycle” between work and benefits.
334 This may be due to job-related
problems, individual characteristics, family circumstances, or a combination of
these. There are other people who change jobs constantly, often for a combination
of the above factors, or the desire for time out of the workforce, seasonal factors
etc. Researchers caution that these cyclically employed people have quite different
needs and require to be treated differently from other job-seekers. Case managers
need to determine the underlying cause of the cycle, such as a need for training or
education, for family support, or managing conflict.
(d) Relocation
4.153 For many professional people who become unemployed, relocation to a centre
where relevant jobs are available is often ruled out. The usual reasons given are:
•
Being part of a two-career family which means that the other party has to
arrange a job transfer or find a new job;
•
Financial concerns about selling and buying houses;
•
Disruption to social relations including schooling, families, and recreational
activities.
4.154 None of these are insurmountable. Ways of addressing these include:
•
Asking the prospective employer for assistance in finding the partner a job –
in America, many firms have programmes to assist spouses find jobs, not
necessarily with the same company;
333 Rosdahl and Weise p 161
334 Evans et al 2003 p 107
Page 69 of 144
link to page 71 link to page 71
•
Using the Internet to collect information on possible employers and job
opportunities;
•
The partner seeking a job transfer with their existing company, including
continuing in the same job but based at a different location, and teleworking
from home;
•
Paying some or all of the costs of relocation, whether by the new employer
or the agency assisting the worker to find employment, including providing
bridging finance to cover mortgages;
•
Careful consideration of the value of community roots and involvement,
hobbies, schooling etc. Refusal of relocation should come after careful
consideration of the issues and how these may be resolved rather than
through inertia.
335
(e) Criminal records
4.155 Helping people with criminal records is relatively straightforward, and many
programmes have been proven successful.
336 In addition, employment may be a key
strategy in reducing repeat offences. It is important that return to work programme
providers are aware of participants’ criminal histories, which are then handled in a
practical and non-judgemental way. This includes:
•
Teaching participants how to address heir records in resumes and
applications;
•
Ensuring participants are ready to answer questions about their past;
•
Helping individuals address any current legal issues they may have, such as
parole, creditors, child support etc;
•
Focusing on presentation, communication and confidence in job search;
•
Recognising that extra time is likely to be needed to find a job;
•
Being alert to substance abuse;
•
Preparing participants to handle questions or reactions from co-workers;
•
Knowing what occupations are “friendly” to ex-offenders; and
•
Being honest and straightforward with employers, and encourage them to
provide a work trial at the least.
(f) Obesity
4.156 In April of 2002 the United States recognised obesity as a disease. This was a
contentious decision as some people believed that obesity was purely a matter of
personal choice, of a sign of mental aberration.
4.157 Taxpayers have been able to deduct the costs of weight loss programs as a medical
expense since 2000 if they were recommended by a doctor to treat a specific
disease. Obesity itself was not recognised by the Inland Revenue Service (IRS) as an
ailment that qualified for the weight loss expense deduction.
335 Borchardt 2002 p 9
336 Brown 2001 p 83
Page 70 of 144
link to page 72 link to page 72 link to page 72 link to page 72
4.158 To receive the deduction, a taxpayer must participate in a weight-loss program for
medically valid reasons. Simply joining a gym or a weight control program to
``improve the taxpayer's appearance, general health and sense of well-being' and
not under a physician's guidance will not qualify, the IRS said.
4.159 Also not deductible are diet foods, even if they are an integral part of the weight
loss plan. The IRS reasons that people have to pay for their food whether or not
they are trying to lose weight. The deduction comes in the area of medical
expenses, which must in total exceed 7.5 percent of adjusted gross income and can
only be taken by taxpayers who itemize their deductions.
B External factors
Attitudes of employers
4.160 Australian research into employer attitudes to the unemployed found that while
some employers speak quite negatively about people, others feel empathy and
sympathy for the unemployed and for their situation. Attitudes towards long term
unemployed, however, were generally negative and pessimistic. Rightly or
wrongly, there was a perceived stigma around the long term unemployed and this
influenced their bias against employing them.
337 There was almost universal
support towards employing women who were returning to work after raising
children, while there was an acknowledged stigma attached to older men.
4.161 In general, the most important thing for employers is to find the right person for
the job – the right skills, experience and attitude.
338 American research indicates
that in response to an uncertain economy when employers become more cost-
conscious and risk-averse, hiring decisions are more likely to be driven by a desire
to avoid making a mistake rather than to recruit the most promising candidate.
339
4.162 It is important to recognise that some employers will not want to re-employ some
individuals post an injury for a variety of reasons such as poor performance,
attitudes or relationships.
(a) The Disability symbol
4.163 The British Employment Service holds a register of employers who have
demonstrated a commitment to employing people with disabilities, using the
disability symbol as the representation. These employers generally have policies
specifically addressing the employment of people with disabilities, covering issues
such as recruitment, retention, training and development, promoting awareness
and adaptations. They were six times more likely than other employers to be
actively seeking to recruit disabled people. In a 1994 survey, 85% of them said
they would have paid for any necessary adaptations or modifications for existing or
new disabled staff.
340
4.164 The disability symbol, which is a Government initiative, has been developed so
employers can show their commitment to good practice in employing disabled
337 Dept of Employment and Work-place Relations 2001 p 4
338 Snape 1997 Executive summary
339 Bricout 2003 p 45
340 Dench, Meager and Morris 1994 Executive Summary
Page 71 of 144
link to page 73 link to page 73

people. It is a communication tool which can be used by employers to encourage
disabled people to apply for specific jobs. Employers who use the symbol make five
commitments to action. These are :
•
A guaranteed job interview: To interview all applicants with a disability who
meet the minimum criteria for a job vacancy and to consider them on their
abilities;
•
Consulting disabled employees regularly: To ask disabled employees at least
once a year what you can do to make sure they can develop and use their
abilities at work;
•
Keeping employees if they become disabled: To make every effort when
employees become disabled to make sure they stay in employment;
•
Improving knowledge: To take action to ensure that key employees develop
the awareness of disability needed to make your commitments; and
•
Checking progress and planning ahead: Each year, to review these
commitments and what has been achieved, plan ways to improve on them
and let all your employees know about progress and future plans.
4.165 Symbol users are expected to put the symbol on all job advertisements in the press
or at the Jobcentre, as well as internal vacancy advertisements and job application
forms. The symbol can also be put on letterheads, stationery, internal magazines
and newsletters; doorways and signs, reception areas, interview rooms and at career
exhibitions. An internet search on the words
disability symbol resulted in
hundreds of advertisements on their accredited status from proud employers.
4.166 Several countries also provide systems to recognise “good employers” of people
with disabilities such as the Greek Letter of Approval, public acclaim and small
prizes,
341
(b) Duration of unemployment
4.167 One way of handling the negative perceptions of employers regarding long term
unemployed is to involve the employers more in public employment and training
programmes. Research shows a strong positive link between participation in such
programmes and the experience of recruiting unemployed people.
342 Following a
positive experience of employing a previously unemployed person (whether
directly or through a programme) lead to a readiness to take on more unemployed
people. But a negative experience, especially if accessed through a public
programme, had the opposite effect. The key message to programme managers was
to manage carefully the selection and placement of unemployed people.
341 Thornton and Lunt 1997 p 147
342 Atkinson, Giles and Meager1996 Executive Summary
Page 72 of 144
link to page 74 link to page 74 link to page 74 link to page 74 link to page 74 link to page 74
4.168 The Denver Workforce Initiative provides a work-based training programme for
employers to address performance and retention problems. The
Managing to work
it out programme for supervisors (a companion programme to the
Workin’ it out
programme for entry level workers) challenges beliefs and biases about work and
workers, and presents strategies for resolving conflict, communicating with and
motivating entry level workers.
343
(c) Educating employers regarding disabilities
4.169 An American demonstration project to find employment for people with significant
disabilities who had been unable to gain employment on their own found that
employers did not view people with disabilities as qualified applicants for existing
positions.
344 As a result of an employer focus group discussion, the project team
recommend:
•
Present job restructuring as a way for businesses to save money rather than
creating jobs for disabled people. Money can be saved by eliminating the
need for overtime, or completing tasks not typically accomplished, whereas
job creation is seen as increasing costs rather than company efficiency; and
•
Employment specialists must build relationships with employers – which
does take time – so that they can demonstrate how a person with significant
physical disability can perform the essential functions of a particular job.
4.170 Australian research on employer attitudes and behaviour regarding hiring
unemployed people concluded that employers are not a homogeneous group. Each
employer has different needs, motivations, attitudes, prejudices, backgrounds and
personal life experiences.
345 A second study aims to segment employers into
groups with like attitudes and motivations, so that the Department of Employment
and Work Relations can target its approach according to what works best for each
group type.
4.171 The people with disabilities themselves may have to help employers understand
their abilities. For example, an employer may be reticent in a job interview about
asking questions on the applicant’s ability to perform certain functions. One
solution is that the applicants themselves bring up the topics of concern, and
describe how they will overcome any functional limitations. Harder to resolve is
when a manager’s empathy and pain for a person with a disability works against the
interests of the person with the disability. In these cases, the manager has to
acknowledge that the pain is their pain, not the other person’s.
346
(d) Understanding return to work programmes
4.172 “You don’t get injured workers well to put them back to work: you put them back
to work to get them well”.
347 This is the philosophy of an American rehabilitation
expert, Richard Pimentel.
348 Pimentel believes that the fundamental problem for
343 Relave 2000
344 Inge et al, p184
345 Department of Employment and Work Relations 2001 p 2
346 Pimentel 1998
347 Pimentel on www.wcbsask.com
348 Richard Pimentel, a senior partner with Milt Wright and Associates is a nationally renowned expert on job retention, attitude change
in the workplace, return to work, workers' compensation and cost containment. A Vietnam veteran with a disability, Pimentel has
Page 73 of 144
link to page 75 link to page 75
return to work (RTW) programmes are the employers and workplace supervisors.
If these people are better educated, then the problems are addressed.
4.173 Pimentel promotes work as therapy. At the appropriate point in the recovery
process, providing an injured employee with work that is compatible with any
physical restrictions and consists of activities which promote healing will facilitate
a more rapid and complete recovery than would staying at home. It also decreases
the risk of a permanent disability or re-injury when they eventually return to full
duty.
349 Pimentel notes the need to teach doctors how to work with employers in
return to work activities and how to develop work as therapy guidelines for their
patients.
4.174 Issues identified by Pimentel for employers to understand include:
•
The decision to bring an injured worker back to work should not be a
supervisor’s decision (they will select the workers whom they like / are good
workers. These people will return to work anyway);
•
Decisions about returning injured workers to the job should be in the hands
of managers who are not emotionally attached to the situation;
•
RTW programmes require processes to guide them – how to determine what
tasks an injured worker can do from the details in the medical certificate
(which normally only outlines what a worker can NOT do); and
•
Employers must understand that employees want productive work which
contribute to the company’s success while not putting them at risk of further
injury, not some mindless make-work activities.
350
Job adaptations
(a) Supported employment
4.175 Supported employment is a long established concept utilised in many countries. In
general, it aims to provide meaningful jobs for people with severe disabilities,
including traumatic brain injury. It is a way to move people from dependence on a
service delivery system to independence via competitive employment. Recent
studies indicate that the provision of on-going support services for people with
severe disabilities significantly increases their rates for employment retention.
4.176 Supported employment encourages people to work within their communities and
encourages work, social interaction, and integration. Supported employment
services should achieve the following outcomes:
•
Opportunity to earn equitable wages and other employment-related benefits,
•
Development of new skills,
•
Increased community participation,
pioneered proactive risk management, return-to-work and Equal Employment Opportunity (EEO) programs to generate cost savings
and enduring attitudinal changes in corporate culture.
349 Pimentel 1999
350 Pimentel 1998
Page 74 of 144
•
Enhanced self-esteem,
•
Increased consumer empowerment, and
•
Quality of life.
The types of supported employment services used depend on the needs of
individual consumers.
4.177 In America a job coach is a person who is hired by the placement agency to provide
specialized on-site training to assist the employee with a disability in learning and
performing the job and adjusting to the work environment. As the worker learns
the tasks, the coach’s involvement gradually fades, but they are available for follow-
up as required. Job coaching can also be used when tasks change and the
individual needs assistance in getting acclimatised to new tasks.
4.178 Natural supports are support from supervisors and co-workers, such as mentoring,
friendships, socializing at breaks and/or after work, providing feedback on job
performance, or learning a new skill together at the invitation of a supervisor or co-
workers. These natural supports are particularly effective because they enhance the
social integration between the employee with a disability and his/her co-workers
and supervisor. In addition, natural supports may be more permanent, consistently
and readily available, thereby facilitating long-term job-retention.
4.179 The different supported employment models are listed below.
4.180
Individual Placement Model--A person with a disability is placed in a job in a
community business which best suits his/her abilities and preferences. Training is
provided on the job site in job skills and work related behaviours, including social
skills, by a job coach. As the employee gains skills and confidence, the job coach
gradually spends less time at the work-site. Support is never completely removed.
The private or public vocational rehabilitation agency furnishing the job coach is
always available to the employer for retraining for new assignments, assisting in
dealing with challenging behaviours, supplying periodic consultations with co-
workers and employer, giving orientation and training for co-workers.
4.181
Enclave Model--A small group of people with disabilities (generally 5-8) is trained
and supervised among employees who are not disabled at the host company's work
site. Persons in the enclave work as a team at a single work site in a community
business or industry. Initial training, supervision, and support are provided by a
specially trained on-site supervisor, who may work for the host company or the
placement agency. Another variation of the enclave approach is called the
"dispersed enclave." This model is used in service industries (e.g., universities,
restaurants, and hotels). Each person works on a separate job, and the group is
dispersed throughout the company.
4.182
Mobile Work Crew--A small crew of persons with disabilities (up to 6) works as a
distinct unit and operates as a self-contained business that generates employment
for their crew members by selling a service. The crew works at several locations
within the community, under the supervision of a job coach. The type of work
usually includes caretaker / groundsman work. People with disabilities work with
people who do not have disabilities in a variety of settings, such as offices and
apartment buildings.
Page 75 of 144
link to page 77 link to page 77
4.183
Small Business Model--Within a small business, there may be up to six employees
with disabilities, but not more than the number of employees without disabilities.
The small business operates like any business, generating work and paying
employees from revenues received. The small business is located within the
community.
4.184 In New Zealand, Mainstream is a two-year, subsidised employment programme for
people with significant disabilities. The programme is provided by the State
Services Commission and aims to assist participants into meaningful, long-term
employment within selected State sector organisations. Placements are made by
specialist employment consultants such as Workbridge.
4.185 Almost without exception, cost-efficiency research has found that supported
employment is a better financial option for individuals with disabilities than
sheltered workshops. American research indicates that supported employment,
even for severely disabled people, becomes cost-efficient to taxpayers about the
fourth year of operation.
351
(b) Assistive technology
4.186 For people with disabilities, assistive technology is an essential tool for
independence. It is any item, piece of equipment, or product that can increase,
maintain, or improve the performance of people with disabilities. It ranges from
simple “low-tech” equipment such as a hand held magnifier, to home or vehicle
modifications, to modified software and hardware products, to ramps, wall crutches
and widened doorways. With the new advances in technology, there are fewer and
fewer instances where job modifications cannot be made to accommodate even the
most severe injuries.
4.187 While computers and technology are valuable accommodations for people with
severe disabilities, focusing solely on the technology and the individual was not
sufficient to ensure success. The needs of the employer must be balanced with the
employee’s preferences to ensure successful integration of technology and
individual.
352 Most technologies have a limited life span and it is important to
prepare for when the technology becomes unreliable or out-dated.
4.188 The work environment is another important consideration. Voice recognition
technology requires a relatively quiet environment to function accurately, and by
contrast, it can distract colleagues in open plan work spaces. Braille printers can be
noisy and may require sound-hoods.
4.189 Installation of assistive technology requires a consultative approach with the
affected worker, employers, colleagues, and may require investigation of several
options. Employers also need to be prepared to have an adjustment / settling in
period
(c) Modification of job duties
4.190 Where there is a discrepancy between the physical demands of a job and the
worker’s capacity to do that job, the next step is to assess whether some form of
351 Kregel et al 2000 p 154
352 de Jonge, Rodger and Fitzgibbon 2000 p 78
Page 76 of 144
link to page 78 link to page 78 link to page 78 link to page 78 link to page 78 link to page 78
modification to the job tasks is possible. It may be that some unessential functions
can be eliminated, or essential tasks rearranged or reallocated to accommodate the
injured worker. Sometimes this is as simple as providing special equipment such as
seating at a different height, shelving to eliminate bending and lifting.
353 Care must
be taken when reallocating duties to ensure that this is the most appropriate
approach.
4.191 There is an increasingly strong backlash from front line supervisors, unions and the
injured workers themselves as some employers in America go to extremes in
devising meaningless tasks in the name of modified duties.
354
4.192 There are several issues for employers in modifying duties:
•
Light duties must be meaningful and contribute value to the organisation;
•
Light duties for an injured worker does not mean adding additional tasks to
non-injured workers, making them work twice as hard to cover the
workload;
•
Smaller employers are less likely to have modified duties available;
•
Larger employers may have problems with cross-department/divisional
boundaries. These could be budgetary, “silo” mentality, or accountability
problems; and
•
The need to have trade union representatives on-side.
4.193 Some smaller American employers have assigned restricted duties staff to voluntary
/ non-profit organisations to keep them active during their recovery and to
maintain good working habits. While the employee works as a volunteer for such
agencies as the Salvation Army, the Red Cross or the YMCA, they are paid their
normal wages by their employer. These assignments are regarded as regular work.
The employers have found this sends a good message to their work forces that there
is no such thing as “no light duty available”. The injured worker benefits by
speeding their recovery, the company image is enhanced with positive public
relations and the local community benefits through the donation of labour to the
voluntary agency.
355
4.194 The consistent finding from multiple surveys of employers has been that expensive
accommodations are rarely needed by workers with disabilities.
356 In one project
in 2000, 100 accommodations were made at a total cost of US$11,235, making the
average cost per accommodation $112.35.
357
(d) Teleworking
4.195 In the United States, alternative work arrangements have proliferated as employers
seek to meet staffing and production needs through non-traditional employment
arrangements.
358 These include different work location (eg at home), work contract
(such as on-call, temporary or leased) and employment status. Of particular
353 New York Workers’ Compensation Board p 33
354 Kremer 2003 p 40
355 ibid p 45
356 Unger and Kreel 2003 p 5
357 Inge et al 2000 p 183
358 Anderson et al 2001 p 97
Page 77 of 144
link to page 79 link to page 79 link to page 79 link to page 79 link to page 79
interest to people with disabilities is teleworking, sometimes known as
telecommuting. It is work performed at a distance from the main work-site,
usually using information and communications technology, such as computers,
telephone, videophones and faxes.
4.196 Because of the flexibility of telework, it reportedly:
•
Saves office space;
•
Boosts productivity;
•
Reduces absenteeism and sick time;
•
Reduces commuting time;
•
Improves staff morale and thus
•
Improves staff retention rates.
359
4.197 A British company developed a successful programme for women returning to work
who wished to become teleworkers.
360 The training was subsequently extended to
women in prison and families with at-risk children. Key to the project was the use
of the most up to date information technology, both hardware and software. The
courses - run for two days a week for ten weeks - include personal development to
encourage the participants to recognise their worth, increase their confidence, and
to accept responsibility for making changes in their own lives. The training
stresses that teleworking and child minding cannot be carried out simultaneously.
Barriers faced by the company included a lack of awareness of teleworking, and a
lack of funding.
4.198 For people with disabilities, telework offers an accessible, barrier-free workplace,
flexible work scheduling, and the elimination of any bias or discrimination.
Typical jobs include word processing, telephone customer service, programming,
accounting, data entry, editing, filling orders, researching, and writing. A
Minneapolis study indicated that most companies require staff to attend the office
at least for training, retraining and team meetings, and also to provide back-up
services as required.
361 Teleworking requires clearer communications, explicit
expression of tasks and standards of performance, which provide incidental
benefits to the company such as better delegation and staff empowerment.
4.199 Acknowledged downsides for people with disabilities include:
•
The consequent lack of social contact, given that many people with
disabilities are already relatively socially isolated; and
•
Possible lack of career and promotional prospects;
362 and
•
A lesser profile of people with disabilities as co-workers and productive
members of the labour force.
363
359 Anderson et al 2001 p 98
360 Murray 2001 pp1-8
361 ibid p 99
362 ibid p 101-2
363 Bricout 2003 p 48
Page 78 of 144
link to page 80 link to page 80 link to page 80
(e) Work trials
4.200 Work trials have long been used to help a potential worker try out a specific
occupation, and for potential employers to assess a person’s suitability for that job.
Usually, the worker’s wages are paid by the agency placing them in the trial,
although the length of trials can vary from between four and twelve weeks.
Workers benefit because they can experience a job and a company on a first hand
basis, while employers benefit because they can become familiar with an employee.
Although the employer is not required to hire the individual, in many cases, they
do make an offer of employment at the end of the trial.
4.201 To achieve any benefits, to worker or employer, a work performed under a work
trial must be meaningful, constructive, productive, and add value to the company.
In this respect, it is no different from temporary light duties.
Case management / rehabilitation issues
4.202 The case manager plays a vital role in the rehabilitation of a long term unemployed
or injured worker. All too often case managers report lack of time to invest in their
clients. In Michigan, welfare-to-work program managers sought greater flexibility
to provide a wider range of screening, assessment and referral services, and to have
more time to work with the most disadvantaged people.
364 The problem is assessed
as not so much being the client, but the services available do not meet the clients’
needs.
4.203 Case management as a concept can include :
•
Monitoring progress of a client’s return to work,
•
Referral to specialist services such as childcare, transportation, housing or
treatment,
•
Advice, counselling and problem-solving, and
•
Calculating appropriate financial assistance for the client.
4.204 A British study found that case management worked best if case workers were able
to build a long-term trusting relationship with a client, and that caseloads must be
kept low if case managers are to provide the individually intensive assistance that
most clients require.
365 This included case managers doing what they say they will
do, listening to client concerns, and being available at relatively short notice, and
occasionally outside conventional working hours.
4.205 The commonly held view of case management in education, medicine, psychology
and many other disciplines has been a deficit, disorder, problem-oriented paradigm.
The emphasis has been on risk factors that define what is wrong, missing or
abnormal. Viewing the world through this deficit lens prohibits seeing strengths,
resources and capabilities.
366
4.206 Social workers are increasingly focusing on how to discover and build on clients’
strengths. Known as the “strengths perspective”, it relies on five key assumptions:
364 Danziger and Seefeldt 2002 p 80
365 Kellard et al p 3
366 Utesch 2001 p 1
Page 79 of 144
link to page 81 link to page 81 link to page 81
•
Despite life’s problems, all people and environments have strengths that can
be marshalled to improve the client’s quality of life;
•
Client motivation is fostered by a consistent emphasis on strengths as the
client defines these;
•
Discovering strengths is a co-operative exploration between case manager
and client, not driven by an “expert”;
•
The focus on strengths leads to discover how the client has managed to
survive even the most hostile of environments (rather than blame the victim
for their circumstances); and
•
All environments, even the bleakest, contain resources.
367
4.207 Case managers can be trained in how to interview for client strengths, rather than
liabilities and deficits. This facilitates an active, dynamic relationship with their
clients, where each is perceived as a real person. This relationship is central to
successful identification of client strengths, needs and goals.
368 The approach helps
clients use their own capacities, talents and skills towards achieving their goals,
generally using people in their own social and community networks to assist them.
4.208 Goal planning is fundamental to the case management process. Goals must be:
•
Expressed positively;
•
Client focused, realistic;
•
Achievable;
•
Measurable;
•
Easily understood; with
•
One observable outcome per goal.
369
4.209 The goal plan then becomes a living document which is mutually reviewed and
revised, encompassing progress made to date, and barriers yet to be overcome.
Key to achievement of the plan are a series of ten activities:
1
Checking that the goals are positive, clear, measurable and focused on the
client;
2
Praising and rewarding the client when goals are accomplished;
3
Rewarding attempts to achieve goals despite lack of success;
4
Checking that not too many goals are being worked on at once;
5
Checking what resources are required to achieve each goal. These can
include knowledge, skills, support, co-operation, goods, services etc;
6
Recognising what advocacy roles the case manager or significant others may
need to take on behalf of the client;
367 de Jong and Miller 1995 p 320
368 Rapp and Wintersteen (1989) pp 23-32
369 Kisthardt 1992 pp 120-122
Page 80 of 144
link to page 82 link to page 82 link to page 82 link to page 82 link to page 82
7
Checking whether the case manager is pushing the client to do things they
are unwilling to do;
8
Checking the rate of progress – too fast or slow;
9
Reducing the client’s fears about failure or success with a goal; and
10
Encouraging the client’s active involvement in, and ownership of, the goal-
planning process.
370
4.210 Strength based case management has been found to be successful in working with
substance abusers who have returned to employment.
371 372
4.211 A new direction in vocational rehabilitation is increased emphasis being placed on
understanding the psychosocial characteristics of workplaces.
373 These include:
•
Organisational risk factors for job stress;
•
Psychological work demands;
•
Employee control over the work process;
•
On the job social supports;
•
Uncertainty on-the-job; and
•
On-the-job conflict.
4.212 Left unaddressed, these work-site factors could interfere substantially with
employees’ desire to return to work and their ability to maintain employment and
advance in their careers.
4.213 An American programme called Moving Up is a national model in job placement
and retention. Its counselling and vocational staff are hired for their personal skills
and background as mush as any professional credentials. The goal is to have staff
who engage the clients and earn their trust, and work out which approach will
work for each person’s individual circumstances. While it is not considered
essential for case managers and career advisers to have personal histories similar to
their clients, it is seen as a plus that some of the agency staff have some background
in common with their clients, and thus they serve as excellent role models.
4.214 Key characteristics of the agency staff are stated as:
•
Understanding the needs of the students;
•
Knowing the demands of the job market;
•
The ability to motivate people;
•
Understanding the needs of the employers they will be working with, and
•
Having passion and compassion – people with energy, optimism and self-
confidence.
374
370 ibid p 122
371 Pack 2003 p 18
372 Siegal et al 1996 pp93-98
373 Koch and Rumrill 2003 p 2
374 Proscio and Elliott (undated) pp 25-6
Page 81 of 144
link to page 83 link to page 83 link to page 83 link to page 83
4.215 Participation in recreational activities is a critical component of the career
development process, providing opportunities for individuals to explore their
interests and to develop work-related skills. With a growing preponderance of
tedious and unfulfilling occupations, workers are increasingly seeking life
satisfaction through avenues other than work.
375
4.216 Researchers have compiled a list of the benefits of participating in recreational
activities for people with disabilities:
•
An increase in self-determination;
•
Development of friendships;
•
An improvement in physical functioning;
•
Enhanced perceptions of social acceptance;
•
A decrease in negative attitudes towards people with disabilities;
•
The development of socially acceptable behaviours;
•
Establishes life-long leisure pursuits which will be helpful in coping with
(the inevitable) change throughout life.
376
4.217 These benefits then translate into employment related benefits:
•
A reduction in attitudinal barriers to employment;
•
The development of a broader range of occupational interests;
•
The acquisition of transferrable job skills;
•
Increased access to the “hidden” job market;
•
An increase in social acceptance by peers; and
•
The development of coping skills as a buffer against job stress.
377
Recreational involvement is seen as an intermediate step to vocational goal
attainment.
4.218 The level of knowledge of case managers and agency staff about various
programmes and incentives for employing people with disabilities has a significant
impact on the use of these measures. While this seems obvious, research shows
that staff do not always have the appropriate knowledge, and that complicated
administrative procedures do not help.
378
Addressing lawyer and advocate attitudes
4.219 It is perhaps trite to say that the best solution to the problems created by lawyers
and advocates is not to create the decisions to be challenged. This is just not
possible. There always will be some decisions which are not accepted by the
client, and in some cases, they will seek legal or other professional assistance in
challenging the decision.
375 Devine and Koch 2003 p 83
376 ibid p 83
377 ibid p 84
378 Corden and Sainsbury 2001 p 12
Page 82 of 144
link to page 84 link to page 84 link to page 84
4.220 A controlled study on workers with low-back injuries found that the adversarial
system is significantly associated with a poor rehabilitation outcome, partly because
the patient was constantly recounting their symptoms and disabilities on numerous
occasions to lawyers, doctors and the court. This reduced compliance with
rehabilitation exercise regimes, resulting in significant delays. Patients who had
settled claims and then actively sought work found that their history of a claim for
back injury was a significant handicap, and thus a common reason that these
patients indicated they would not go through a court claims process again.
379
4.221 More than 100 top American employment lawyers recently compiled a Top-10 on
what employers do wrong and why employees sue. This list provides useful
reminders on how to treat clients to achieve the most favourable attitude and
response:
i)
Distributing employee handbooks with sweeping language like: "The
company will not tolerate any type of harassment or discrimination";
ii)
Making promises to employees that are difficult or impossible to keep;
e.g., promising future stock options without having a stock option plan;
iii) Having procedures for addressing complaints but not following the
procedures;
iv) Ignoring or failing to make a good faith attempt to resolve employee
complaints;
v)
Failing to deal promptly with emotional situations, letting them fester
and escalate instead;
vi) Forcing former employees to seek legal advice by refusing to discuss
their termination;
vii) Having weak HR departments that rubber stamp questionable
employment decisions;
viii) Using junior HR staff to interview high-ranking company officials
accused of wrongdoing;
ix) Conducting lots of investigations without ever finding anything wrong;
and
x)
Treating terminated employees with disrespect; e.g., giving a twenty-five
year employee a two-week severance package.
380
4.222 The President of the New South Wales Workers’ Compensation Commission
strongly endorses using alternative disputes resolution rather than court based
challenges to decisions. His view is that their no-fault scheme is one of full
disclosure, speedy resolution and non-adversarial techniques. The lawyer’s role is
as an advisor rather than as an advocate in an adversarial situation.
381 He also
379 Greenough and Fraser 1988 p 954.
380 Reynolds March 2001: www.hro.com/news_letters_display
381 Sheahan p 3
Page 83 of 144
link to page 85 link to page 85 link to page 85 link to page 85 link to page 85
noted that almost 100% of cases had settled but only after the litigation was
in
extremis and the bulk of costs incurred, and that senior veterans of the adversarial
legal culture were themselves calling for change.
382
Focus on ability rather than disability
4.223 Probably every study on occupational injuries confirms that the longer workers are
off the job, the less likely it is that they will return to work. Furthermore, staying
at home for long periods does not promote recovery but increases the likelihood of
disability – if disability is their only focus day after day, then they will fall into a
disability mentality.
383
4.224 Initiatives to commemorate 2003 as the European Year for Disabled People
included the challenge to employers to look at the ability, not the disability,
384 and
the establishment of mentoring programmes pairing young people with disabilities
with business mentors. “See the ability, not the disability” is the motto of many
(dis)ability organisations.
4.225 Business in the Community’s annual Awards for Excellence include the Realising
Ability Award as one of 15 award categories. The award recognises best practice
and innovation in addressing disability as a corporate social responsibility and is
supported by the UK Employers’ Forum on disability, the Department for Trade
and Industry and The Financial Times.
385 Past recipients include a company
employing 60 unemployed disabled people in call centre work, and another
providing 1,000 fully accessible and accredited IT training placements for deaf and
hard of hearing people.
4.226 One of the best examples of the success of focus on ability comes from the UN
Food and Agriculture Organisation (FAO), which has been co-ordinating
mushroom production training for disabled farmers in Thailand and Cambodia.
The course is designed for farmers, and teaches all the basics of building a
mushroom house and growing the mushrooms, with the emphasis on food
production not the disabilities. The manager of the programme noted that
“watching these people apply themselves, not only in food production, but also in
their everyday tasks, you realise that their abilities, energy, and resourcefulness are
unlimited”.
386
Addressing co-worker attitudes
4.227 There are few formal initiatives to address co-worker attitudes. For many co-
workers, just gaining a better understanding of the problems of having been
unemployed, injured, or disabled helps address any negative perceptions. Thus,
initiatives which improve the understanding of employers and supervisors are also
appropriate for co-workers. The same applies to agencies wanting to place long
term unemployed or disabled people into employment: understanding the attitude
of employers (and co-workers) is the first step to formulate strategies to best meet
382 ibid p 5
383 Pimentel 1999 p 1
384 Hart 2003 p 14
385 website: <www.btic.org.uk>
386 FAO News 1 December 2000
Page 84 of 144
link to page 86 link to page 86 link to page 86 link to page 86
their needs.
387 Focus groups conducted with a number of Californian employers
revealed that just sitting down and talking through the issues with supervisors and
colleagues was very effective.
388
4.228 Feeling empathy or pain for a person with a disability is a natural emotion. The
person feeling the pain must acknowledge that it is their own pain they are feeling,
and let the pain go away.
389
4.229 Use of “natural supports” helps people with disabilities has been increasing, and
has contributed to better integration of these people into the company workforce,
and better understanding of their needs.
4.230 Using a literature search, two American academics have developed a list of the key
strategies that directly teach skills and provide advice to co-workers.
390 These are:
•
Use a mentor after initial job development, analysis and training;
•
Use job sharing options;
•
Use specifically trained mentors for initial training;
•
Anticipate personnel changes;
•
Establish an ongoing dialogue and regular meetings between all the people
involved;
•
Model appropriate social responses;
•
Be present at social activities to capitalise on potential interactions;
•
Redirect questions / comments to the person with the disability;
•
Reassure managers and co-workers that they can ask personal questions;
•
Build trust between external support agency and work-site personnel;
•
Refine new and existing social networks continually;
•
Use personal contacts to enhance social support;
•
Collaborate between external support agency and work-site managers / co-
workers to develop adaptations and modifications;
•
Facilitate and support involvement of work-site personnel; and
•
Provide consultation on redesigning or organising the work environment to
benefit all employees.
4.231 Help is readily available for co-workers who feel uncomfortable meeting with
people with disabilities. Hints on how to act or what to say when meeting people
with disabilities are widely available in books and on the Internet, such as on
<www.dol.gov/odep/pubs/fact/comucate.htm>
Addressing transport issues
4.232 The ability to get to work and home again on time is vital to maintain steady
employment. Only the United States appear to recognise the importance of
387 Department of Employment and Workplace Relations 2001 p1
388 Sum et al 2001 p 40
389 Pimentel undated
390 Storey and Certo 1996 p 68
Page 85 of 144
link to page 87 link to page 87 link to page 87 link to page 87
transport for low income workers, and the difficulties they face accessing it because
of cost and/or availability.
391 (Other countries provide transport-related assistance
for people with disabilities only). States variously provide free or low cost cars,
loans to purchase cars, financial assistance towards transport costs, and vouchers to
cover petrol or public transport costs.
4.233 Other forms of government sponsored assistance include van/car pools, contracting
services to fill gaps in public transport, allowing low income workers to use
specialist services for elderly / disabled people, using volunteers to drive
participants to work or in emergencies, and lastly encouraging employers to
provide transport.
4.234 In Britain, the possession of a driving licence is known to increase a person’s
chance of obtaining work, and evidence also suggests that people with access to
private transport are more likely to sustain employment.
392 A review of needs
conducted for the British Department of Work and Pensions identified several
activities necessary to assist long term unemployed into work. Termed “mapping
transport provision” it involves:
•
Mapping of existing public transport provision on to a network of major
employers and a network of neighbourhoods where the client groups live;
•
Working with transport providers to provide subsidised services until they
become self-sufficient. It may also involve employers providing some
financial contribution;
•
Developing formal mechanisms for identifying and matching people with
similar transport needs e.g. Through car pools; and
•
Transport to childcare facilities, or providing childcare facilities near public
transport services.
393
4.235 Financial assistance towards the costs of getting to work (ie for taxi fares or to pay
some-one to drive the person) for people with disabilities was seen as fundamental:
arriving reliably on time and ready for work was valued by both workers and
employers.
394
Retaining employment
4.236 The first few months of employment are a critical time for new workers. Most
programmes to assist long term unemployed workers gain employment have
focused simply on the transition into work, with little, if any, emphasis on helping
the former unemployed people retain their jobs in the long term. A British survey
conducted in 1991 identified a range of post employment support programmes
used in OECD countries, mainly in North America. While few of these initiatives
have been formally or rigorously evaluated, the resulting report provides a solid
basis for further policy development. Some of the key concepts identified in the
391 Kellard et al 2002 p 35
392 ibid p 114
393 Kellard et al 2002 p 115
394 Thornton and Corden 2001 Executive summary
Page 86 of 144
link to page 88 link to page 88 link to page 88 link to page 88 link to page 88
research and which have not been discussed elsewhere in this report are listed
below.
395
(a) Earnings supplements / financial assistance to employees
4.237 There is some evidence that earnings supplements may facilitate job retention, but
employees may find it difficult to retain their jobs when the supplementary
payments end. US evidence indicated that providing emergency financial assistance
such as grants or cheap loans can improve job retention. Some post employment
programmes offer advice and training in money management.
(b) Wage subsidies for employees
4.238 Wage subsidies for employers were found to be more likely to increase recruitment
and retention of employees if employers were committed to training and/or other
support for employees. In Ireland and Germany, the viability of social enterprises
depends on such support.
396 A major Finnish study found that disabled people in
subsidies work has positive images of work while their employers had positive
images of these workers. Up to a third of these workers in subsidised employment
found work in the open labour market.
397
4.239 Experience, including in New Zealand experience in the mid 1990s, did not show
good job retention rates once the subsidy payments ceased. British researchers
found there was criticism of such financial measures if they did not have conditions
attached to them, such as maintaining employment when the subsidy period had
ended.
398
(c) Retention incentives for employers and /or employees
4.240 Retention incentives are used extensively in the United States, to encourage
workers to remain in employment and employers to retain their recently employed
workers. They are usually one-off payments made at previously defined milestone
points, normally a specified number of months in employment. Incentive
payments vary widely across the states.
4.241 Britain introduced a Back-to-Work bonus for benefit recipients in 1996 to
encourage people to maintain contact with the labour market. One evaluation
suggested that the Bonus itself did not encourage people into part-time work, rather
that the promotion of the bonus educated people that part-time work was a
legitimate activity.
399 Respondents to another evaluation indicated that the Bonus
would have little effect on helping them move into full time work as:
•
Some respondents (mainly men) wanted full time work only, and would not
contemplate part-time work;
•
Benefits were felt to offer more security than a full time job;
395 Kellard et al 2002 p 2
396 Thornton and Lunt 1997 p 309
397 ibid p 85
398 ibid p 309
399 Ashworth and Youngs 1998 Executive Summary
Page 87 of 144
link to page 89 link to page 89 link to page 89
•
Some respondents wished to work only part-time, and also there was a
perception of a lack of suitable part-time jobs.
4.242 Additionally, the Bonus was seen (negatively) as an enforced savings measure, as it
comprised half the money earned above the earnings disregard that was deducted
from their benefits.
400
(d) On-job support
4.243 New employees moving to work after an absence often require assistance to adapt
to a number of aspects of their job. This includes:
•
Job coaching. This is practical assistance on-the-job, such as demonstrating
what is to be done, how to organise the work, getting on with colleagues,
ensuring punctuality;
•
Mentoring. This gives the new employee a one to one relationship with a
co-worker or an external party (called a mentor or a buddy) who helps the
new employee adjust to the workplace and the routine of being back at
work. In the united states, mentoring has had significant impact;
401
•
Peer support groups. Some united states welfare to work programmes
include these, whereby new employees share experiences and solutions with
others in similar positions. It may also include additional training or
workshops on issues such as budgeting, time management, conflict
resolution and workplace communications. Problems with these included
timing and location of sessions;
•
Telephone help-lines. These are toll-free hotlines to assist individuals with
emergency or routine problems which might cause them to lose their jobs.
Such problems include childcare, transportation, accommodation, food,
substance abuse, health, domestic violence, and family stress. The marriott
hotel chain credits its telephone resource service (staffed by social workers)
with reducing tardiness, absenteeism and turnover;
402
•
Post-employment education and training. Some schemes provide training at
the work-site, others provide training outside standard workplace hours.
Such skill training must closely match the needs of the employees and the
employers, as well as fit with work and home schedules. Cost can be an
issue to both employers and employees, and some governments provide
financial assistance; and
•
Training employers in job retention techniques. Such training includes
developing appropriate attitudes, listening skills, conflict resolution,
teamwork, as well as how to provide employment counselling services, hire
ex-offenders, identify any government tax credits for employees, and
manage employees with specific problems such as substance abuse.
4.244 Retention efforts should begin before employment, and should be built in to
employment preparation and placement programmes. Evaluation of the first major
demonstration project (the PostEmployment Services Demonstration) to examine
400 Thomas et al 1999 Executive summary
401 Kellard et al 2002 p 92
402 Hershey and Pavetti 1997 p 83
Page 88 of 144
link to page 90 link to page 90 link to page 90 link to page 90 link to page 90
the effectiveness of providing case management services to newly employed welfare
recipients indicated that services must be targeted differently for different clients,
that service delivery needs to be as simple as possible, and that close links are
needed with employers.
403
(e) Protection of employment
4.245 Employment protection for injured or disabled workers is quite prevalent in
Europe and North America, although the actual provisions vary widely. In the
Netherlands, disabled workers may be dismissed only with the permission of the
Employment Service. As a rule, a labour contract should not be broken within the
first two years of a worker’s disability.
404
4.246 Spain has provision to ensure the re-instatement of disabled workers once they
have completed the relevant rehabilitation process. Those with a permanent partial
disability are entitled to be re-employed by the same firm, either in the same job
with a similar wage level if output remains normal, or in a job adapted to residual
capacity without a drop in wage or more than 25%. In the latter case, a trial
period of adjustment maybe permitted for up to six months.
405
4.247 Belgium provides compensation to employees if dismissal is for neither economic
nor urgent reasons which prevent the continuation of the contract. Some
protection applies during the first six months of incapacity, unless the employee’s
injury is sufficient that they are unable to continue working.
406 In most countries,
dismissal of a disabled worker is subject to standard legal provisions for
employment protection, and anti-discrimination requirements.
4.248 Provisions requiring employers to keep on staff who have been injured do not
recognise that in some cases, there may be a pre-injury poor relationship between
the employer and worker for reasons such as performance problems or staff
relationships. Compulsory re-employment of the worker may not be in either
employer’s or worker’s interests.
(f) Quota systems
4.249 Quota systems represent a long standing European policy approach to the
employment of people with disabilities. Generally it is a legal requirement for
public and/or private sector employers who employ a specified number of workers
that a set percentage of these employees should be people with some specified
disabilities. Quota schemes are generally complex, and in some cases contentious.
4.250 Greece operates a quota system of compulsory employment for members of seven
specified groups for all employers with 50 or more staff at a rate of 7% of the
workforce. The seven groups include war veterans and their families, people with
disabilities, and parents with more than five children in full-time education.
407 While the membership of quota groups varies in detail, all include people with
disabilities.
403 Relave 2000
404 Thornton and Lunt 1997 p 198
405 ibid p 233
406 ibid p 43
407 ibid p 145
Page 89 of 144
link to page 91 link to page 91 link to page 91 link to page 91
4.251 Quota percentages are variable (for instance France has six percent, Austria four
percent). Some occupations are also exempt, as in France where people who drive,
navigate or travel on board, and workers in jobs which involve heavy physical
labour.
408 Some countries provide rewards for employers who exceed the required
quotas, while others, like Austria, count a blind person or a wheelchair user as two
disabled people for quota purposes.
409
4.252 Some countries allow companies which do not achieve their quota to make a
financial contribution to a special fund, which then is used to finance training and
job creation for disabled people. Experience has been that firms pay into the funds
simply as a way of discharging their statutory responsibilities, rather than
demonstrating any commitment to employ people with disabilities.
410
4.253 Many American states have a “preferred worker” programme, which offer
incentives to employers to take on rehabilitated injured workers who were not
previously on their own staff. Again, the details of schemes vary between states,
with some (like North Dakota) showing available jobs on the Internet. Incentives
include not paying workers’ compensation premiums for such workers for a set
period, repayment of additional expenses in starting a new job, subsidy on wages
for a specified period, and payment of the costs of modification of workplace
premises.
(g) Levy systems
4.254 Levy systems differ from quota systems in that employers make a financial
contribution to s special fund, in lieu of employing the target proportion of
disabled people. Such a contribution may be permitted as a last resort when the
possibility of direct employment has been exhausted, or it may be a legitimate
choice. Levies are usually collected into a special rehabilitation fund and
redistributed variously to employers, disabled workers or service providers.
411
4.255 Levies can also be used to implement labour market measures to improve the
prospects of disabled people (as in Western Europe and Japan) or as financial
incentives to employers to hire workers (as in Eastern Europe and China) where
the finance is seen as compensation for employing a less productive worker.
4.256 The aim of levy systems is to maximise employment rather than to collect revenue.
It is seen as an equalisation measure.
Self-employment
4.257 Self-employment offers many the freedom to work at their own pace in an
environment that accommodates their special needs. Owning their own business
often provides the flexibility that is necessary to those who require frequent
medical attention, flexible hours, accessible work space, or other special
considerations. Self-employment does present many challenges and is not for
everyone, but for many people with disabilities and chronic health conditions, self-
employment offers the hope of making a living and achieving self-sufficiency.
408 ibid p 97
409 ibid p 28
410 Lunt and Thornton 1994 p 235
411 Thornton 1999 Introduction
Page 90 of 144
link to page 92 link to page 92
4.258 Starting a business requires a significant commitment of time, energy and
resources. In addition, the individual must have some marketable skills or a
product or service with a demonstrated market demand. Any person pursuing
business ownership must be prepared to make personal sacrifices and be willing to
learn the "how to's" of starting and successfully managing a business enterprise
before they start up the business.
4.259 In some countries, it is relatively rare for people with disabilities to become
economically active through running their own business. In the United Kingdom,
Business Ability is a successful project (95% success rate) dedicated to developing
self-employment as an option for disabled people.
412 It provides the following
services:
•
Home visits;
•
Initial assessment of suitability of self-employment option;
•
Benefits advice;
•
Help to appropriate financial assistance / grants / bursaries / preferential rate
loans;
•
Access to ongoing business training and marketing opportunities;
•
Access to free computers through fast track application; and
•
Ongoing business mentor support.
4.260 The UK also has a New Deal programme for self-employment. Like other New
deal programmes, this uses the system of a Personal Adviser to help and support
clients before and during the programme, and for up to two years after the worker
leaves the programme. A training grant of us to £1500 can be used for courses on
how to run a business, or to buy expert advice and guidance on getting established.
A period of six months is allowed for “test trading”. The worker receives an
allowance equivalent to their Job-seeker’s Allowance plus a top-up grant. Any
money the business makes goes into a business account which is jointly managed
between the worker and their training provider. The money in the business
account can be used only for spending on the business until the test trading period
is over.
413
4.261 This allows the newly self-employed worker to promote their business and build up
their customer base. They can trade and make mistakes without risking their own
income. At the end of the test trading period the money in the business account is
available to use in the business or to keep as a contingency. If at any stage, the
worker decides that self-employment is not for them, they can return to the main
new deal programme to find paid employment.
4.262 The Prince’s Trust Business Programme provides assistance to 18 –30 year olds to
start businesses. It focuses particularly on those who are unemployed, under-
skilled, leaving the criminal justice system or care. To receive funds, applicants
must have been refused funding from other sources, although roughly half the
businesses did receive other financial support. Approximately three-quarters of
businesses supported by the Trust were still trading 18 months after start-up.
412 Riddell 2002 p 43
413 New Deal: Self-employment brochure
Page 91 of 144
link to page 93 link to page 93 link to page 93 link to page 93
4.263 Characteristics of the owners of businesses which survived include:
•
White ethnic origin;
•
Older rather than younger;
•
Had a family background of self-employment (one or both parents had been
self-employed at some stage);
•
Had a neutral or averse attitude to risk taking;
•
Were motivated by a desire for independence and lifestyle rather than
growth or income; and
•
Were generally better educated (with some tertiary qualification).
Business owners’ characteristics such as gender, disability and household
circumstances did not lead to any clear differences in business survival rates.
414
4.264 Men are more likely than women to enter self-employment from benefit, and they
tend to move into sole trade or low capital, labour intensive business. Earnings are
typically low and hours worked high. Success in self-employment for males is
associated with the presence of a spouse or partner and children, and the most
successful tend to be aged 25 – 45. Higher qualifications and a good employment
history or previous exposure to self-employment are also good indicators of
success.
415
4.265 In the United States, people with work disabilities are twice as likely to be self-
employed as the rest of the population.
416 The U.S. Small Business Administration
provides millions of dollars each year to support the initiatives of micro businesses.
The Office of Disability Employment Policy works with them to extend training
and financial support in order to increase the numbers of self employed people
with disabilities. In addition,
state vocational rehabilitation programs provide a
variety of services to aspiring entrepreneurs with disabilities.
4.266 The Research and Training Centre on Rural Rehabilitation Services (RTC:Rural)
has developed a best practice model for small business development, based on
research into the practices of all the states and their own extensive experience.
417 The model reflects the importance of the consumer doing the development work,
rather than the counsellor.
4.267 There are eight components in the model:
1.
The vocational rehabilitation provider assesses a consumer’s business
potential;
2.
The consumer develops a business idea, explores its feasibility, and
conducts a market analysis;
3.
The consumer gets any necessary education and training;
4.
The consumer obtains technical/ professional assistance to develop a
business plan;
414 Meager, Bates and Cowling 2003 pp 2 - 3
415 Kellard et al 2002 executive summary
416 Ravesloot and Seekins 1996 p 189
417 RTC:Rural web-site www.ruralinstitute.umt.edu
Page 92 of 144
link to page 94 link to page 94 link to page 94 link to page 94
5.
The consumer writes the business plan;
6.
The consumer determines the availability of, and applies for, funding
from other sources (note that in the first American study of people with
disabilities who are self-employed, more than half the respondents made
initial investments of less than $10,000);
7.
The vocational rehabilitation provider reviews the self-employment
plan; and
8.
The vocational rehabilitation provider monitors the business’s progress.
4.268 The range of businesses established is extensive and includes retail, professional
services, repair services, arts and crafts, entertainment, building trades, automotive
services, farming, health services and office services.
4.269 For some people with disabilities and injuries, self-employment still requires some
support systems. This is similar to the standard business model: the smart strategy
in planning for entrepreneurial work is to be aware of strengths and skills, and to
build on these, while recognising limitations and needs and either building these
skills or locating sources of support.
418 Regrettably, the social service community
tends to hold the belief that requiring on-going support means that a person is not
sufficiently capable of making decisions.
4.270 Notwithstanding the success of some of these small businesses, self-employment is
not a substitute for proper job development, systematic instruction and natural
support. Fear of the community, poor job development technique, limited vision
when facilitating supports and misunderstanding of funding streams is cited as
deriving self employment in a few cases.
419
Operating within prevailing labour market conditions
4.271 Over the last twenty or so years, the state of the labour market has been changing.
As far back as 1997, research in Britain was indicating that regular nine-to-five jobs
were becoming a rarity. Employers were able to operate with different types of
labour force: some wanted a multi-skilled, stable labour force while others
preferred to sub-contract and hire temps.
420 Workers also had varying preferences
about the range of tasks they were called on to perform, and the hours of work.
Many preferred to work flexible hours in order to meet family and other
responsibilities.
4.272 The New Zealand labour market has also become more flexible from the employers’
point of view, perhaps less so from the workers’ viewpoint.
4.273 The recent American recession hit the white collar and IT sectors for the first time.
Executive level employees were remaining unemployed for longer than lower paid
employees.
421 In that about 85% of job-seekers were finding jobs through some-one
they knew, the solution was the development of a formal system for networking for
418 Rizzo 2002 p 100
419 Griffin and Hammis p 1
420 Casey et al 1997 Executive summary
421 Loeb 2003
Page 93 of 144
link to page 95 link to page 95 link to page 95 link to page 95
senior executives and managers. The clients of this firm were generally people
with six-figure salaries, and experience at company vice-president level. They had
a wealth of professional skills, but nothing in the way of job-seeking or networking
skills. The programme included preparation and presentation of resumes in such
style that these would be seen at the top of the pile of resumes. Outplacement firms
estimate that the average length of job for senior level executives is now between 22
and 36 months, meaning that older / senior executives could find themselves
changing jobs several times before retirement.
422
4.274 Job rotation was introduced as a pilot initiative in Denmark in 1992. Its apparent
success has stimulated interest from across Europe, including the UK. Job Rotation
involves unemployed people being trained in the skills needed for a specific job in a
specific company. They then join the company for an agreed length of time and
take over the job of an employed person. The employed person is then able to take
time out for training. At the end of the period the employer can decide either to
dismiss or retain the unemployed person.
423
4.275 The strength of networking for senior employees is supported by Richard Bayer,
CEO of the Five o’clock Club, a national American career coaching organisation.
424 They recommend using social events such as corporate Christmas functions to
network, and access potential employers. These people are normally too busy to be
available for cold calling, and the relaxed atmosphere gives the job-seeker a chance
to show their personality, their listening skills, and their knowledge.
4.276 The job market for middle managers is generally a very tight market, as firms move
to reduce layers of management. One assessment in America is that 20% of those
unemployed for more than six months are former executives, managers or
professionals.
425
4.277 From time immemorial, it has been assumed that governments have a duty to
provide for the poor, and this includes providing jobs. In a dynamic economy,
there is always a certain amount of unemployment, because industries contract
(while others expand), people leave jobs voluntarily for a variety of reasons,
demand for goods and services change, currency valuations fluctuate, and
technologies change. One means of dealing with unemployment is to provide
taxpayer funded job creation programmes, with subsidies ranging up to 100% of
the costs of wages and overheads. A strong message from much of the research is
that these programmes will distort the prevailing labour market conditions, not
necessarily for the best.
4.278 Britain introduced a National Insurance Contributions (NIC) Holiday in April
1996. It enabled employers to recruit employees who had been out of work and
receiving benefits for at least two years, and to claim back one year’s worth of NIC
contributions. Take-up of the scheme was low, and an survey of employers
revealed that awareness of the scheme was low, and the contributions holiday was
422 Loeb 2003
423 Hutchinson 1999 pp175-9
424 Five o’clock Club website: www.fiveoclockclub.com
425 Graves 2003
Page 94 of 144
link to page 96 link to page 96 link to page 96 link to page 96 link to page 96 link to page 96
too small to be of value to large firms, but for small firms the risk of taking on
unsuitable workers was not outweighed by the holiday.
426
Multi-targeted Programmes
4.279 Programmes with a mix of activities tended to help with the widest range of
individuals.
427 Targeting resources towards the most disadvantaged people and
developing programmes to meet their needs did help them. A mix of job search
and education increases earnings for most for the broadest range of individuals.
4.280 Several programmes have recently been initiated in the United States to help the
hard-to-employ find work. These reflect the time limits (usually 5 years) placed on
the length of time a family can receive welfare support. While formal evaluations
are not planned until 2004, there are components of these programmes which are
useful to study. Each programme has been implemented at several sites across the
states to enable wider evaluation.
4.281 Enhanced Services for the Hard-to-Employ
428 is designed to field and evaluate
innovative ways to boost employment, reduce welfare receipt and promote well-
being in the target population. The programmes include:
•
Supported work, in which people are given subsidised jobs along with
training and job search assistance until they find regular jobs;
•
Initiatives which combine mental health treatment and employment
services;
•
Improved identification of those with serious employment barriers to
increase their participation and retention in mental health or substance
abuse treatment; and
•
Two generation interventions that offer services for pre-schoolers or
adolescents in parallel with services for their parents.
4.282 Belgium provides a 14 week training course for lower educated unemployed aged
between 18 and 40 years of age.
429 Working in small groups of up to eight people
for 30 hours each week, the training comprises technical training, counselling and
guidance including job search assistance, and language and mathematics training.
The training include traditional educational methods, demonstrations, individual
and group work, role plays, industry visits, and on-job practical training
placements. They have a charter for job seekers which affirms the right of every
job seeker to receive personal and intensive support to help their re-integration into
the labour market.
430 The provision of this assistance is completely separated from
the provision of income support, which they encourages the building of trust
between the long term unemployed and those trying to help them. Participation is
voluntary with a reported success rate of 60%.
431
426 Snape 1997 Executive summary
427 Michalopoulos 2000 Executive summary
428 MDRC <www.mdrc.org>:
429 Geers 1991 p 58
430 ibid p 62
431 ibid p 64
Page 95 of 144
link to page 97 link to page 97 link to page 97
4.283 In August 2003, the New Zealand government introduced Jobs Jolt, a programme
of 10 initiatives aimed at getting people off benefits, into employment and to
address the shortage of skilled labour, at a cost of more than NZ$100 million.
432 The initiatives include:
•
Active case management for older workers, by reducing case management
ratios for older workers and giving clients more active and job-focused
assistance, including training in workplace skills such as computer literacy;
•
Employment coaching, one on one to specific groups of job-seekers to
address their employment barriers, increase their value to employers and to
improve their chances of moving into sustainable and higher quality
employment. Specialist providers will work with clients to assess their
needs, help them set suitable work goals, and gain employment. Support
will be continued for six months once clients are in work;
•
Extra help for those unemployed for more than eight years, including one
on one specialist assistance to address their specific barriers. It is expected
that this programme will also help the Ministry better understand the
reasons behind long term unemployment;
•
Job partnerships between Work and Income and industry. A National Co-
ordinator will oversee the development of industry partnerships.
Programmes will focus on training targeted to meet skill and labour
shortages identified by industry, and may include on the job training, work
experience or pre-employment training;
•
Pilot programmes for enhanced service and case management for sickness
and invalid beneficiaries. One pilot will address enhanced case
management, helping clients set goals, develop individual plans addressing
their strengths, needs, barriers, and key issues. Another pilot will be an
expansion of the Job Club for job-seekers with disabilities who are near
work readiness; and
•
The other initiatives include clarifying the responsibilities of the
unemployed receiving benefits, improving communities’ ability to access,
participate in and efficiently use information communications technology,
and assistance to the Mayor’s Task Force for various projects.
4.284 A successful programme in Portland emphasised participation in a range of
activities, tailored services individually, and stressed job quality. The programme
substantially increased participation in education and training programmes
(particularly post-secondary education and training) and helped recipients gain
general and occupational qualifications.
433
Results based funding
4.285 In results-based funding models, rehabilitation providers are compensated
according to the measured outcome of the service they have provided. The model
depends on being able to identify and measure appropriate components of targeted
outcomes to which payments can be attached. The results are the impact on
participants of the results of the programme.
434 The concept resulted from
432 Ministry of Social Development website: www.msd.govt.nz
433 Martinson and Strawn 2002 p 2
434 Corden and Thornton 2003 p 8
Page 96 of 144
link to page 98 link to page 98
concerns about the apparent stagnation of supported employment in America and
Britain in the 1980s, and from the need for greater accountability in achieving
outcomes.
4.286 Of the several models reviewed, the Oklahoma Milestones is considered a success
and has been highly influential. The model used six milestone payments for
outcomes:
1
Assessment;
2
Job preparation;
3
Job placement;
4
Four weeks retention;
5
Ten weeks retention; and
6
Closure
4.287 There were two levels of funding (regular and highly challenged), reflecting
different needs for preparation and enabling providers to offer appropriate levels of
service. Quality standards were incorporated in service requirements for each
benchmark payment. Fundamental to the model is the concept of scoring /
categorising individuals in order to be able to pay providers more for provision of
services to those in greatest need. This was designed as a counter-measure to the
risk of creaming off first all those most easily assisted.
4.288 Britain introduced a comparable programme called WORKSTEP in 2001. A review
conducted in 2002 focused on the potential disadvantage of the model, that there
could be adverse selection of people in the programme in response to financial
incentives or disincentives perceived. In the UK context was an increasing
rejection of the categorisation of people on the basis of disability and a growing
support for a social (rather than medical) model of disability.
435
4.289 The next research focus is on investigating what WORKSTEP accomplishes for
individual disabled people and understanding how outcomes are achieved. Case
studies of selected providing organisations involve depth interviews at two points
in time with staff, clients, employers and Jobcentre Plus advisers. The case studies
will be complemented by a small number of one-off studies of the delivery
processes and outcomes. In the longer term, the evaluation strategy will address the
overall impact of the programme and cost-effectiveness.
Concluding remarks
4.290 The most successful programmes are those in which staff believe that participants
can succeed and convey that expectation from the onset of programme
participation.
436 Best practice includes:
435 ibid p 41-2
436 Brown 2001 p 43
Page 97 of 144
Setting and maintaining goals:
•
Set high expectations for success
•
Clearly articulate and consistently enforce programme rules
•
Set goals for programme performance and monitor success
•
Model programme expectations on the workplace
•
Focus on strengths, skills and interests rather than on barriers
•
At all stages, maintain a clear focus on the goal of employment
•
Define success in the context of employment
•
Identify both short and long term goals, with interim benchmarks of success
Helping participants:
•
Help participants explore their interests and options
•
Monitor attendance and progress in all activities and services
•
Keep participants motivated to move forward
•
Promote access and support for all participants
•
Make an active commitment to serve all individuals, including those with
serious barriers to employment
•
Provide a range of support services to address participant needs
•
Teach participants to conduct their own job search
•
Invest adequate resources
•
Develop personal and trusting relationships with participants
•
Use employment plans as comprehensive case management tools
•
Help participants help each other
•
Help participants get the best job they can
Supporting staff
•
Provide staff with training, flexibility and support
•
Give staff a clear mandate to serve individuals with barriers
•
Provide regular, ongoing training for staff
•
Provide multiple opportunities for staff development and support
•
Form partnerships with agencies that have experience serving individuals
with barriers
•
Give staff the time they need to help participants with barriers
•
Give staff the flexibility and tools to address individual needs
•
Have (some) staff who have faced the same barriers as participants
Working with employers
•
Work closely with employers
•
Use aggressive job development to increase opportunities for participants
•
Build long term relationships with employers
Page 98 of 144
link to page 100 link to page 100 link to page 100 link to page 100
•
Involve employers in programme design and implementation
•
Focus on individuals’ strengths rather than barriers when marketing them to
employers
•
Address stereotypes and misconceptions about individuals with barriers
•
Look for jobs with companies that provide a supportive work environment
Follow up
•
Continue to support participants after employment
•
Build in post-employment services as a formal programme component
•
Pay careful attention to the transition to work
•
Facilitate access to transitional benefits
•
Use post-employment follow-up to achieve multiple goals
•
Help participants to up-grade their skills and advance to better jobs
4.291 There is no one model for designing assistance. Some problems must be addressed
before individuals begin work, others while they are working, and still others may
not be evident until after they have begun to work. Programmes must be able to
use multiple strategies at different intensities and in different combinations to be
able to meet the needs of participants.
437 Flexibility is the key to assisting
individuals with multiple barriers. Care must be taken to avoid participants
becoming overwhelmed – success will normally be incremental, and recognising
this will help participants stay motivated.
438
4.292 Research conducted in the 1980s found that job-search-first programmes might
speed up the return to work of welfare recipients, but the jobs tended to be short
lived and poorly paid. This left many people living in poverty, back on welfare,
and still severely disadvantaged.
439 The important message in the evaluation of
policies and programmes is that one size does not fit all, and that each initiative has
strengths which have benefited at least some of the participants / recipients.
4.293 “Leaving welfare is a process, not an event.”
440 Getting a job is only one step in a
long sequence of steps: building confidence, developing personal skills, acquiring
job readiness skills, and triumphing over setbacks. Even in very supportive
programmes, high rates of job loss can occur.
437 Brown 2001 p 5
438 Brown p 54
439 Hamilton G p2
440 Hershey and Pavetti 1997 p 84
Page 99 of 144
link to page 101 link to page 101 link to page 101 link to page 101 link to page 101
5
Part 4: Best Practice
5.1
Experts caution that consideration of borrowing practices from other countries
must include an analysis of the unique economic, social, and political elements in
each country. What works well in one country will not necessarily work well in
another, due to different definitions, compensation / benefit payment structures,
cultures, and labour markets. Research has shown that Germany, Sweden, and the
United States, for instance, have all attempted to make improvements in their
disability programmes by introducing new requirements, practices, procedures and
incentives, but not all have proved to be successful.
441 Equally, it can be difficult
to pinpoint which specific new practice which might have been successful, as new
practices are rarely carried out in isolation.
5.2
The US General Accounting Office investigated practices for improving rates of
return to work for people with disabilities. They cite three specific practices which
have been proven successful in Sweden and Germany. These are:
•
Intervening as soon as possible after a disabling event to promote and
facilitate return to work;
•
Identifying and providing necessary return to work assistance, and
managing cases to achieve return to work goals; and
•
Structuring cash and health benefits to encourage people with disabilities to
return to work.
442
5.3
The State of Wisconsin has been at the forefront of policy development to reduce
welfare dependency but analysts are divided on which policies were successful.
One concluded that emphasising getting any job is more successful than aiming for
a good job or undertaking training, and that successful schemes enforce
participation with a clear threat of sanctions.
443 Another believes that the decline
in Wisconsin’s welfare caseload resulted from a combination of circumstances
(strong economy, restricted benefit eligibility and payment levels) which will not
be repeated.
444
5.4
The experience of the New Zealand Employment Service in the 1990s with its Job
Action programme was that, while the programme was moderately successful, the
numbers of long term registered unemployed job-seekers reduced in part because
people allowed their registrations to lapse rather than participate in the
programme. This effect has been noted in a number of similar international
programmes.
445
5.5
Many American states have introduced sanctions on welfare clients for not
participating in programmes. Sanctions have a range of purposes:
•
Purging the caseload of people who are not interested in working;
•
Purging the caseload of those who have alternative means of support;
441 Sim 1999 p 41
442 ibid
443 Mead (1998) p 23
444 Wiseman 1996 p 516
445 Eardley and Thompson p 29
Page 100 of 144
link to page 102 link to page 102 link to page 102
•
Giving a clear message that help is available but only if people are serious
about getting a job, and only for a short period of time; and
•
Helping to motivate clients who might not otherwise participate in
activities to promote self-sufficiency.
446
5.6
Sanctions range from reductions in, or cessation of, welfare payments to
requirements to participate in specific treatments (such as substance abuse, mental
health counselling, or parent training).
5.7
Researchers have also found that mandatory participation requirements are not
always necessary, and some programmes have found that there are more people
keen to attend than the organisers have resources to serve.
447 What is important,
however, is
1
To make expectations of participants clear from the start;
2
To provide the services which were offered (including training, and real
job opportunities); and
3
Where applicable, to impose the penalties that were threatened.
5.8
To achieve this, organisers of programmes must understand and work with the
local labour market. Resources must be devoted to:
•
Cultivating relationships with firms and industries;
•
Developing jobs for particular individuals;
•
Keeping abreast of technical and occupational changes which dictate the
skills required in the workplace; and
•
Knowing the current state of the local labour market – employment growth
areas, unemployment rates, prevailing wage rates and general demography.
Evaluation of programmes
5.9
Formal evaluations are available for only a small percentage of initiatives which
help the long term unemployed obtain and retain employment. A comparison of a
range of American programmes is attached as Appendix Five. Costs per person for
the eleven programmes ranged from US$ 16.50 to US$1,706 per month.
Employment rates achieved varied from 31% to 80%. Average monthly earnings
ranged from $85 per month for young mothers to $500 for adult women.
448
5.10 Evaluation should ideally be built into any new programme, and implemented
early. Useful questions to be addressed in evaluations include:
•
Are the programmes and policies being implemented as intended?
•
What are the reasons for these findings
•
What are the implications of the findings for future directions?
•
What are some of the barriers?
446 Nightingale and Holcomb1997 pp60-1
447 Nightingale and Holcomb 1997 p 61
448 ibid pp56-7
Page 101 of 144
link to page 103 link to page 103 link to page 103 link to page 103
•
How can the barriers be overcome?
449
5.11 Success indicators for disability programmes include quality of life and cost
effectiveness.
450 Quality of life incorporates independent living, community
inclusion, integration as well as employment.
Principles of good intervention design
5.12 The basic principles underlying successful interventions as listed below were
derived in the Michigan studies in the late 1990s.
451 Interventions which raise
ability to survive events could be required as a result of redundancy,
unemployment, serious illness / injury of self or in the family, loss of property. The
variance in such events means that any intervention needs to be tailored to the
event, while retaining the focus on obtaining and retaining employment.
5.13 For success in finding re-employment, there are six key tasks a job seeker must be
able to handle:
1.
Identification of transferable skills;
2.
Identification of the market for those skills;
3.
Procuring interviews with employers;
4.
Communicating their skills and value to a prospective employer;
5.
Emotional, attitudinal, and behavioural management of setbacks and
barriers; and
6.
When receiving a job offer, the ability to negotiate and make the best
choice.
452
5.14 Programme organisers must recognise that for many of the participants, the
training will be the first education or training since leaving school. The following
nine steps have been identified:
1 Recruitment of participants is the start of the intervention
This includes identifying the right people to participate in an intervention (as not
all people will benefit from one), persuading them to participate, and actually
getting them there for Day 1. Potential clients must recognise the need for
intervention and accept their role as an active participant. Any barriers to
participation such as childcare or transport must be removed.
2 View intervention as a social influence
A relationship of trust must be established between client and the “interventionist”
(i.e. they will act in the client’s best interests and respect the client’s needs).
Trainers need to present relevant credentials such as own experience of the client’s
449 Perrin p 113
450 ibid
451 Caplan, Vinokur and Price 1997 pp371-4
452 Caplan, Vinokur and Price 1997 pp 354-5
Page 102 of 144
link to page 104
situation, and specialist training for managing such interventions. In group
sessions moderate use of self-disclosure can help participants recognise their
experiences and feelings are normal.
3 Target motivation, skills, knowledge and resources for coping
Help participants build strategies for coping with setbacks, barriers, and lapses in
using these strategies. Move progressively into successively more challenging
situations which utilise the skills just learnt. To take an example from the
Michigan programme, job seekers learn how to conduct job seeking telephone calls
first by watching the trainers model the wrong way, next by generating suggestions
for improvement, then role-playing the correct approaches before applying their
new skills in live situations. Positive feedback is an essential aspect, from both
trainers and peers.
4 Build self-sufficiency
An intervention may not provide all the resources for successful coping, but it
needs to enhance the participants’ existing skills, motivation and knowledge so that
they have the key resources available to them.
5 To be successful requires the confidence to try to succeed
As previously stated, the likelihood of gaining re-employment depended more on
having the self-confidence to seek out jobs than on the actual skills used in doing
so.
6 Allow for individual differences
This is essential to maximise levels of individual achievement. Not only do people
have different needs, they have different abilities to benefit from interventions.
People are influenced by a range of factors including their own life experiences,
their values and beliefs. Programme providers need to recognise that the best
results are achieved when they deal with participants according to participants’
values and beliefs, not according to the organisers / presenters’ beliefs.
7 Use active teaching and learning methods, rather than didactic techniques
Active learning leads to better skill acquisition and utilisation and reduces the
person’s resistance to adopting new skills.
453 Active learners energetically strive to
take a greater responsibility for their own learning. They take a more dynamic role
in deciding how and what they need to know, what they should be able to do, and
how they are going to do it. Their roles extend further into educational self-
management, and self-motivation becomes a greater force behind learning.
8 Blend active learning with model demonstration, graduated utilisation of skills
and positive feedback
No one technique will achieve 100% effectiveness by itself but using a combination
of techniques gives participants greater opportunities to both learn and use new
skills.
453 Caplan, Vinokur and Price 1997 p 358
Page 103 of 144
link to page 105 link to page 105 link to page 105 link to page 105
9 Inoculate against setbacks
Slips and lapses into previous behaviours, attitudes and moods are the norm, not
the exception, as is the likelihood of rejections. Interventions should prepare
participants for these eventualities, developing strategies and practising techniques.
Topics include recognising what could go wrong (in say a telephone interview),
how the job seeker is likely to feel about this, what they are then likely to think,
and how to deal both with the possible dysfunctional thoughts and actions that
normally are associated with a setback and with the actual activity which went
wrong. Successful job seeking is a long string of
no’s followed by a
yes. Every no
is one
no closer to a
yes.
Predicting who might become long term unemployed
5.15 Various studies have attempted to identify those individuals who, when first
registering as unemployed or becoming injured or disabled, are likely to be at high
risk of becoming long term unemployed. Many programmes of assistance are
restricted to people who are already long term unemployed, on the assumption that
most people who become unemployed do find fins work again within a few months
with minimal assistance from public sources. Researchers generally agree,
however, that by the time the long term unemployed are offered additional
assistance, they are generally in need of considerably more help than when they
were first unemployed.
454
5.16 The problem of predicting whether any particular individual will become long term
unemployed is quite distinct from the general risk factors of long term
unemployment, such as older age, low levels of education and skills, poor health,
unstable employment history etc.
5.17 Payne and Payne predict that in a group of people with poor educational
qualifications newly registered as unemployed, 60% will find work fairly quickly,
and 40% will become long term unemployed.
455 Their feasibility study to develop a
methodology to identify the high risk unemployed people concluded that such a
methodology was available but sufficient errors resulted that different decision
rules were required. The key trade-off was between maximising the chances of
identifying the future long term unemployed and minimising waste of resources by
providing services to clients who do not need them.
456
5.18 A Swedish study of patients with chronic back pain found that the best predictor of
return to work was the patient’s own beliefs about their return to work.
457 Other
key predictors were the patient’s perception of low support at work, their
perception of physical work demands and work danger, and levels of depression
and pain intensity. The researchers developed a screening instrument, the
Obstacles to Return to Work Questionnaire, which proved to be a relatively good
predictor of sick leave. (A copy of the questionnaire is attached as Appendix Two).
454 Payne and Payne 2000 p 7
455 ibid p 8
456 Payne and Payne 2000 pp21-2
457 Marhold, Linton and Melin 2002 p 73
Page 104 of 144
link to page 106 link to page 106 link to page 106 link to page 106 link to page 106 link to page 106
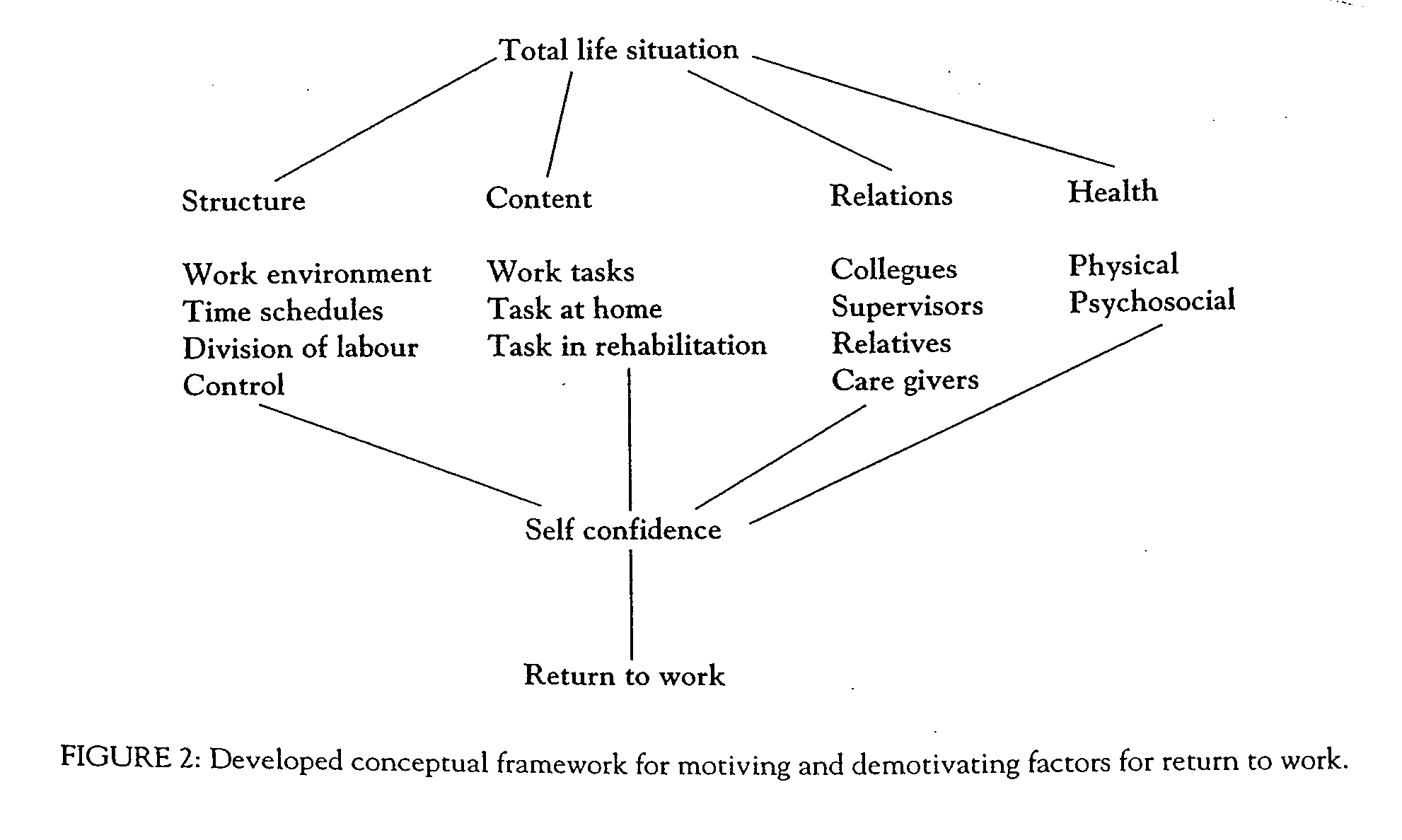
5.19 These findings are endorsed by other researchers
458 459, including a Swedish study
which developed the following conceptual framework:
460
5.20 A Norwegian study identified that high pain intensity, low self-assessed work
ability and a self-predicted absence status of longer than four weeks were good
predictors of being off work long term.
461
5.21 All 25 Canadian General practitioners surveyed by the Canadian Back Institute
believed that they could predict which back patients would not recover as
expected: they did this using instinct or gut feeling combined with a relationship
with the patient and knowing the circumstances surrounding his/her injury.
462 The
Institute developed its own checklist to determine the barriers to rehabilitation.
This is attached as Appendix Three.
5.22 Associated with the risk of remaining unemployed for the longer term is the need
to assess the readiness of an injured / disabled person to engage in job seeking.
Counsellors must process quantities of complex client information including
medical and psychological information plus education, employment and social
histories.
463 Many rely on their own clinical judgement to determine a client’s
readiness to seek employment, but they can have difficulty processing verbal and
non-verbal stimuli.
5.23 Research has shown that rehabilitation counsellors tend to favour negative client
factors (such as incapacities) over positive client factors, leading to a restriction of
access to employment opportunities. There are a variety of tools readily available
458 Hoogendoorn et al 2000 p 2122
459 Mills and Thornton 1998 p 594
460 Gard and Sandberg 1998 p 104
461 Reiso et al 2003 p 1472
462 McIntosh, Melles and Hall 1995 p 195
463 Mannock ,Levesque and Prochaska 2002 p 16
Page 105 of 144
link to page 107
to counsellors to assess the readiness (and willingness) of injured workers to return
to work so that the counsellor can address any barriers identified.
Modified work duties
5.24 Best practice includes employers having organisational return to work programmes
which are ready to be utilised as required. There are seven key components for
employers to consider:
1.
Identify lighter jobs and create job descriptions. Recognise that in some
situations lighter duties will be required for limited periods of time only;
2.
Where modified duty jobs are not readily apparent, consider new tasks or
ways of combining elements of existing jobs to create a modified duty job.
Small employers should explore with staff / union representatives what
voluntary agencies might be able to provide light duty jobs in partnership;
3.
Establish time limits for accommodating temporary restrictions – transitional
duty jobs should be transitional;
4.
Deal with any obstacles to having an effective return to work programme
including any cross – departmental issues or union concerns;
5.
Make sure modified duty jobs are safe, supervised and add value – they must
not be make-work;
6.
Identify any external assistance which may be available; and
7.
Communicate the company programme to every-one – employees at all levels,
union representatives. Make it part of the company culture.
464
Demand-side job development
5.25 The demand-side job development model is consistent with international trends
promoting the employment of people with disabilities, and is an excellent way of
focusing on outcomes rather than on process. Services are provided directly to
employers to help them meet their labour force needs by hiring people with
disabilities. The aim is to increase the number and range of positions that people
with disabilities can perform, and then to assist the employer in developing a pro-
active strategy to recruit people with disabilities.
5.26 Characteristics of demand-side job development include:
•
Identifying jobs which employers are having difficulty filling, evaluating the
essential components of the jobs, and assessing how tasks may be
restructured to enable jobs to be performed by people with disabilities;
•
A change of focus for rehabilitation professionals from “selling” clients to
becoming consultants to employers on organisational development,
workflow design and human resource development;
464 Kremer 2003 p 42-3
Page 106 of 144
link to page 108 link to page 108 link to page 108
•
Understanding employer needs in getting work done and matching
employer needs with client competencies;
•
Finding jobs and developing any job adaptations before finding the clients
to fill the jobs;
•
Maintaining on-going relationships between employers, vocational
professionals to provide continuing support to workers with disabilities, and
openings for career development;
•
Rehabilitation professionals provide top quality service to employers in
terms of job candidates, and providing training/ education and support to
supervisors; and
•
The goal of any job creation and placement is to improve the employer’s
financial position. Employers need to make enough profit to stay in
business.
465
Maintaining employment
5.27 Employment retention services are a key component of addressing the problems of
long term unemployed. As previously stated, the transition to steady employment
after a break is often difficult and stressful. Studies show that one quarter of
former welfare beneficiaries stop working within three months of placement, and at
least half are not working within a year.
466
5.28 Pre-employment programmes to help long term unemployed return to work need
to include job retention strategies. Such strategies should address any or all of:
•
Transportation issues;
•
Child / dependent care;
•
Health care;
•
Frequent follow-up in the first weeks of new employment and ongoing in-
work support;
•
Training in workplace norms such as punctuality, dress, communications,
behaviour;
•
Placement in good jobs as opposed to the first available job: better initial job
quality is linked with higher wages later on;
•
Financial assistance for low income workers;
•
Community resources available to support newly employed workers;
•
Handling crises and emergencies;
•
Instilling and supporting a will on the part if the programme participants to
persevere and achieve; and
•
Training in soft skills, entry-level job skills and life skills.
5.29 Programmes can successfully target clients for job retention.
467 One of the many
models is attached as Appendix Four. An important message is, however, that if
465 Gilbride and Stensrud 1992 pp 36-7
466 Relave 2000 p 2
467 Rangarajan, Schochet and Chu 1998
Page 107 of 144
link to page 109 link to page 109
people adapt programmes from overseas, they generate their own weights and cut-
off values using local data.
Business partnership
5.30 As American states and communities focus on welfare reform, attention was
increasingly focused on how the business community could be part of the effort.
Private companies were asked to participate in programmes to:
•
Prepare welfare recipients for work;
•
Train them in job skills;
•
Hire welfare recipients; and
•
Promote job retention once they are in work.
5.31 Best practice guidelines were developed, partly to help sell the concept of
partnership and then to ensure that partnerships worked, generally within the
context of other initiatives such as job search and training. Key challenges are:
•
Building business community interest in a partnership – businesses will
remain involved only if their own interests are advanced;
•
Making the partnership work, where the partners have very different
backgrounds and perspectives;
•
Remaining in touch with business needs, keeping attuned to labour market
conditions;
•
Promoting the employment of welfare recipients without stigmatizing them;
and
•
Maintaining a focus on the interests of the welfare recipients, while
achieving a balance between supply and demand of labour and the
competing interests between welfare reform and business.
468
5.32 First action is to identify appropriate potential business partners, such as those
with:
•
Urgent labour needs;
•
Possible job opportunities which match welfare recipients’ skills;
•
Large businesses which tend to have leaderships roles in the community;
•
Small businesses because they generally do not get involved;
•
Businesses with opportunities for workers to advance;
•
Businesses with government requirements to hire additional or
disadvantaged workers; and
•
Businesses already committed to helping their community.
469
468 Brown, Buck and Skinner 1998 p 14-15
469 ibid pp32-33
Page 108 of 144
link to page 110
5.33 Relationships need to be developed over time, building the vision, strategy and
goals together from the start. Goals and expectations must be clear at the start and
be realistic. Partnerships are about “win-win”: helping the welfare recipients and
strengthening businesses simultaneously. They need to be established on good
communications and trust, and then maintained constructively. This requires
strong leadership and dedicated staff.
470
5.34 The American Manpower Demonstration Research Corporation (MDRC) has
developed a series of How-to publications which promote best practice in
implementing welfare reform. Titles include:
•
Promoting participation: How to increase involvement in welfare to work
activities
•
Promoting partnership: How to involve employers in welfare reform
•
Beyond Work first: How to help hard to employ individuals get jobs and
succeed in the workforce
These are all available on the MDRC website <www.mdrc.org>
470 Brown, Buck and Skinner 1998 pp45-46
Page 109 of 144
link to page 111 link to page 111 link to page 111 link to page 111
Part 5: Recommendations for NZ
5.35 Before considering initiatives for implementation in New Zealand, it is important to
answer the question “ why go back to work?” Employment is described as a social
institution that meets many human needs:
•
It imposes a time structure on the working day;
•
It implies regularly shared experiences and contacts with people outside the
family;
•
It links an individual to goals and purposes that transcend their own;
•
It defines aspects of status and identity; and
•
It enforces activity.
471
5.36 Understanding how a job fulfils these needs helps explain why there is a motivation
to work beyond earning a living.
472 It also sheds light on the effects of job loss as
distinct from unemployment – this can be in terms of bereavement. Many countries
have not recognised the risks associated with job loss and have not implemented
comprehensive interventions that deal with the dual reality of loss of job and loss of
identity / family. The remedy for job loss is a new and satisfactory job – not “any
job”.
473
Human Capability Framework
5.37 The New Zealand Department of Labour developed the Human Capability
framework as a way of providing an integrated view of key economic and social
objectives, and of understanding the role of the labour market in achieving them.
It is designed to provide a better understanding of the influences, linkages and
levers that impact on human capability.
474
5.38 The framework brings together a number of elements which affect New Zealand’s
human capability:
•
Key factors that influence people’s capacity (their skills, knowledge and
abilities) and the diverse ways of building capacity;
•
Key factors that influence the creation of opportunities for that capacity to
be used in ways that give people financial or personal rewards; and
•
The ways in which capacity and opportunity get matched, and the risks for
people and businesses if capacity is damaged or capacities and opportunities
do not correspond.
5.39 The following diagram shows the variety of influences on human capacity in both
economic and social spheres:
471 Jahoda 1979 p 494
472 Tu 2000 p 57
473 ibid p 67
474 Department of Labour 1999 Overview
Page 110 of 144
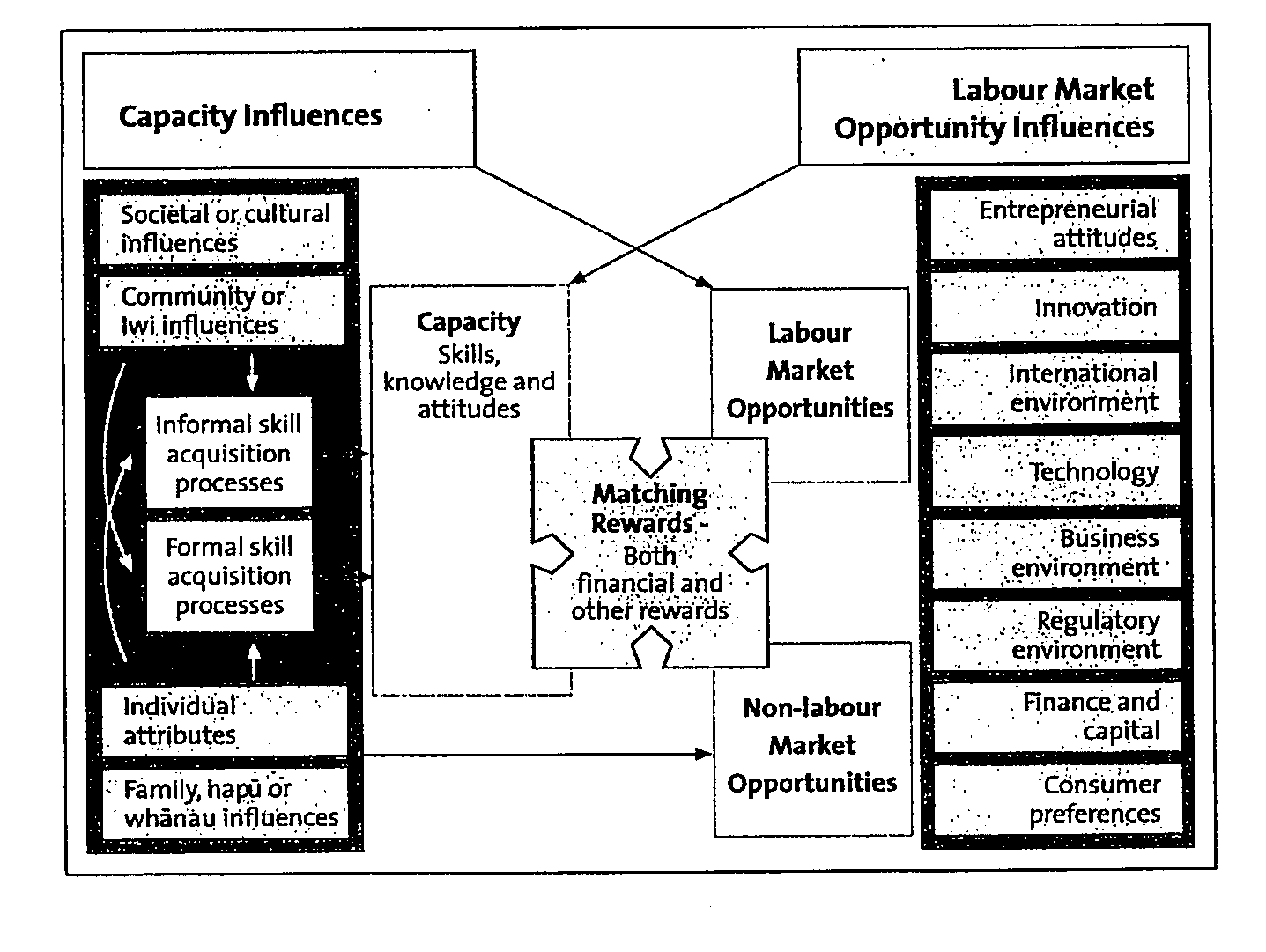
5.40 Current trends affecting human capability include:
•
An ageing workforce;
•
Increasing proportions of Maori, pacific island and other ethnic groups,
often in population concentrations;
•
Significant numbers of new entrants to the workforce have low educational
attainments;
•
Increasing globalisation of the New Zealand economy;
•
Constant technological change;
•
Changing skills levels required by industry, with a move from low skilled
manual labour to low skilled service sector; and
•
Job growth in the high skilled market, and job losses in the low skilled
market
5.41 Key policy issues identified by the department are to address the following needs:
•
A flexible workforce, able to adapt to changing skill needs and prepared for
lifelong learning;
•
Innovative business development which is able to make best use of new
global opportunities and new technologies;
•
Improved workforce capacity, including educational achievement amongst
maori and minority ethnic groups; and
Page 111 of 144
link to page 113 link to page 113 link to page 113
•
Innovative regional solutions to address the impact of agricultural and
manufacturing downturns, the continuing population drift northwards and
concentrations of low capacity levels within some communities.
5.42 The commitment by the Department of Labour to use the framework in its work
means that ACC’s practices should be consistent with the framework.
The current New Zealand labour market
5.43 According to the Department of Labour
475, the labour market of New Zealand is one
of the cyclically strongest in the world at present
. The unemployment rate has been
trending down since 1999 thanks to robust job growth and is now at 4.4 percent,
the lowest since December 1987 and one of the lowest in the OECD. Encouraged
by this, a high number of people are participating in the labour market as the
participation rate rebounded to a high 66.6 percent. Approximately 30,000 new
jobs are created each year.
5.44 The outlook is for a weakening in the New Zealand economy over the next year
due to a sharp fall in export returns, caused by the rise in the New Zealand dollar
and the staggering world economy. A weakening in economic growth is expected to
lead to a worsening of labour market conditions in 2003/04, with lower
employment growth and a moderate rise in unemployment.
5.45 Recent years have seen strong growth in knowledge intensive services, including
education, health and community services and property and business services.
Leisure and entertainment industries have also grown faster than average. The
occupational mix of employment within industries is also changing, with a shift
towards white collar work. Manual work is declining while numbers of managers,
professionals and technicians are increasing. Clerical work is declining, reflecting
the impact of information technology.
5.46 The Department’s Future of Work team notes that some groups of workers have
suffered a drop in job tenure, but long term employment relationships remain
strong. Non-standard employment (such as part-time, casual, temporary and self-
employment) is on the rise.
476 The increase in part-time and self-employment is
partly driven by people’s need for flexibility, but the increase in temporary and
casual work is likely to lead to more job insecurity, low pay and poor working
conditions for these workers.
5.47 The number of older workers is expected to increase by a third between 2002 and
2011. The Department of Labour warns that employers may have to create new
employment patterns to retain older workers. Making maximum use of the
available workforce will require breaking down the negative stereotypes that
surround age.
477
5.48 The increase in the ageing population means that retraining is likely to be required
to keep up with changing skill demands. Fewer young people entering the
workforce means that employers will need to be more flexible in order to retain
475 Department of Labour website <www.dol.govt.nz>
476 The proportion of people who work the standard 40 hour week stands at just 30%.
477 Department of Lbaour pp16-17
Page 112 of 144
link to page 114 link to page 114
older workers. Migration will continue to have a major impact on the labour
market, both inwards and outwards migration. An increasing portion of the labour
force will be migrants from non-English speaking countries.
5.49 Higher levels of skills are increasingly required, especially in communications,
literacy, numeracy and problem solving. Flatter management structures means
that workers are progressively required to display judgement, leadership and
initiative along with motivation and attitude.
5.50 This is all best summarised : “Change is the norm. The best way of coping with the
changing face of work is to take charge of your own destiny”
478 The challenge for
ACC is to implement it.
Helping long term claimants
5.51 Recent research on the needs of long term ACC claimants in return to
independence identified five stages in the transition to independence / work:
1.
Pre-contemplation: not thinking abut returning to independence / work;
2.
Contemplation: thinking about returning to independence / work;
3.
Preparation: preparing to return to independence / work;
4.
Action: entering work or transitioning from part-time to full-time work;
5.
Maintenance: remaining independent from ACC / remaining in work.
479
5.52 The time taken to transition along the continuum varies from claimant to claimant,
and some claimants move backwards in reaction to negative events (such as job
rejections from employers).
Helping newly injured
5.53 This literature search has acknowledged that being pro-active when workers are
first injured is most effective. Various potential initiatives are identified for
claimants, for employers, for case managers and for medical professionals.
5.54 Initiatives which would assist new claimants cope with their changed
circumstances include:
•
Money management training to enable new claimants to budget and live
within their reduced level of income;
•
Meeting / discussion groups with other claimants with the same / similar
type of injury, albeit at different stages in their rehabilitation;
•
Programmes for the newly injured, similar to the Spinal Injury Trust pilot
operational in Christchurch; and
•
Managing the trauma of the injury and the grieving process of the accident.
478 Department of Labour 2003 p 6
479 Litmus 2003 Conclusions
Page 113 of 144
link to page 115 link to page 115
5.55 The proven benefits of early return to work for many types of injuries need to be
explained to many of the medical profession, in particular to the patient’s General
Practitioner. These include:
•
Better self image;
•
Improved ability to cope;
•
Improved work survivability; and
•
Improved ability to be independent.
480
5.56 There is both empirical and anecdotal evidence that many GPs respond
unconstructively to pessimistic attitudes from injured workers, by focusing on the
negative issues rather than on what the patient can achieve. They extend time off
work which allows patients more free time to dwell on the negative, rather than
assisting patients keep their minds active and focused on more positive matters.
5.57 This has been described as “the physician treating the whole patient”,
acknowledging both medical and biosocial issues. Physicians cannot prove or
disprove the existence of pain clinically, but they can address the problem that
prolonged time away from work makes recovery progressively less likely.
481
5.58 There is no question that to return to work after a long absence may require some
effort on the part of the worker to face their fears or unwillingness about returning
to work. Many people with disabilities describe days when their symptoms are
sufficiently severe that they have to force themselves to get up and go to work
despite their pain. The benefit is that once at work, their daily tasks and duties
serve to distract them from their pain. If GPs can work with their patients, helping
them recognise the benefits of being at work and developing pain management
techniques, many will be rehabilitated more quickly.
Case management
5.59 As case managers play a key role in the rehabilitation of claimants, it is relevant to
list some of the effective practices identified in the course of this research. These
include:
•
Training case managers in how to interview for “client strengths”;
•
Including the goals of vocational rehabilitation right at the start of the
claimant / case manager relationship, rather than focusing initially only on
managing the injury and grief, and ensuring that the claimant both
understands this and commits to it;
•
Setting goals at the start and maintaining the focus on them;
•
Ensuring goals are realistic ones which can be achieved step by step;
•
Focusing on (the many things) the claimant can do rather than (the few)
they cannot do;
•
Understanding how people respond to negative / positive attitudes in the
same way, and learning to manage claimants’ pessimism;
480 Melhorn pp69-70
481 Melhorn p70
Page 114 of 144
link to page 116
•
Overcoming concepts of ageism (“they’re close to retirement so no need to
get back to work”);
•
Acknowledging and rewarding claimant achievements in rehabilitation in a
small but positive way;
•
Learning how to recognise literacy problems in claimants and managing this
as a barrier to return to work;
•
Exploring the work-place culture of the claimant’s pre-injury employment as
part of their return to work. This may result in the claimant being referred
to another employer, or in providing assistance / support to the claimant’s
colleagues and managers;
•
Recognising the impact of changes in the labour market mean that many low
skilled or manual workers may require new skills in order to return to work.
This is re-skilling and not to be confused with the concept of up-skilling;
and
•
Mapping transportation with claimants, whether for work or for family
matters such as childcare.
Policy development
5.60 The OECD has provided some useful guidelines on developing policy to help
people with disabilities obtain and retain employment.
482 These are:
•
Recognise the status of disability independent of the work and income
situation. Disabled does not equate with unable to work;
•
Introduce a culture of mutual obligations: it is not just society’s
responsibility but disabled people and employers as well;
•
Design individual work/benefit packages comprising
•
Rehabilitation and vocational training
•
Job search support
•
Financial assistance
•
The potential of different forms of employment such as part-time, subsidised
etc
•
Activities to assist the social integration of people with disabilities
•
Introduce new obligations for disabled people, such as participation in
vocational rehabilitation, employment and other integration measures;
•
Involve employers in the policy process. Different approaches to encourage
employment of people with disabilities range from moral suasion to anti-
discrimination legislation and compulsory employment quotas. Thee
effectiveness of these measures depends on the co-operation of employers;
•
Promote early intervention
•
Make financial assistance a flexible policy element, to take account of
whether the person has been able to gain a job, changes in the person’s
disability status over time, and not to penalise a person unfairly for taking
up employment;
482 OECD 2003
Page 115 of 144
•
Reform programme administration. Promote equal access to all programmes
for all people. Caseworkers will need an extensive knowledge of the range of
benefits and services available, and have time to assist individuals and follow
each case; and
•
Design disability programmes as active programmes, not early retirement or
quasi-permanent exits from the labour market.
Page 116 of 144
link to page 118
APPENDICES
APPENDIX ONE: How to relate to people with disabilities
These Guidelines were developed by the American Psychological Association.483
Many of the barriers which people with disabilities face are reinforced by small details of
language and behaviour. These details may seem insignificant, but they often reaffirm
inaccurate assumptions and cause offense. By changing how you portray and communicate with
people with disabilities, and by modifying a few features of your environment, you, as human
service providers, educators, and the media, are in a unique position to shape public attitudes
about people with disabilities in a helpful way.
1 PORTRAYAL ISSUES
Language influences perceptions and behaviour. Words in popular use mirror prevailing
attitudes in society. Oftentimes, societal attitudes create barriers for people with
disabilities. Through language usage, we can conjure up images of people actively engaged
in life, and we can avoid stereotypical phrases that suggest helplessness or tragedy.
Person First Language
When you refer to a "disabled woman," your listener or reader has already begun to form
some kind of image of "disabled" before she/he hears the word "woman." The subject of
the sentence then hasn't a chance to be thought of as a regular person. She will be
considered mainly disabled and secondarily a woman until or unless your subsequent
language jars this image loose.
On the other hand, if you refer to her as a "woman with a disability" the reverse tends to
occur. Your audience first starts forming an image of an ordinary woman, and then
modifies it. The focus becomes on the individual, not the particular functional limitation.
Once you've identified her as having a disability, and the most adaptive image you can
conjure up for her is pretty much set in your reader or listener's mind, there is no reason
not to use the briefer expression "disabled woman" from time to time if you feel the need
for literary variety.
Sensationalizing
One common way of sensationalizing disability is to describe highly successful people with
disabilities as "superhuman." Such individuals are shown as being "incredible" or
"extraordinary" because they strive to overcome their limitations and serve as role models
or yardsticks for measuring personal achievement. While people with disabilities have had
to overcome obstacles dealing with their disability, they generally have the same range of
talents and dispositions as non-disabled individuals. Portraying persons with disabilities as
"superstars" creates unfair expectations.
483 From website http://www.apa.org/pi/cdip/enhancing.html
Page 117 of 144
Another common way of sensationalising is to use the language of tragedy or catastrophe.
Words and phrases like "afflicted with," "struck by," "a victim of," or "crippled with"
disability generate sentimental feelings of pity, which can be socially damaging to the
person described. It also leaves the reader or listener with the nebulous impression that
individuals with disabilities face serious problems with which they cannot cope.
Focus
If you get stuck on a person's disability, your listener or reader will get stuck there too.
Usually, other aspects of the person are more interesting or relevant to the issue at hand.
This is equally true regarding race, ethnicity, sex, and sexual orientation. If such
demographics seem worth mentioning, then mention them. This can be done without
making them the focus of the described individual's being.
Being, Having, Doing
It is generally useful to avoid verbs that imply that disability encapsulates all there is to say
about a person. Also, it is useful to avoid verbs that suggest images of passivity. For
example, the phrase "so-and-so is in a wheelchair" conjures a passive image, someone just
sitting there doing nothing. By contrast, the phrase "so-and-so uses a wheelchair" tends to
elicit an action image, someone wheeling a chair or operating a control device. The first
person seems helpless and detached; the second, participatory and involved.
Most people who have been hospitalized even briefly understand how disconcerting it is to
be known temporarily as "the heart in room 18" or "the liver in room 24." It doesn't take
much imagination to understand how annoying it would be to hear yourself referred to as
a "spinal cord injury" or a "manic depressive" for the rest of your life. It's no harder to say,
"Charlie has a spinal cord injury" or "manic-depressive illness" than it is to say, "Charlie is
a spinal cord injury" or "manic depressive." The first suggests that disability is just one
trait among many. The second implies that it summarises the essence of all that Charlie is.
In summary, in the most wholesome, socially appealing image, the person is doing
something. In the second best, one is seen as a person who has a disability. In the least
helpful social image, one's very being is identified by disability--other facets of personality
disappear, leaving only embodied disablement.
Disability-Disease Distinction
Some disabilities are progressive results of chronic conditions, but many, probably most,
are not. The illness/injury that caused the disability is an event of the past. A person with a
substantial disability may be healthier than you are. This distinction can be very important
in such situations as a job search, acquiring health insurance, and getting a date. A person
with a severe disability doesn't need the unwarranted obstacle of being seen as also having
an active disease.
Injury-caused disabilities are easy to distinguish from disease-caused disabilities once you
know they result from injuries. Disease-caused disabilities pose more problems because
most people don't know which diagnostic labels reflect acute illnesses that are long past
and which designate continuing illnesses. To err on the safe side, assume "stable disability,
no disease" unless the person corrects you.
Euphemisms
Euphemisms claimed as politically correct by various splinter groups (e.g., "impaired,"
"physically challenged," and "differently abled") have generated endless jokes and
parodies, which may not be what their promoters wanted. Suffice it to say, these are fad
phrases that have not gained general acceptance among people with disabilities.
Page 118 of 144
Of the main non-euphemistic terms, "disability" has come to be preferred over "handicap"
as the more general descriptor. This is owing to the latter's narrower meaning as well as its
historical association with fundraising pathos. The word "disability" refers to the
functional limitation a person experiences as a result of an impairment. The word
"handicap" refers to the social consequences of the disability. For example, stairs, narrow
doorways, and curbs are handicaps to people with disabilities who use wheelchairs.
2 COMMUNICATION ISSUES
Many people feel uncomfortable around individuals with disabilities. Much of this
discomfort stems from lack of personal contact with people with disabilities and a sense of
awkwardness and uncertainty as to how to speak and act in their presence.
The following section offers suggestions for increasing effective communication and
reducing anxiety when interacting with people with specific disabilities.
Hearing Impairments
• Do not make assumptions about a person's ability to communicate or the way in
which they do it. Always ascertain which communication medium the deaf or
partially hearing person intends to use.
• When interacting with people who prefer lip reading, use a well-lit, glare-free area.
• Face the person directly and continue speaking at a normal volume and rate.
• Rephrase sentences rather than repeat them.
• Do not cover your mouth or look away from the person, such as to take notes,
while you are talking.
• Communicate in writing, if necessary.
• When a sign language interpreter is present, it is best to face the person and speak
normally.
• Omit phrases such as "please tell him/her that..." and address the person directly
while the interpreter signs.
Visual Impairments
• Ask if any particular assistance is needed.
• Orient the person to the area, explaining where major furniture is located. If the
person has been there before, you should inform him/her of any changes or new
obstacles.
• Keep doors fully open or closed to prevent accidents.
• Offer to read written information for a person with a visual impairment, when
appropriate.
Page 119 of 144
• If you are guiding someone, let him/her take your arm just above the elbow, and
guide rather than lead or propel the person. Give him/her clear instructions such as
'this is a step up' as opposed to 'this is a step.'
• When giving directions, use specific words such as "straight ahead" or "forward."
Refer to positions in terms of clock hands: "The chair is at your 2:00." Avoid vague
terms such as "over there."
• Don't assume the person will recognise you by your voice even though you have
met before. Identify yourself by name, maintain normal voice volume, speak
directly to the person, and maintain eye contact.
Speech Impairments
• Listen patiently and avoid completing sentences for the person unless she/he looks
to you for help.
• Don't pretend to understand what a person with a speech disability says just to be
polite.
• Ask the person to write down a word if you're not sure what she/he is saying.
Mobility Impairments
• Ask if assistance is required.
• Do not remove a person's mobility aid, for example crutches, without the person's
consent.
• When talking to someone who is in a wheelchair and the conversation continues
for more than a few minutes, sit down or kneel to be eye level. This avoids neck
strain and is much more positive.
his/her
• Don't lean on a person's wheelchair unless you have his/her permission--it's his/her
personal space.
3 COMPLIANCE ISSUES
As service providers and advocates, psychologists and other mental health providers need
to ensure that their services adequately meet legal and ethical obligations.
To improve compliance with the Americans With Disabilities Act and to better meet the
needs of individuals with disabilities:
• Do not deny your services to a client with a disability. You may refer him/her if that
individual requires treatment outside of your area of specialization.
• Do not separate out or give unequal service to clients with disabilities unless you
must do so to provide a service that is as effective as that provided to those without
disabilities.
Page 120 of 144
• Watch for criteria that screen out clients with disabilities. For instance, do not
require a driver's license for payment by check. Use policies, practices, and
procedures in your office that can be modified for those with disabilities, such as
making sure service animals are permitted in your office.
• You may need to provide auxiliary aids and services, such as readers, sign-language
interpreters, Braille materials, large-print materials, videotapes and audiotapes, and
computers when necessary to effectively communicate with your clients with
disabilities. You may use alternative forms of communication, such as notepads and
pencils, when these forms are as effective.
• Evaluate your office for structural and architectural barriers that prevent
individuals with disabilities from getting the services they need from you. Change
these barriers when they can be readily changed (without much difficulty or
expense). Look at ramps, parking spaces, curb cuts, shelving, elevator control
buttons, width of doorways, levered door handles, width of toilet partitions, height
of toilet seats, high-pile carpeting, and ensure that rooms are large enough to
manoeuver a walker or wheelchair.
• When building new offices or remodeling, hire an architect or contractor familiar
with ADA requirements.
Copyright (c) 1999 by the American Psychological Association. This material may be reproduced in whole or in part
without fees or permission, provided that acknowledgement is made to.
Page 121 of 144
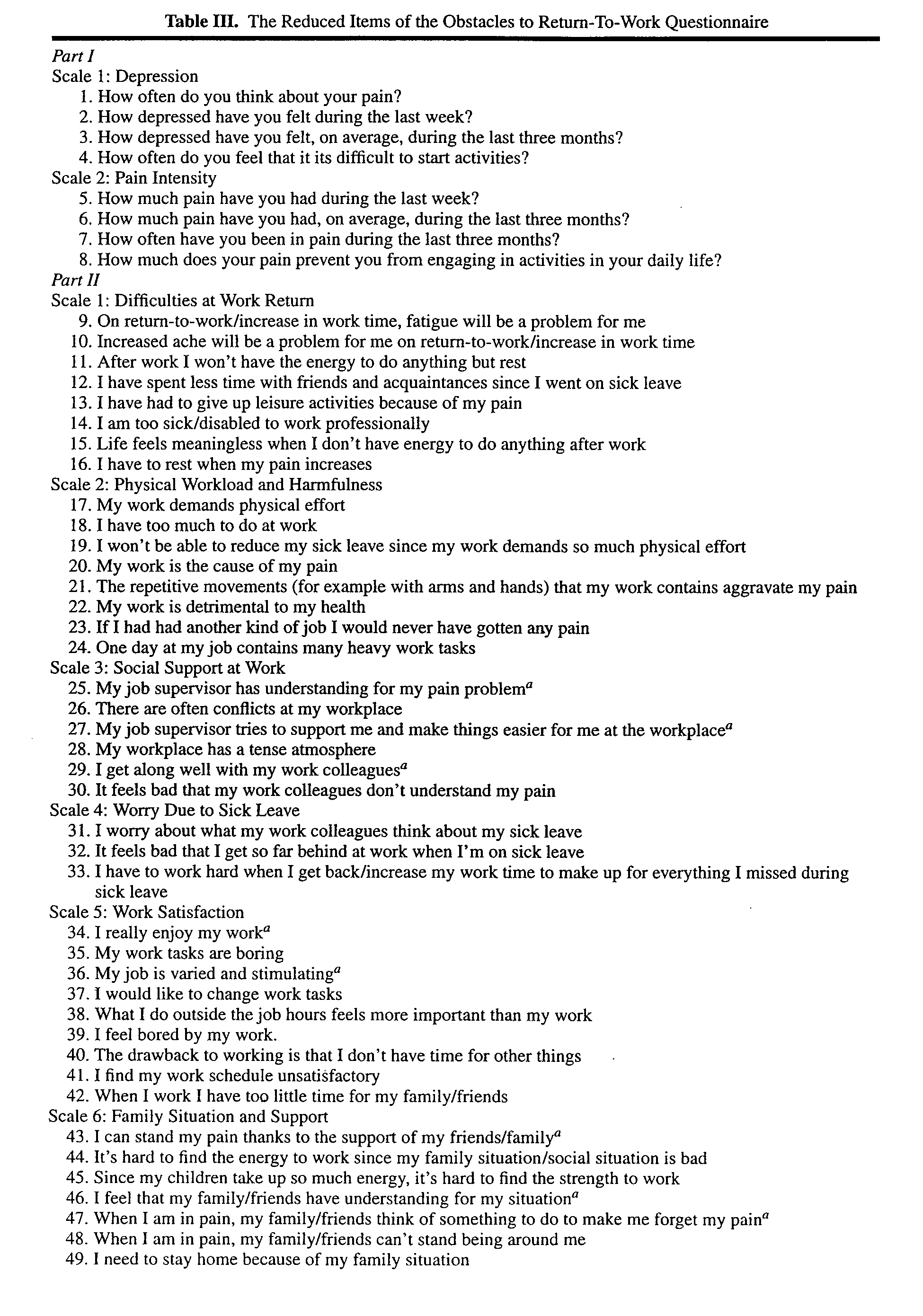 APPENDIX TWO: Obstacles to return to work Questionnaire
Page 122 of 144
APPENDIX TWO: Obstacles to return to work Questionnaire
Page 122 of 144
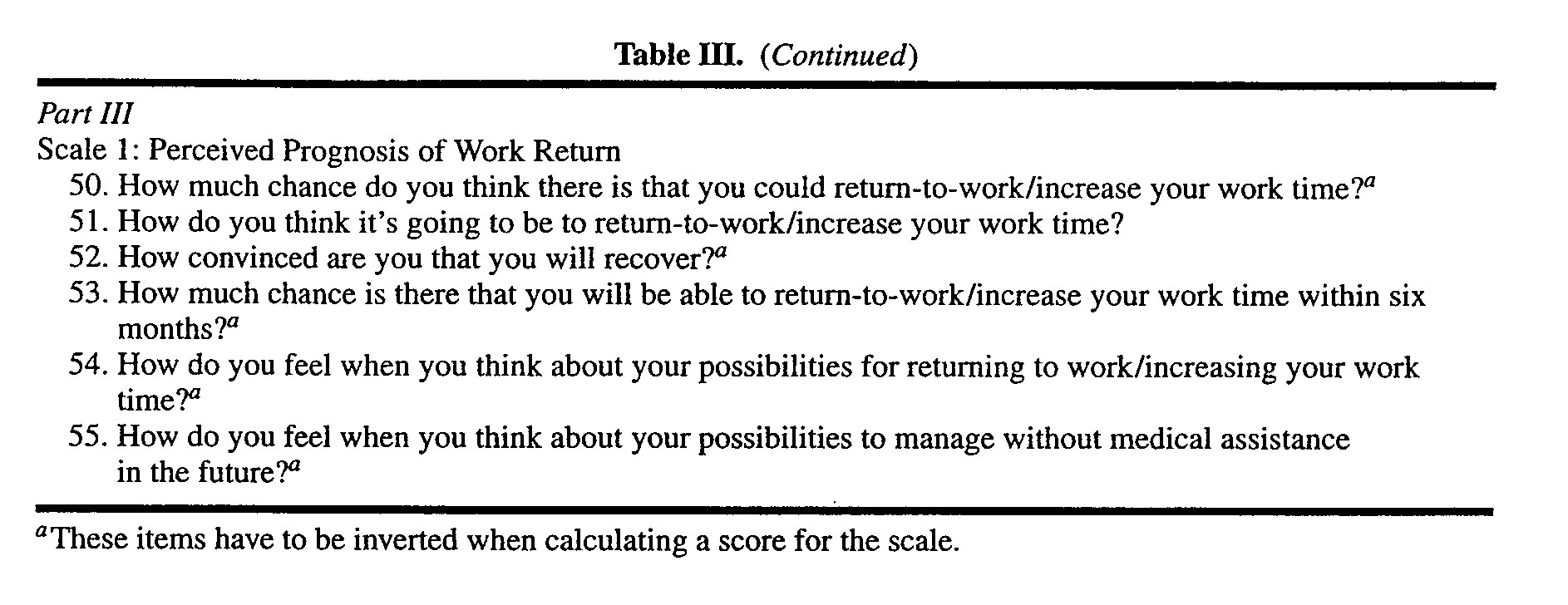 Page 123 of 144
Page 123 of 144
link to page 125 link to page 125
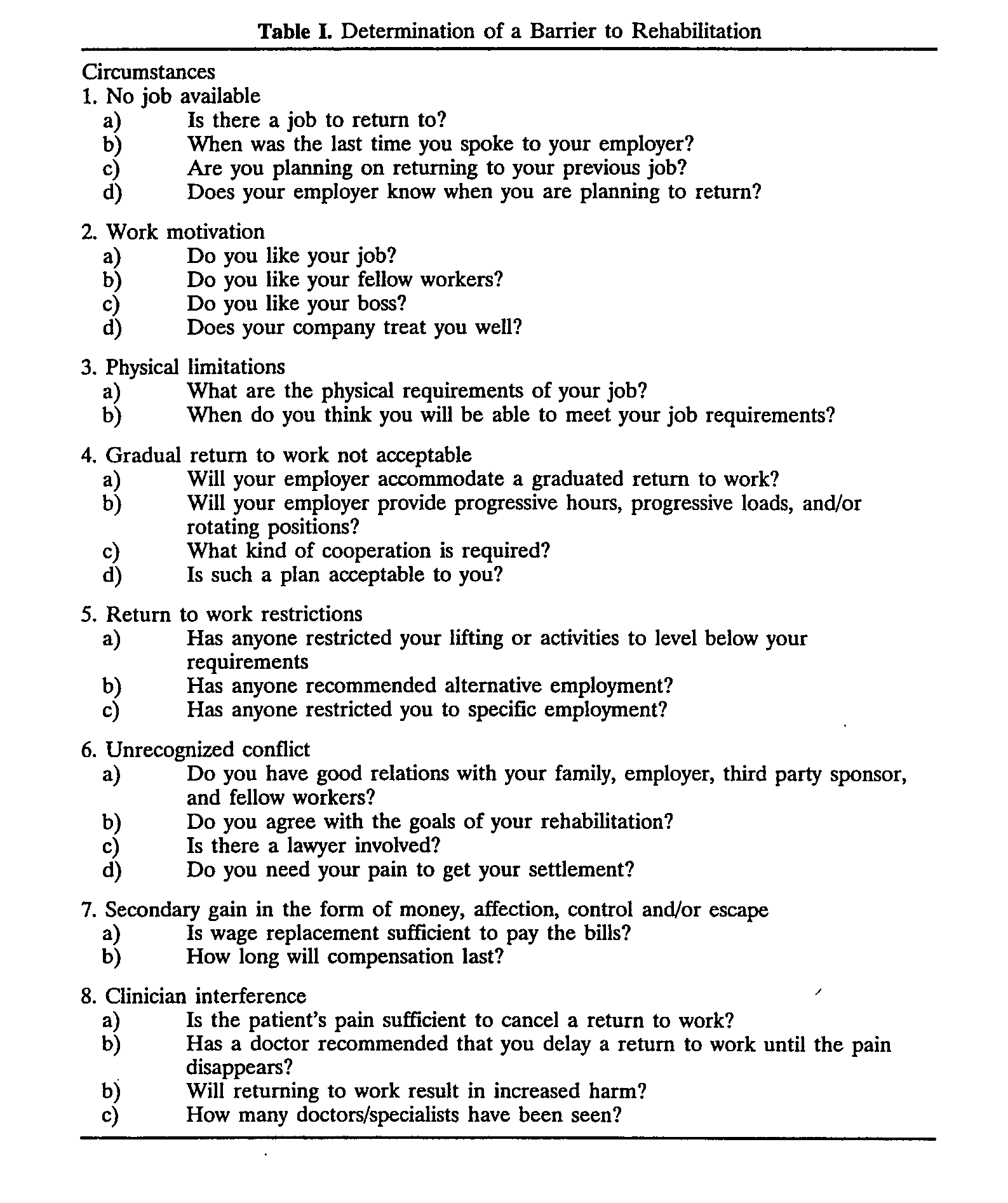 APPENDIX THREE: Identifying barriers to rehabilitation 484
APPENDIX FOUR: Identifying people needing assistance with job retention 485
APPENDIX THREE: Identifying barriers to rehabilitation 484
APPENDIX FOUR: Identifying people needing assistance with job retention 485
484 McIntosh, Melles and Hall 1995 p 195
485 Rangarajan, Schochet and Chu 1998
Page 124 of 144
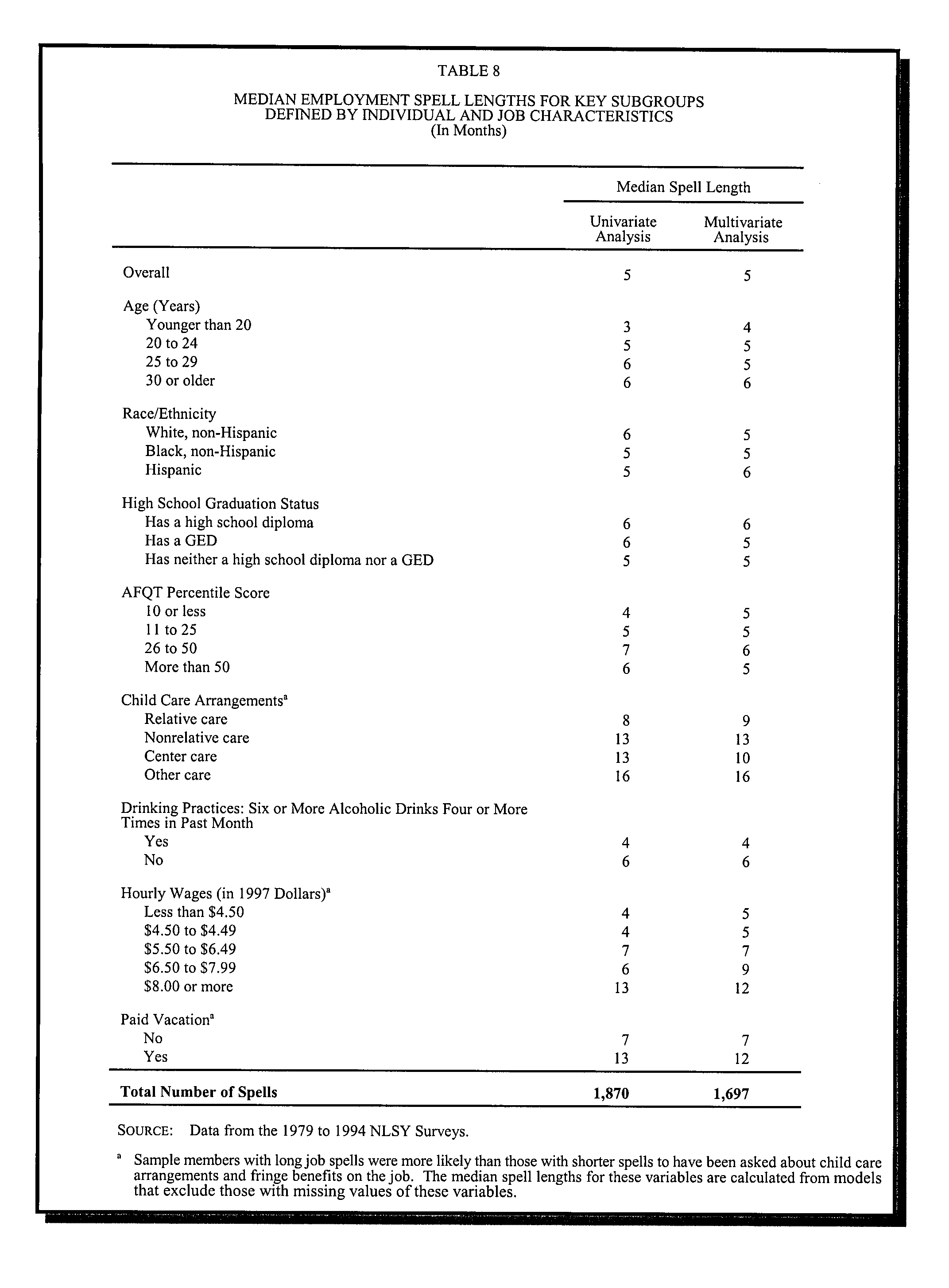
APPENDIX FOUR: Model For Predicting People Requiring Assistance To Return
Employment
Page 125 of 144
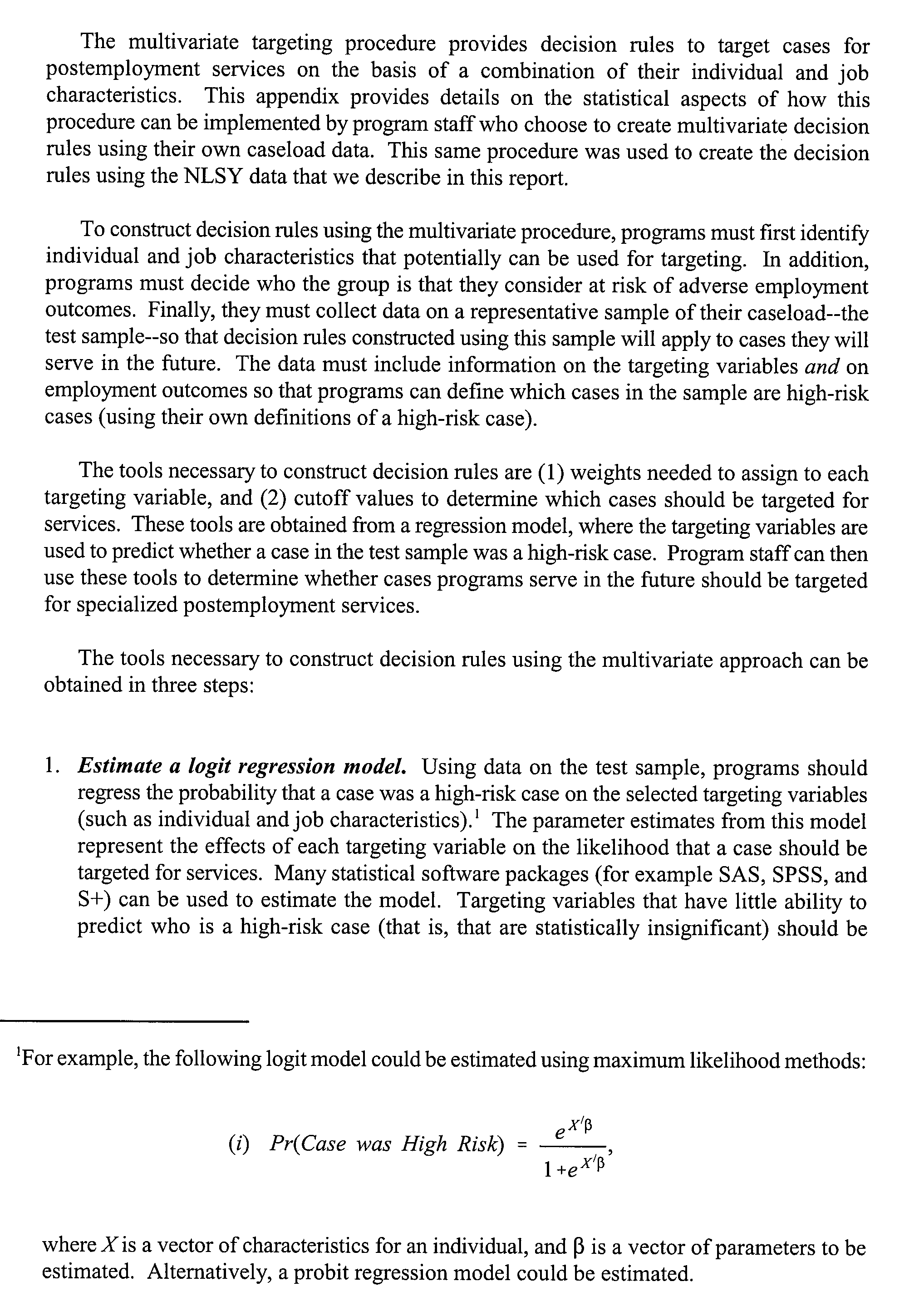 Page 126 of 144
Page 126 of 144
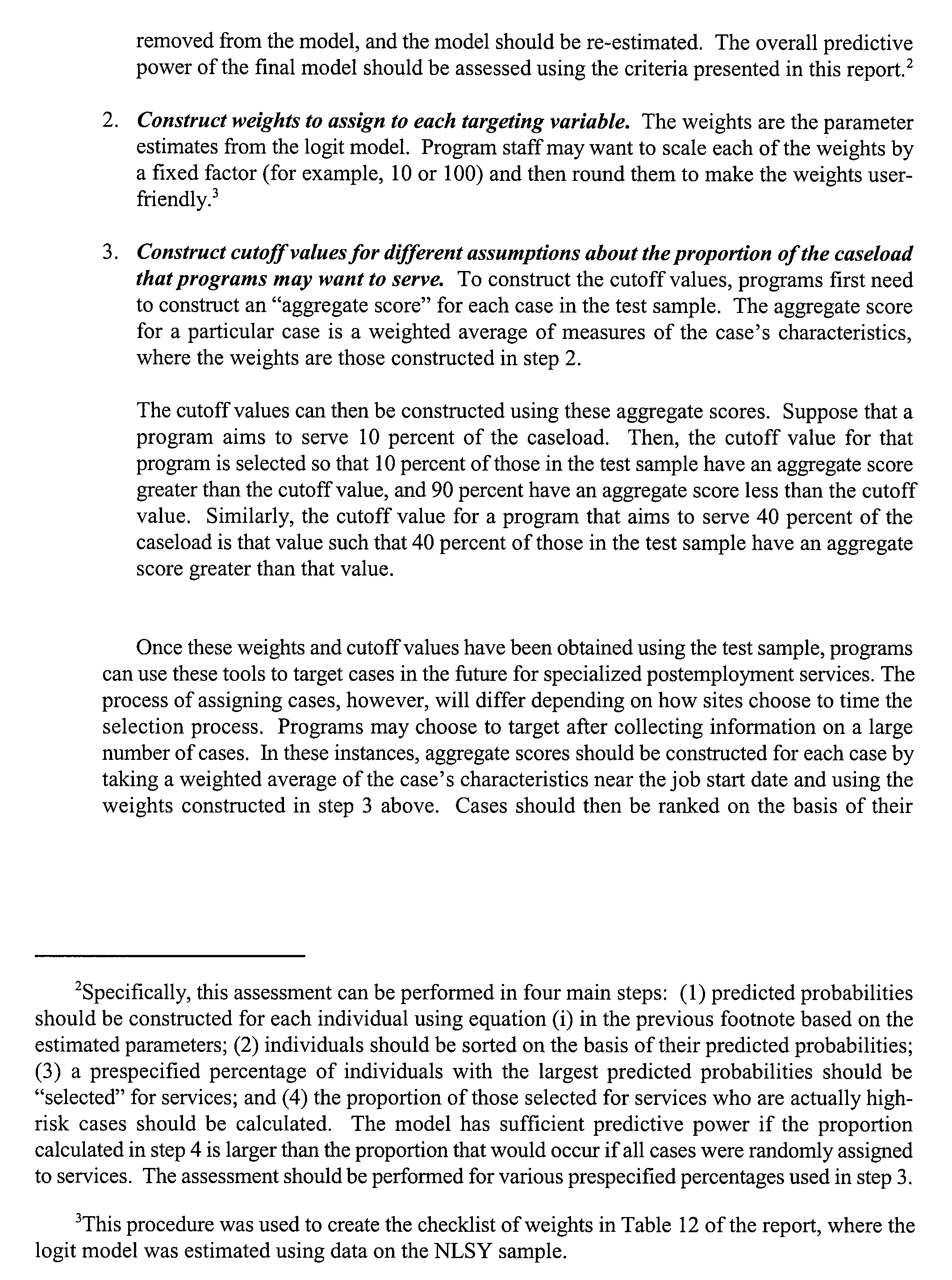 Page 127 of 144
Page 127 of 144
 Page 128 of 144
Page 128 of 144
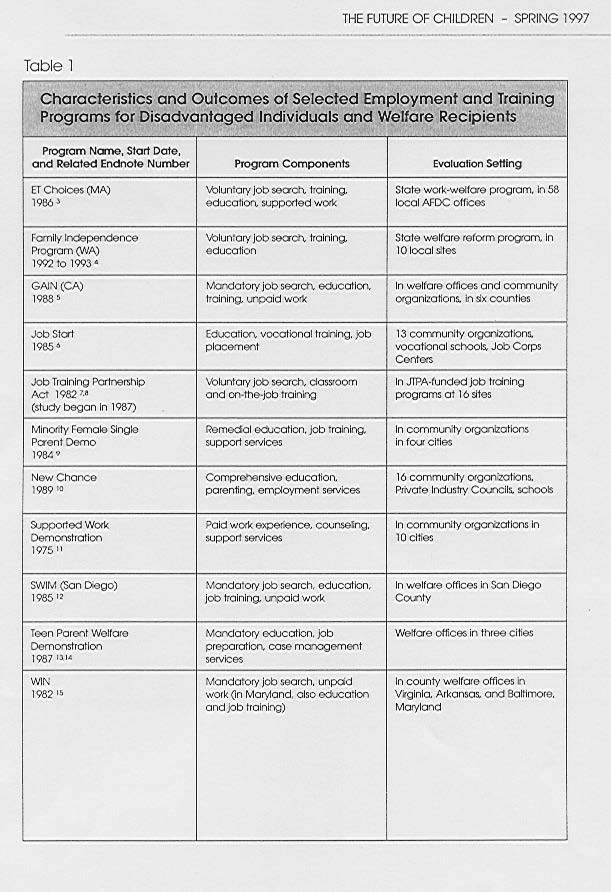 APPENDIX FIVE: Evaluation of selected employment and training programmes
APPENDIX FIVE: Evaluation of selected employment and training programmes
From Nightingale and Holcomb 1997
Page 129 of 144
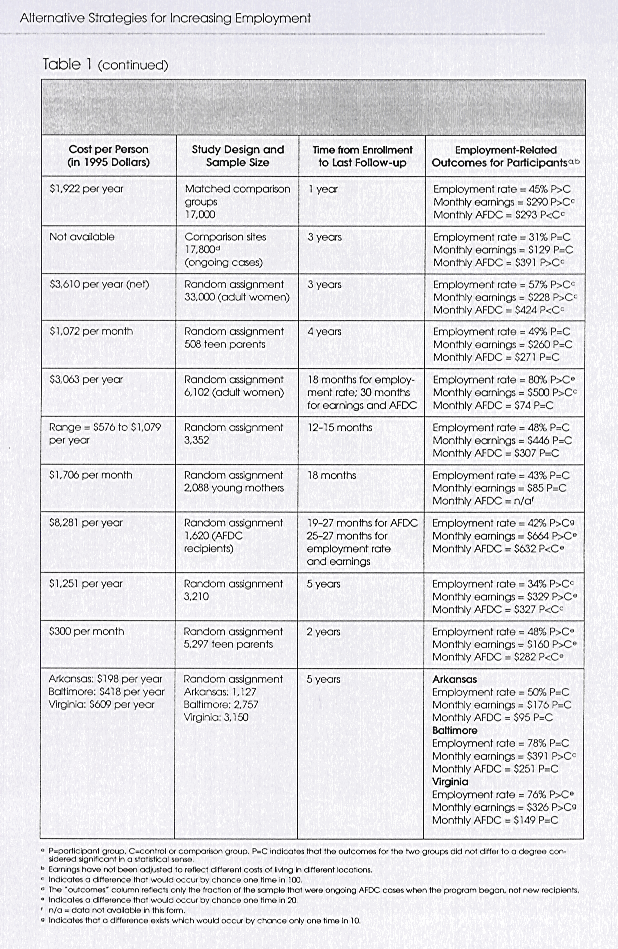 Page 130 of 144
Page 130 of 144
Bibliography
Author
Title
Aarts, Leo J M & De Jong, Philip R
Economic Aspects of Disability Behaviour
ACC 2003
Fourth Quarterly Maori Report 2002/3
ACC Staff Intranet: Informe
Employment Maintenance Programme
American Association of Retired Persons
How to Recruit Older Workers. 1993
Anderson, Jane & Bricout, John C & West, Michael
Telecommuting: meeting the needs of businesses and
D
employees with disabilities. 2001
Annable, Gary
Disabilities in Manitoba. 2000
Arthur, Sue, & Corden, Anne & Green, Anne &
New Deal for Disabled People: Early
Lewis, Jane & Loumidis, Julia & Sainsbury, Roy
Implementation Department of Work and
& Stafford, Bruce & Thornton, Patricia &
Pensions research Report No 106
Walker, Robert. Department for Work and
Pensions
Ashworth, Karl & Hartfree, Yvette & Stephenson,
Augusta (2001)
Well Enough to Work? Department of Work
and Pensions research Report No 145
Ashworth, Karl & Youngs, Rachel.
Prospects of Part-time Work: The Impact of the
Back to Work Bonus. Department for Work and
Pensions Research Report No 115
Atkinson, L; Giles, L and Meager N
Employers, Recruitment and the unemployed,
Institute for Employment Studies Report no
325
Australian Commonwealth, Return to Work
Review of International and Jurisdictional Best
Advisory Group
Practice in Return to Work
Baines Colin (2003)
Disability, the Organisation of Work, and the need
for change. OECD
Baldwin, Marjorie L & Johnson, William G
Dispelling the Myths about Work Disability: in
New Approaches to Disability in the Workplace
1998
Bivand P (1999)
Tough-love on the dole. Working brief no 107,
Department of Work and Pensions, UK
Blackwell, Terry L & Leierer, Stephen J & Haupt,
Predictors of Vocational Rehabilitation Return-to-
Stephanie & Kampitsis, Angeliki
Work Outcomes in Workers’ Compensation.
2003
Borooah, Vani K
Why do Unemployed Men Ireland Find it Hard to
get Jobs?. 2000
Borooah, Vani K
Globalisation, Barriers to Employment and Social
Exclusion. September 2001
Boylan, Ann & Burchardt, Tania
Barriers to self-employment for disabled people.
Page 131 of 144
January 2003
BRC Marketing and Social Research (2003)
Return to sustainable earnings, Final report
Brantner CL (1992)
Job coaching for persons with traumatic brain
injured employed in professional and technical
occupations in Journal of Applied
Rehabilitation Counsel 1992 Vol 23
British Medical journal, 1996
Welfare Claimants are Less Healthy than Workers.
British Medical journal, Vol 313 p 646
Brown, Amy (2001)
Beyond work first: how to help hard-to-employ
individuals get jobs and succeed in the
workforce, published by the Manpower
demonstration Research Corporation
Bryan, Helena
Previously injured workers add value to workplace.
June 2003
Bunch, Mary & Crawford, Cameron (1998)
Persons with Disabilities: literature of the factors
affecting employment and labour market
traditions published Human Resources
Development Canada
Burchardt Tania (2001)
Moving in, staying in, falling out: employment
transitions of disabled people, BHPS Conference
2001
Butler, Richard J., William G Johnson, Marjorie L
Managing Work Disability: Why First Return to
Baldwin.
Work Is Not a Measure of Success, in Industrial
and Labour Relations Review 48 (April 1995)
.
Canadian Injured Workers Alliance, 1995
Voc Rehab & Re-employment from the Injured
Worker’s Perspective: Analysis of Survey Findings.
Caplan, Robert D & Vinokur, Amiram D & Price,
From Job Loss to Reemployment Field Experiments
Richard H (1997)
in Prevention – Focused Coping. In Primary
Prevention Works, eds GW Albee and TP
Gullotta. Sage Publications
Caplan, Robert D & Vinokur, Amiram D & Price,
Job Seeking, Re-employment, and Mental Health: A
Richard H & van Ryn, Michelle
Randomized Field Experiment in Coping with
Job Loss. 1989
Casey, Bernard; Metcalf, Hilary; Metcalf, Hilary and
Employers use of flexible labour published by
Millward Neil (1997)
Central Books
Cater, Bruce I (2000)
Employment, Wage, and Accommodation Patterns
of Permanently Impaired Workers in Journal of
Labor Economics Vol 18 No 1
Centre for Research on Women with Disabilities
Personal Assistance: Its effect on the Long-term
Health of a Rehabilitation Hospital Population
Chapin MH and Kewman DC (2001)
Factors affecting employment following spinal cord
injury: a qualitative study in Rehabilitation
Psychology Vol 46 no 4
Cole, Donald C; Mondloch Michael V; and Hogg-
Listening to injured workers: how recovery
Johnson, Sheilah
expectations predict outcomes In Canadian
medical Association Journal Vol 166 no 6
Corden, A & Thornton, P (2001)
Employment programmes for disabled people: An
international research review. Department for
Page 132 of 144
Work and Pensions In-house Report no 90
Corden, A & Thornton, P (2003)
Results-based funded supported employment:
avoiding disincentives to serving people with
greatest need
published by Social Policy Research
Unit, University of York.
Corden, Anne & Sainsbury, Roy (2001)
Incapacity Benefits and Work Incentives
Department for Work and Pensions Research Report
no 141
Cotton, Kathleen (2001)
Developing Employability Skills, Close-up #15
in
School Improvement Research Series C
Crawford, Cameron 1992
Why people with disabilities can’t get jobs and how
we can solve that problem: An introduction to On
Target. In Entourage Autumn 1992
Crowther, Ruth E; Marshall, Max; Bond, Gary R &
Helping people with severe mental illness to obtain
Huxley, Peter (2001)
work: systematic review. In British Medical
Journal Vol 322
Danziger, Sandra; Corcoran Mary; Danziger
Barriers to the employment of welfare recipients in
Sheldon; Heflin, Colleen; Kalil, Ariel; Levine,
Prosperity for all? The economic boom and
Judith; Rosen, Daniel; Seefeldt, Kristin; Siefert,
African Americans, ed R Cherry and WM
Kristine and Tolman Richard (2000)
Rodgers III. (Russell Sage Foundation)
Danziger Sandra K and Seefeldt Kristin S (2002)
Barriers to employment and the “hard to serve”:
implications for services, sanctions and time
limits in Focus 22 Vol 1
Davis, Mr
Return-to-Work Incentives. WCRI Research Brief.
June 1989
De Jong, Peter & Miller, Scott D
How to Interview for Client Strengths
De Jonge, Desleigh & Rodger, Syliva & Fitzgibbon,
Putting technology to work: Users’ perspective on
Heidi
integrating assistive technology into the
workplace. 20 June 2000
DeBord, Karen, Ph.D. & Matthews, Wayne D, Ph.D.
Work Front – Home Front: A Report on Work First
& Canu, Rebekah F & Parris, Pamela L S
Participant Work Family Balance
DeGroat, Bernie
Many Single Mothers on Welfare Face Multiple
Barriers to Employment. November 1998
Dench, S ; Meager, N & Morris, S
The Recruitment and Retention of People with
Disabilities, Institute for Employment Studies
Report 301
Dench, S and Regan J
Learning in later life: motivation and impact,
Department for Education and Employment
Research Report 183
Department of Employment and Workplace
Employer attitudes about job seekers in 2001
Relations, Australia 2001
Employer survey papers, Topic 5
Department of Labour, NZ 1999
Human Capability: a framework for analysis
Department of Labour, NZ 2003
Work trends: how work is changing in New Zealand
Department for Work and Pensions, UK 2002
Helping People into Employment
Page 133 of 144
Department for Work and Pensions, UK
New deal for job-seekers. Summary of new deal:
self-employment
Douglas Ezzy, Dept of Sociology, La Trobe
Unemployment and Mental Health: A Critical
University, Bundoora, Australia 3083
Review
Drake RE; McHugo GJ; Bebout RR; Becker DR;
A randomised control trial of supported employment
Harris M; Bond GR and Quimby E (1999)
for inner-city patients with severe mental
disorders in Archives of General Psychiatry Vol
56
Eardley, Tony & Thompson, Merrin.
Social Policy
Does Case Management Help Unemployed Job
Research Centre (1999)
Seekers on website
http://www.coss.net.au/library/6034.html
Ehret, Richard
Vocational Rehabilitation in Workers
Compensation: The Good, the Bad, the Ugly.
December 1988
Evans, Martin; Eyre, Jill; Millar, Jane and Sarre
New Deal for Lone Parents: second synthesis report
Sophie (2003)
of the national evaluation. Published by
Department for Work and Pensions UK
Franz, John B. Fresno Pacific College
Cognitive Development and Career Retraining in
Older Adults. 1983
Fraser, Robert T & Shrey, Donald E
Perceived Barriers to Job Placement Revisited:
Toward Practical Solutions. 1986
Frederickson BE; Trief PM; Van Beveren P: Yuan
Rehabilitation of the patient with chronic back pain:
HA and Baum G (1988)
a search for some outcome predictors in Spine
1988 Vol 13
Fried, Barbara
The Transitional Employment Approach. 27-29
October 1993
Fryer, David & Payne, Roy
Being Unemployed: a Review of the Literature on
the Psychological Experience of Unemployment.
1986
Galizzi Monica and Boden Leslie I (1996)
What are the most important factors shaping return
to work? Evidence from Wisconsin, published
Workers Compensation Research Institute,
Galluf Tate, Denise
Factors Influencing Injured Employees Return to
Work. 24 February 1992
Gard, Guvnor & Sandberg, Christine
Motivating Factors for Return to Work in
Physiotherapy Research International Vol 3 no
2
Gardner, John A
Return To Work Incentives Lessons For Policy
Makers From Economic Studies, June 1989
Gardner, John W, MD, March 16 2000
Smoking Linked to Physical Injuries Centre for the
advancement of health on web-site
www.hbns.org/newsrelease/smoking3-16-00.cfm
Geers, Frederik
New Strategies to Combat Long-Term
Unemployment in Belgium. 1991
Gilbride, Dennis D & Stensrud, Robert 1992
Demand-Side Job Development: A Model for the
1990s. in Journal of Rehabilitation
Oct/Nov/Dec 1992.
Goldstone, Carol with Meager, Nigel (2002)
Barriers to employment for disabled people
Department for Work and Pensions In-house
Page 134 of 144
Report no 95
Graves Sheri
Job ready in just a few months in The Press
Democrat August 10, 2003
Greenough CG and Fraser RD (1989)
The effects of compensation on recovery from low-
back injury in Spine Vol 14
Greenspan AI, Wrigley JM, Kresnow M, Branche-
Factors influencing failure to return to work due to
Dorsey CM, and Fine PR (1996)
traumatic brain injury in Brain Injury 1996 Vol
10
Gregson JA and Bettis PJ (1991)
Secondary Trade and Industrial Education work
Values Instruction: Emancipatory or
Indoctrinational? Paper
presented at the
American Vocational Association Convention,
Los Angeles, CA. (ED 341 781)
Griffin Carey and Hammis Dave
Is Self-employment a cop-out? On
<www.diversityworld.com/Disability/selfempl.
htm#Cop-Out>
Gun, R T & Fraser, R D
The Therapeutic Effects of a Return to Work
Hamilton, V Lee; William S Hoffman, Clifford L
Unemployment, Distress and Coping: A Panel Study
Broman & David Rauman. 1993
of Autoworkers Journal of Personality and Social
Psychology Vol 65 No 2
Hangley, Bill Jr & Loizillon, Anais
The Transition work corporation:
Philadelphia@Work. An Innovative Welfare-to-
Work Strategy for Participants with Substantial
Job-Readiness Barriers
Harald Reiso MD; Jan F Hygard BSc, BA; Gudrum S
Back to work: Predictors of Return to Work Among
Jorgensen; Rune Holanger; Dag Soldal MD &
Patients with Back Disorders Certified as Sick
Dag Bruusgaard MD, PhD
Harries, Tim & Woodfield, Kandy (2002)
A qualitative evaluation of transitional support for
clients returning to employment Department for
Work and Pensions Research Report No 175
Harries, Tim & Woodfield, Kandy
Easing the Transition to Work. 2002
Heenan, Deirdre
“It won’t change my world but it turned my life
around”: participants’ views on the Personal
Advisor Scheme in the New Deal for Disabled
People. 2002
Heidi Goldberg (Centre on budget and Policy
Improving TANF program outcomes for families
Priorities)
with barriers to employment
Hendler, MD, Nelson
Return to Work Barriers and How to Overcome
Them
Hershey, Alan M & Pavetti, LaDonna A
Turning Job Finders into Job Keepers
Hillage J and Pollard E
Employability: developing a framework for policy
analysis, Department for Education and
Employment Research Report No 85
Hills, Dione; Child, Camilla; Blackburn, Vicky and
Evaluation of the New Deal for Disabled People
Youll, Penny (2001)
pilots Department for Work Pensions:
Research Report
143
Hogelund, Jan. Who Returns to Work and Why?
Work Incapacity and Reintegration: A Literature
Review
Page 135 of 144
Holzer H (1996)
What employers want: Job prospects for less-
educated workers Russell Sage Foundation
Honey S and Williams N
Supply and demand for supported employment,
Department for Education and Employment
Research report no 70
Hoogendoorn, Wilhelmina E;van Poppel Mireille;
Systematic Review of Psychosocial Factors at Work
Bongers, Paulien M; Koes Bart; & Bouter Lex 1999
and Private Life as Risk Factors for Back Pain.
In Spine Vol 25 no 16
CTS Rehabilitation Specialists Programme on
http://p2001.health.org/Rs01/MODULE4PM.htm
HRDC (1998)
Evaluation of the Employability Improvement
Program published by Human Resources
Development Canada
HRDC (1997)
Lessons Learned : A Review of Older Worker
Adjustment Programs published by Human
Resources Development Canada
HRDC (1998)
Possible measures to improve labour market
adjustment for older workers published by
Human Resources Development Canada
Hutchinson J (1999)
Job rotation: linking learning, business growth and
unemployment? In Local Economy vol 14
Inge, Katherine J & Strobel, Wendy
Vocational outcomes for persons with severe
physical disabilities: design and implementation
of workplace supports
Institute for Employment Studies, 2002
New Deal 50plus: Sustainability of Employment –
Synopsis
Institute for Research on Poverty (2000)
Barriers facing the hard-to-serve population on
web-site <www.ssc.wisc.edu/irp/events/wel-
conf.htm>
Institute of Work Psychology
A Positive Approach to Older Workers
International Social Security Review
Netherlands Serious Steps to Resolve Longstanding
Problems
Ivar Lodemel & Heather Trickey (2001)
An offer you can’t refuse. Workfare in international
perspective The Policy Press
Jackman GJ 2000
Will new employment opportunities become a
reality in this new millenium? Cracow 2000
Conference proceedings at www.icevi-
europe.org/cracow2000/proceedings/chap0
7.html
Jahoda M 1979
The psychological meanings of unemployment in
New Society 6 Sept 1979
Jenaro, Cristina & Mank, David & Bottomley, John
Supported Employment In The International
& Doose, Stefan & Tuckerman, Phil
Context: An Analysis Of Processes And
Outcomes. 2002
Johnson, Leslie Stratton & Archer-Heese, Gail &
Work Hardening: Outdated fad or effective
Caron-Powles, Deanne L & Dowson, Tracey M
intervention? 20 June 2000
Johnson, William G & Baldwin, Marjorie L &
Back Pain and Work Disability: the need for a new
Page 136 of 144
Butler, Richard J (1998)
paradigm. In Industrial Relations Vol 37
Johnson, William G, Richard J Butler & Marjorie
First Spells of Work Absences Among Ontario
Baldwin, 1995
Workers in Research in Canadian Workers’
Compensation ed Terry Thomasen and Richard P
Chaykowski published IRC Press
Johnson, William G and Ondrich J (1990)
The duration of post-injury absences from work in
Review of Economics and Statistics No 72
Joseph Rowntree Foundation
The Working Families Tax Credit: Options and
Evaluation
Kalil, Ariel; Corcoran Mary E; Danziger Sandra K;
Getting Jobs, Keeping Jobs, and Earning a Living
Tolman Richard; Seefeldt, Kristin S; Rosen, Dabniel;
Wage: Can Welfare Reform Work? Institute for
and Nam, Yunju (1998)
Research on Poverty Discussion Paper 1170-
98
Kellard, Karen & Adelman, Laura & Cebulla,
From job seekers to job keepers: job retention,
Andreas & Heaver, Clare (2002)
advancement and the role of in-work support
programmes. Department for Work and
Pensions Research Report no 170
Kellard, Karen, Legge, Kate & Ashworth, Karl
Self-employment as a route off benefits Research
(2003)
report no 177 Department for Work and
Pensions
Kisthardt, Walter E & Gowdy, Elizabeth & Rapp,
Factors Related to Successful Goal Attainment in
Charles A
Case Management
Krause, Niklas & Dasinger, Lisa & Wiegand,
Does Modified Work Facilitate Return To Work For
Andrew
Temporarily Or Permanently Disabled Workers?
20 August 1997
Kremer, James 2003
New Directions in Return to Work in Journal of
Workers’ Compensation Vol 12 no 4
Ktrentzman 2003
The Krentzman Obesity Newsletter, April /
May 2003, Volume 10, Number #4
Kwong SS (2000)
Retraining for the Unemployed – an uphill battle
that never ends on web=site
www.erb.org/current/pr000809/Erb_pr2.pdf
Larson, Barbara A
The Aging Worker. 2001
Laudet, A., Magura, S. Vogel, H. & Knight, E.
Recovery challenges among dually-diagnosed
(2000)
individuals in Journal of Substance Abuse
Treatment, Vol 18 No 4
Lazarus, Richard S (1983)
The Costs and Benefits of Denial in The Denial of
Stress, ed S Breitnitz
Lazarus, Richards S and Folkman Susan (1984)
Stress, Appraisal and Coping
Leana, Carrie R & Feldman, Daniel C
Finding New Jobs After a Plant Closing: Antecedents
and Outcomes of the Occurrence and Quality of
Reemployment. 1995
Litmus Research Company
Returning long term claimants to independence: a
summary of qualitative interviews with
claimants, July 2003
Loeb Sara (2003)
Execs out of shape for today’s market in Skokie
Page 137 of 144
review February 27, 2003
Loumidis, Julia; Stafford, Bruce; Youngs, Rachel ;
Evaluation of the New Deal for Disabled People
Green Anne; Arthur, Sue; Legard, Robin; Lessof,
Personal Advisor Pilots Department for Work
Carli; Lewis, Jane; Walker, Robert; Corden,
Pensions: Research Report No 144
Anne; Thornton, Patricia and Sainsbury, Roy
(2001)
Luft, Harold S (1975)
The Impact of Poor Health on Earnings in
Review
of Economics and Statistics. Vol 57 no 1
Lunt, Neil & Thornton, Patricia 1994
Disability and Employment: towards an
understanding of discourse and policy in
Disability and Society Vol 9 No 2
.
Manitoba League of Persons with Disabilities
Barriers to Re-employment of injured workers with
significant disabilities on web-site
<www.mlpd.mb.ca>
Mannock, Thomas J & Levesque, Deborah A &
Assessing Readiness of Clients with Disabilities to
Prochaska, Janice M (2002)
Engage in Job Seeking Behaviours in Journal of
Rehabilitation July.Aug/Sept 2002
Manuel Jude 2003
Survey of former clients of job search website Seek
Marhold, Charlotta & Linton, Steven J & Melin,
A cognitive-behavioral return-to-work program:
Lennart (2001)
effects on pain patients with a history of long-
term versus short-term sick leave. In Pain Vol
91
Marhold, Charlotta; Linton, Steven J and Melin,
Identification of Obstacles for Chronic Pain Patients
Lennart (2002)
to Return to Work: Evaluation of a Questionnaire
in Journal of Occupational Rehabilitation Vol
12 No 2
Marini, I
A Fischler & N Booth Vocational Impact of
Psychiatric Disorders: A Guide for
Rehabilitation Professionals. In Work 21, 2003
Martinson, Karin & Strawn, Julie
Built to Last: Why Skills Matter for Long-Run
Success In Welfare Reform. May 2002
Mathematica Policy Research Inc
Families on TANF in Illinois: Employment Assets
and Liabilities
Mautz, Denise & Storey, Keith & Certo, Nick
Increasing Integrates Workplace Social Interactions:
the Effects Of Job Modification, Natural
Supports, Adaptive Communication Instruction,
And Job Coach Training. 2001
McCormick, B
Unemployment Structure and the Unemployment
Puzzle. 1991
McIntosh, Greg & Melles, Tony & Hall, Hamilton
Guidelines for the Identification of barriers to
Rehabilitation of Back Injuries
in Journal of
Occupational Rehabilitation Vol 5 No 3
Mead Laurence M (1998)
The decline of welfare in Wisconsin, Institute for
Research on Poverty Discussion paper 1164-
98
Meager, Nigel; Bates, Peter and Cowling Marc 2003
Business start-up support for young people delivered
by the Prince’s Trust. Department for Work
and Pensions Research Report no 184
Meager, N & Bates, P & Dench, S & Honey, S &
Employment of Disabled People: Assessing the
Page 138 of 144
Williams, M
Extent of Participation
Melhorn, J Mark
The Benefits of Returning the Injured Worker to
Work Early: A Review of the Research in Journal
of Workers Compensation
Melzack R and Wall PD (1965)
Pain Mechanisms- a new theory. In Science Vol
150
Michalopolous Charles and Schwartz, Christine
What works best for whom? Impacts of 20 welfare
with Adams-Ciardullo, Diana (2000)
to work programs by sub-group. Report for the
National Evaluation of Welfare to Work
Strategies (NEWWS)
Millman, Zeeva & Latham, Gary
Increasing Reemployment Through Training in
Verbal Self-Guidance
Mills, R & Thornton J 1998
Return-to-work outcomes in acute, work-related low
back pain in Journal of Occupational Health
and Safety – Australia and NZ Vol 14 no 6
Monthly Labour Review
Developing Employment Policies for Persons with
Disabilities. October 1992
Morgantown, W V
Job Accommodation Network (JAN), Job
Accommodation Network annual report:
October 1, 1992 through September 30, 1993
Mueser, KT; Becker DR and Wolfe R (2001)
Supported Employment, job preferences, job tenure
and satisfaction in Journal of Mental Health
Vol 10 no 4
Murrell KFH and Humphries S (1978)
Age, experience and short-term memory in MM
Gruneberg, PE Morris and RN Sykes (eds)
Practical Aspects of Memory (Academic Press)
New York State Education Department
Job Coaching. 1998
Nicholas Michael K (2002)
Work hardening / conditioning: Functional
restoration and pain management programs.
New South Wales WorkCover
Nightingale, Demetra Smith & Holcomb, Pamela A
Alternative Strategies for Increasing Employment in
(1997)
Welfare to Work Vol 7 No 1 Spring 1997
Nijboer, I D & Grunemann, R W M & Andries, F
Work Resumption After Disability. 1993
Noer, David N (1996)
Breaking Free: a prescription for personal and
organisational change. 1996
North Dakota Workers Compensation
Preferred Worker Programme
NZES
The Barriers to Employment Faced by Long Term
Job Seekers: Key Findings from a Survey of New
Zealand Employment Service Clients. December
1996
O’Day, Bonnie, (1999)
Policy Barriers for People with Disabilities who
Want to Work in American Rehabilitation
Spring/summer 1999
OECD 2003
Disability programmes in need of reform OECD
Policy Brief
Page 139 of 144
Pack Margaret 2003
Exploratory research on ACC’s longer term
claimants Internal ACC report.
Parente R and Stapleton M (1999)
Development of a cognitive strategies group for
vocational training after traumatic brain injury
in NeuroRehabilitation, No 13
Parker, Brett (1997)
Very long-term job seekers’ barriers to employment:
a nationwide survey in Labour Market Bulletin
1997 vol 1
Payne, Roy & Hartley, Jean
A test of a model for explaining the affective
experience of unemployed men. 1987
Payne, Clive and Payne, Joan 2000
Early identification of the long term unemployed
Policy Studies Institute Research Discussion
Paper 4
Peale, Norman Vincent Dr
The Power of Positive Thinking. 1952
Perrin, Burt (1999)
Lessons learned from evaluation of disability policy
and programs Prepared for Human Resources
Development Canada
Phillips, J S & Barrett, G V & Rush, M C(1978)
Job Structure and Age Satisfaction, Aging and
Work. 1978
Pimentel (undated)
Attitudinal barriers should not run amok in the
workplace in Thompson Publishing group
Inc’s ADA Compliance Guide Monthly
Bulletin
Pimentel Richard, 2001
Return to work for people with stress and mental
illness in MWA Update on website
<www.miltwright.com/mwa_update>
Pimentel Richard (1999)
Working therapy in Recovery, Vol 10 No 2
Polit, Denise & London, Andrew & Martinez, John
The Health of Poor Urban Women: Findings from
the Project on Devolution and Urban Change,
Manpower Demonstration Research Corporation.
May 2001
PricewaterhouseCoopers
The Impact of Compensation Pathways on Health
Social and Economic Outcomes of NSW Workers
Compensation Claimants: Results of a
Qualitative Study
Proscio, Tony & Elliott, Mark (undated)
Getting in Staying on Moving up: A Practitioner’s
Approach to Employment Retention published
by Public/Private Ventures
Proudfoot Judith; Guest David; Carson Jerome;
The effect of Cognitive-Behavioural training on job-
Dunn Graham and Gray Jeffrey (1997)
finding among long term unemployed people in
The Lancet Vol 350
Rangarajan, Anu; Schochet, Peter and Chu, Dexter
Employment experiences of welfare recipients
1998
who find jobs – is targetting possible?
Mathematica Policy Research
Rapp CA and Wintersteen R (1989)
The Strengths model of case management
in
Psychosocial Rehabilitation Journal, 13 (1)
Ravesloot Craig and Seekins Tom (1996)
Vocational rehabilitation counselors’ attitudes
towards self-employment outcomes in
Page 140 of 144
Rehabilitation Counselling Bulletin Vol 39 No 3
Regan, Sue & Stanley, Kate
Work for Disabled People
Regeringskansliet (Factsheet) from Swedish
Some gender equality initiatives in 2002
Ministry of Industry, Employment and
Communications
Reiso, Harald; Nygard, Jan; Jorgensen, Gudrun;
Back to work: Predictors of return to work among
Holanger, Rune; Soldal, Dag; and Bruusgaard,
patients with back disorders certified as sick in
Dag 2003
Spine Vol 28 no 13
Relave, Nanette, 2000
Promoting employment Retention in Welfare
Information network Vol 4 No 9
Reynolds Timothy M
Top 10 Things plaintiffs’ lawyers love
Rick J and Briner R (2000)
Trauma management vs stress debriefing: what
should responsible organisations do? Institute
for Employment Studies
Rick J; Young K; and Guppy A
From accidents to assaults: how organisational
responses to traumatic incidents can prevent
Post-traumatic Stress Disorder (PTSD) in the
workplace, HSE Contract Research Report
195/98
Riddell, Sheila (2002)
Work Preparation and Vocational Rehabilitation: A
Literature Review Strathclyde Centre for
Disability Research
Rizzo, Dennis C
With A Little Help From My Friends: Supported
Self-Employment For People With Severe
Disabilities. 2002
Roehling M 1999
Weight based discrimination in employment:
psychological and legal aspects in Personnel
Psychology 1999 Vol 52
Rosdahl, Anders & Weise, Hanne
When all must be active – Workfare in Denmark
Ruffolo, Carol F, & Friedland, Judith F & Dawson,
Mild Traumatic Brain Injury From Motor Vehicle
Deirdre R & Colantonio, Angela & Lindsay,
Accidents: Factors Associated With Return To
Peter H
Work. April 1999
Schneider P (1998)
Work interventions in mental health: some
arguments and recent evidence in Journal of
Mental Health Vol 7
Schonstein E; Kenny DT; Keating J and Koes BW
Work conditioning, work hardening and functional
(2003)
restoration for workers with back and neck pain
in The Cochrane Library, Issue 2 2003
Shaw, Andrew & Walker, Robert & Ashworth, Karl
Moving Off Income Support: Barriers and Bridges
& Jenkins, Stephen & Middleton, Sue
Sheahan, Justice Terry
Using ADR in the resolution of workers
compensation disputes on web-site
www.leadr.com.au/SHEAHAN.PDF
Siegal HA Fisher, JA, Rapp, RC, Kelliher, CW,
Enhancing substance abuse treatment with case
Wagner, JH, O'Brien, WF, & Cole,
management: its impact on em,ployment in
PA (1996).
Journal of substance abuse treatment Vol 13
no 2
Page 141 of 144
Sim, Joann
Improving Return-to-Work Strategies in the United
States Disability Programs, with Analysis of
Program Practices in Germany and Sweden.
1999
Smart Solutions, Issue 4
Published by the Welfare to Work Partnership,
District of Columbia, September 2000
Smedmark, Goran. International Social Security
The Swedish Social Insurance System: A Model in
Review
Transition
Smith, C Landon
Chronic Back Strain. September 1997
Snape, Dawn (1997)
Recruiting Long-Term Unemployed People
Research Report no 76 Department for Work and
Pensions
Southgate David (2003)
Is any job better than no job? On web-site
<www.itmanagement.earthweb.com/career/article.p
hp/3081071>
Spruck Wrigley, Heide & Richer, Elise &
The Language of Opportunity: Expanding
Martinson, Karin & Kubo, Hitomi & Strawn, Julie
Employment Prospects for Adults with Limited
English Skills
Staal, J Bart & Hlobil, Hynek & van Tulder, Maurits
Return-to-Work Interventions for Low Back Pain in
W & Koke, Albere J A & Smid, Tjabe & van
Sports Medicine 2002 Vol 32 No 4
Mechelen, Willem (2002)
Sterns, Harvey L
The Aging Worker in a Changing Environment:
Organizational and Individual Issues. 1995
Sterns, Harvey L
The Aging Worker in a Changing Environment:
Organisational and Individual Issues
Sterns, Harvey L & Doverspike, Dennis
Aging and the Training and Learning Process
Stewart Jay R and Gomez Angelo
Interventions in the medical rehabilitation setting
with patients who deny disabling conditions on
<www.bgsu.edu/colleges/edhd/EIS/DIS/denial.
html>
Storey, Keith & Certo, Nicholas J
Natural supports for increasing integration in the
workplace for people with disabilities: A review
of the literature and guidelines for
implementation
StrohmerDC; Pellerin MF; and Davidson KJ (1995)
Rehabilitation counselor hypothesis testing: the role
of negative information, client disability, and
counselor experience in Rehabilitation
Counseling Bulletin Vol 39 No 2
Stutzman Linda J (2001)
Evidence-based return-to-work guidelines in
California Workers’ Compensation Enquirer
Vol 19 No 2
Sum Juliann D , Frank John, Faucett Julia and Stock
Return to work in California: listening to
Laura (2001)
stakeholders’ voices prepared for the
(California) Commission on Health and Safety
and Workers’ Compensation
Swedish Institute
Disability Policies in Sweden. January 2000
Tainter, Suzanne
Mental Health Among Single Mothers: Assessing
the Consequences of Welfare Reform
Page 142 of 144
Tamkin P, Hillage
Employability and Employers: the missing piece of
the jigsaw
Te Puni Kokiri
Te Puni Kokiri Review of the Adequacy of ACC’s
Service Delivery to Maori. 1998
Texas Workers’ Compensation Commission
Return to Work Program for Employer
Thomas, Andrew & Pettigrew, Nick & Cotton,
Keeping in Touch with the Labour Market: A
Daphne & Tovey, Paul. Department for Work
Qualitative Evaluation of the Back to Work
and Pensions
Bonus.
Thomas, T
Disabled Students’ Experience of DipSW
Programmes and the Need for Action. 1999
Thornton, C & Hershey, A (1990)
After REACH: Experience of AFDC recipients who
leave welfare with a job Mathematica Policy
Research
Thornton, Patricia (1999)
International Research Project on Job Retention and
Return to Work Strategies for Disabled Workers
published ILO
Thornton, Patricia & Corden, Anne
Evaluating the Impact of Access to Work: A Case
Study Approach Research & Development
Report WAE138, Department for Work
and Pensions
Thornton, Patricia & Lunt, Neil (1994)
Disability and Employment: towards an
understanding of discourse and policy. In Doing
Disability Research, eds Colin Barnes and Geof
Mercer
Tu Mauri 2000
The Tomoana Resource Centre – an intervention
following job loss in Social Policy Journal of NZ
Issue 15
Unger Donna and Kregel John (2003)
Employers’ knowledge and utilizations of
accommodations in Work Vol 21 (2003)
University of Michigan
Barriers to the Employment of Welfare Recipients.
February 2000
University of Michigan
Barriers to the Employment of Welfare Recipients.
February 2000
University of Toronto
International Study on Job Retention and Early
Return to Work Strategies for Disabled Workers.
US Department of Health & Human Services
Ancillary Service to Support Welfare to Work:
Specialised Child Care
Utesch William E undated
From a glass half empty to a glass half full: a
review of the transition from deficit to strength
based approaches Foellinger Foundation
Van Den Berg, H & Van Der Veer, C.G.
The Myth Of ‘Unemployable’ People: An Evaluation
Of A New Employment Services For The ‘Hard
Core’ Unemployed in Journal of Social Policy
Vol 21 No 2, 1990
Voices
Voices of people with disabilities on web-site
www.returntowork.org/voices.html
Page 143 of 144
Warner R (2001)
Work disincentives in US disability programmes in
Journal of Mental Health Vol 10 no 4
Warr, Peter & Lovatt, Jerry
Retraining And Other Factors Associated With Job
Finding After Redundancy. 1977
Waters, Lea E & Moore, Kathleen A
Self-esteem, appraisal and coping: a comparison of
unemployed and re-employed people. August
2001
WCR
Research Brief
Return to work incentives, June 1989
Wehipeihana, Nan (2002)
Conduit Intensive Support Programme Evaluation
Report. Prepared for Work and Income NZ
White, J (Prairie Women’s Health Centre of
Health Care System in Atlantic Canada Neglects
Excellence)
Immigrant, Refugee and Minority Women
Wiseman, Michael (1996)
State strategies for welfare reform: The Wisconsin
story in Journal of Policy analysis and
management Vol 15 no 4
Woodland, Stephen; Mandy, William and Miller,
Easing the transition into work (part 2 – client
Melissa (2002)
survey) Department for Work and Pensions
Research Report no 186
www.europa.eu.int/comm/employment_social/news
Impact Evaluation of the EES. Employment
/2002/may/inclusion_en.pdf
Strategy
www.mlpd.mb.ca/reports
External Factors Influencing Re-Employment
www.mlpd.mb.ca/reports/html/wwdp/wwdppage8.h Studies of Post-Injury Employment
tml
www.twcc.state.tx.us/commission/divisions/rtw
Return to Work Program for Employers
Yasuda S., Wehman P., Targett P., Cifu D X., West
Return to work after spinal cord injury: A review of
M (2002)
recent research NeuroRehabilitation, 17(3), 177-
186
Yasuda, S & Wehman, P & Targett, P & Cifu, D &
Return To Work For Persons With Traumatic Brain
West, M
Injury
Page 144 of 144
 Brief Report:
Interventions for the management of long term ACC
clients in receipt of weekly compensation
Reviewer
Fiona Conlon
Date Report Completed
Important Note:
Brief Report:
Interventions for the management of long term ACC
clients in receipt of weekly compensation
Reviewer
Fiona Conlon
Date Report Completed
Important Note:
The purpose of this brief report is to summarise information on the effectiveness of
interventions for the management of long term ACC clients in receipt of weekly
compensation and to provide best practice advice. It has not been systematically
developed according to a predefined methodology.
The document has been prepared by the staff of the evidence based Healthcare
Advisory Group, ACC. The content does not necessarily represent the official view
of ACC or represent ACC policy.
This report is based upon information supplied up to 9 December 2008
A c c i d e n t C o m p e n s a t i o n C o r p o r a t i o n
Executive Summary
This report examined the effectiveness and evidence for interventions for the management
of long term ACC clients in receipt of weekly compensation.
Some key findings are:
Implementing intensive case management within a system which focuses on
compensation and medical interventions (including surgery) can be difficult.
Knowledgeable medical and rehabilitation professionals who can provide advice
that dovetails with the reality of the workplace setting are vital.
The medicalisation of injury can result in inferior outcomes in terms of RTW and a
national guidance on, for example, post operative RTW advice, could be beneficial.
There is evidence for promoting RTW through interventions that target the
emotional demands of work, job security, perceived ability to perform tasks,
meeting role expectations and obtaining workplace support.
Management of injury in the workplace, rather than off-site in rehabilitation
centres shows good evidence for success in terms of reducing work disability
duration and associated costs.
Background
There has been increased concern in ACC about the growth in the number of long term
claims. The management of these claims presents a challenge in terms of resources and
cost. The Evidence Based Healthcare (EBH) Research Group has been asked to provide a
high level review of recent literature based on abstracts and conversations to present the
available evidence on interventions to address this issue.
Investigation
The search strategy involved a search of the Ovid MEDLINE® 1996 to November Week 3
2008 database. The search was conducted on 9 December 2008 using key words relevant
to long term claims
361 abstracts were identified and reviewed to identify emerging themes and ideas.
A c c i d e n t C o m p e n s a t i o n C o r p o r a t i o n
Page 2
Systematic reviews and RCTs were included together with other studies especially where
they supported the evidence. The quality of the research studies was not evaluated and
further review of the quality of research available is therefore recommended.
Other sources of information:
Conversation with Cam Mustard, President and Senior Scientist, Institute for Work and
Health; Professor, School of Public Health, University of Toronto – (Telephone Conference
on 18 December 2008).
‘
Barriers facing long term unemployed, injured or disabled workers returning to work – report
on international literature search’. Compiled for ACC by Fiona Knight, 16 January 2004.
Results
The themes identified and the evidence related to these themes are summarised.
The influence of the medical model of health
There is good evidence to show that being fully recovered is not a stipulation for regaining
work activities and a more function centred approach to treatment rather than a pain
centred approach can be more effective for increasing RTW1 2.
Healthcare providers can play an active role in the RTW process, a role that includes direct
contact with the workplace and proactive communication with the patient. The influence
of the GP or healthcare professional’s advice regarding absence duration influences the
outcome and times for RTW3 4 5.
The use of a medical paradigm for the assessment, explanation and treatment of what are
often social conditions can generate interventions inappropriate to the problem.
Implementing intensive case management within a system which focuses on compensation
and medical interventions (including surgery) can be difficult. Patients may request more
testing and passive medical interventions, delaying the initiation of functional restoration.
More tests and pain related treatments may also reinforce a patient’s false expectations for
a cure6. Knowledgeable medical and rehabilitation professionals who can provide advice
that dovetails with the reality of the workplace setting are vital. Doctors may not know the
type of work that their patients are returning to; both a lack of knowledge and ambiguity
about their role can influence outcomes7 8 9.
A c c i d e n t C o m p e n s a t i o n C o r p o r a t i o n
Page 3
There is some evidence to show that the primary treating physician’s behaviour can
increase the likelihood of a RTW, while recommendations for specialty care can reduce the
likelihood of RTW10. Similarly interventions targeting RTW applied in the acute phase of
an injury can compete with a high rate of spontaneous recovery and may therefore be
inefficient11. Another study of those who seek additional health care services after
completion of a tertiary rehabilitation programme showed that this sub group accounted
for a significant proportion of lost worker productivity, unremitting disability payments
and excess healthcare consumption12. This suggests that the medicalisation of injury can
result in inferior outcomes in terms of RTW and a national guidance on, for example, post
operative RTW advice, could be beneficial5.
The Workplace Safety and Insurance Board in Canada issued “Injury/Illness and Return to
Work/Function: A Practical Guide for Physicians” in 2000 for treating physicians. It
highlights the need for primary care providers to lead in coordination and collaborative
roles with other stakeholders (e.g. workplace parties) in the context of encouraging safe
and timely return to work. Similarly in Ontario, guidelines were released based on
evidence based research for the management of patients in relation to low back pain. It is
suggested that guidelines must be accompanied by effective service support to primary
care providers to be successful (Conversation with Cam Mustard).
Ontario is currently trialling a demonstration model in which primary health care
providers have funding for a position within the health centre for a person dedicated to the
coordination of RTW for injured persons, working collaboratively with the workplace and
the compensation agency. This new innovation has not yet been evaluated (Conversation
with Cam Mustard).
Workplace Organisation
Workplace interventions consisting of workplace assessments, work modifications and
case management involving all stakeholders show good evidence of success and cost
effectiveness with respect to RTW outcomes13 14 15 16.
The organisation of the workplace is important for RTW outcomes. For both men and
women the likelihood of RTW improved with the increasing number of opportunities to
“adjust”. Adjustment latitude (i.e. opportunities to adjust one’s work to one’s state of
health by choosing among work tasks and deciding about work pace and working hours)
increased returning to work part time as well as full time work17. The ability to modify
work rather returning to full duties has a lower risk of recurrence18.
A c c i d e n t C o m p e n s a t i o n C o r p o r a t i o n
Page 4
There is good evidence to show that the predictors of RTW that are considered most
clinically relevant are those that generally reflects the way the workplace operates. Physical
recovery is embedded in complicated ways with workplace processes and practices
together with environmental and social organisation in the workplace – good will and
trust are important19 20. Key factors in the workplace culture and organisation that effect
RTW identified in the literature are:
A culture of problem solving and injury management strategies
In house disability management programmes by corporate based case managers
Knowledge exchange
Equitable participation of workers, supervisors and health professionals
Positive work culture and people oriented organisational policies and procedures
A safety climate and ergonomic practices (including accommodation)
Co-worker support 21 22 23 24 25 26.
There is also evidence for promoting RTW through interventions that target the emotional
demands of work, job security, perceived ability to perform tasks, meeting role
expectations and obtaining workplace support27 28 29.
Prognostic factors for non Return to Work (RTW)
In determining the common risk factors for recurrence, chronicity and non return to work
in low back pain the prognostic factors with a high level of evidence were: a history of low
back pain, a low level of job satisfaction and poor general health. The prognostic factors
with a moderate level of evidence were: employment status, amount of wage, workers
compensation, depression and physical factors related to work30. Prevention of these
factors occurring and awareness of their influence is essential at all stages of work
disability and in determining interventions for RTW.
Stakeholder Influences
Injured workers often do not return to work due to a complex group of factors associated
with the development and persistence of the work disability. These factors include: the
worker, the work place system or environment, compensation policies, the healthcare
system and the insurance system. These systems are further exposed to multiple legal,
administrative, social, political and cultural exchanges. Loisel’s diagram provides an
overall societal context for the injured worker (see Diagram 1)31.
A c c i d e n t C o m p e n s a t i o n C o r p o r a t i o n
Page 5
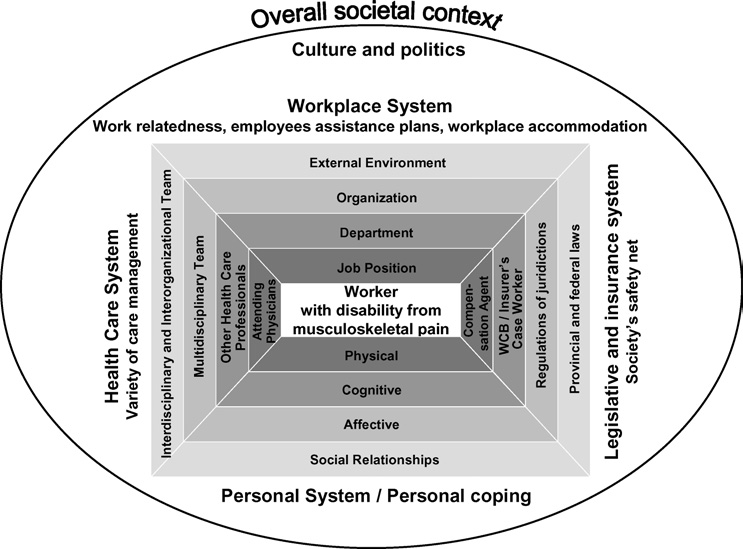
Any intervention directed at RTW outcomes is influenced by the diverse and competing
interests, values and language of the worker, employers, insurers, labour representatives
and healthcare providers. Frictions are inevitable and interventions need to meet common
goals32. Some strategies like education and awareness raising between stakeholder parties
appear to offer results6.
Diagram 1. Figure adapted from Loisel et al, 200533
Workplace based interventions
Management of injury in the workplace, rather than off-site in rehabilitation centres shows
good evidence for success in terms of reducing work disability duration and associated
costs34 35 36 37. Work disability duration can be reduced by work accommodation offers,
contact between the healthcare providers and the workplace, early contact of the worker
with the workplace, ergonomic worksite visits with an intensive functional restoration
programme and the presence of a RTW coordinator38 39.
In the United Kingdom the Department of Work and Pensions is currently experimenting
with delayed benefit reduction; protecting beneficiaries from having their benefit reduced
or suspended for a period until they are established in the workplace. It is hoped that this
A c c i d e n t C o m p e n s a t i o n C o r p o r a t i o n
Page 6
will address job security issues and increase a claimant’s preparedness to take a chance on
RTW. (Conversation with Cam Mustard).
Case Management
There is good evidence to show that patients that received case management had fewer
sick days and a lower cost in terms of weekly compensation than those who did not
receive case management40 However there is no evidence to support any difference in
RTW outcomes with case management41.
Examples of case management in New Zealand include the Ministry of Social
Development’s PATHS (Providing Access to Health Solutions) programme, a partnership
between Work and Income, DHBs, PHOs, community Mental Health and NGOs in
collaboration. This programme utilises an intensive case management approach to help
clients identify their barriers or obstacles to preventing them from working. Options are
explored for removing barriers through access to services. PATHS was awarded the
“Excellence in Rehabilitation” at the New Zealand Health Innovation Awards 2008 (MOH
website). An evaluation of PATHS undertaken between July 2006 and June 2007 found
that in the Bay of Plenty it helped more than 550 people overcome health barriers and get
off benefits with 350 returning to work (Ministry of Health Website). The use of ‘Work
Brokers’, who work with employers and local training providers to grow and develop
opportunities in the local labour market, shows success.
Rehabilitation Interventions
There is inconsistent and conflicting evidence for different types of interventions on RTW
outcomes 42. For example studies reporting the effectiveness of Functional Capacity
Evaluations (FCE) varied in outcomes, some studies reporting that performance was a
weak indicator of faster benefit suspension and was unrelated to sustained recovery43 44 45.
Another study reported the need for accurate job simulation and detailed intensive
assessment of specific work activities for FCE to be a valid tool in RTW46.
One descriptive literature review on physical exercise reported that effects varied
depending on
content related factors (types of exercise, dosage, frequency, skills of health
care providers, etc) and
contextual factors (treatment setting, compensation scheme, etc)11.
It may be that the inter relationship between these factors account for the differences
between reported outcomes for different interventions.
In Ontario vocational rehabilitation programmes have had limited success: For those
claimants placed on a vocational rehabilitation programme, the attrition rate was 50%. Of
A c c i d e n t C o m p e n s a t i o n C o r p o r a t i o n
Page 7
the 50% who complete the programme only 50% of these successfully return to
employment, a success rate of 1 in 4 (Conversation with Cam Mustard).
Psychosocial factors
A systematic review to identify psychosocial predictors of failure to return to work in non-
chronic, non-specific low back pain found strong evidence that recovery expectation is
predictive of work outcome while depression, job satisfaction and stress or psychological
strain are not predictive of work outcome47. Persons with positive prediction require help
to realise their potential for RTW: offering traditional rehabilitation methods to a person
with negative prediction of his or her return to work could be a waste of time if done
ahead of improving self confidence and development of a positive view of what is
possible48.
There is some evidence for increased control for employees over decisions and actions
affecting their health – a process associated with the concept of ‘self efficacy’. Self efficacy
interventions and active involvement in one’s own condition, in relation to the workplace,
have shown positive effects on perceived workability49 50.
The health system can unwittingly reinforce the “sick role” and in so doing can provide
continued justification for an “off work” identity. Depression can become, through
institutional practices, inextricably part of someone’s identity with implications for their
functional recovery. It is uncertain whether low self efficacy among employees is a result
of the disability absence itself rather than a precursor of it51 52.
There is no evidence to show that counselling that addressed motivation, goal setting and
planning to return to work improved vocational outcomes53 54.
While many approaches focus on the psychosocial risk factors “inside” the individual (e.g.
pain, catastrophising, beliefs, expectancies) successful disability prevention and
management will require methods to assess and target psychosocial risk factors “outside”
the individual (e.g. interpersonal conflict in the workplace, job stress, etc)55
Alcohol and drug factors
Alcohol is known to play a significant role in absenteeism, reduction in work performance
and accidents in the workplace56 57 58 and, along with the consumption of drugs, is linked
to poor recovery after traumatic injury59.
A number of interventions show evidence for effectiveness including referral to alcohol
health workers as opposed to only providing information to injured clients60; providing
A c c i d e n t C o m p e n s a t i o n C o r p o r a t i o n
Page 8
motivational interventions and incentives to change behaviour61 57; peer based workplace
substance abuse prevention focusing on changing attitudes which can reduce the injury
rate62 63, and skills based substance abuse counselling programmes64.
The Department of Work and Pensions in the United Kingdom reported on substance
addiction prevalence and found it was higher in beneficiaries than the general population.
However, there is no evidence to show that drug and alcohol programmes within a RTW
programme are any more successful than programmes in the community (Conversation
with Cam Mustard).
Conclusions
From a review of the available evidence and conversations, it would appear that the
current approach to long term claimants is not wholly satisfactory. The challenges faced by
ACC are not unique and are typical of what is evidenced in other countries. The main
findings of this review are:
Recognition of the factors predisposing to chronicity, can improve outcomes.
Successful early intervention strategies are vital.
There is good evidence that a move a way from the medical model of managing
injury to functional management will result in improved outcomes.
Rehabilitation within the workplace environment can enhance outcomes.
Workplace processes and practices influence outcomes and opportunities for
worker control and self efficacy improve outcomes.
There is inconsistent evidence for various rehabilitation interventions and it would
seem that the context of the intervention is more important than the content. A
focus beyond the individual client to a wider focus on the context in which the
individual operates is required.
Specialist knowledge in the areas of case management, vocational expertise and
work brokering are required. GP/specialist behaviour modifications can also
enhance outcomes. The placement of a specialised person within the primary care
environment to focus of coordination of RTW shows promise.
The competing interests of all injury stakeholders need to be understood and
managed appropriately.
A c c i d e n t C o m p e n s a t i o n C o r p o r a t i o n
Page 9
Limitations of this report
This brief report has used abstracts from research studies and therefore the quality
of the research has not been reviewed. The brevity of the abstracts meant that
interventions were not fully explained and described and potential confounding
factors for the success of interventions possibly not identified.
The majority of the studies examine the effectiveness of interventions as early as 6
weeks from the time of injury and less from 3 to 6 months after injury. There were
few studies identified which looked at interventions for injured persons who had
been absent from the workforce for longer than one year.
Many studies related to sickness, rather than specifically to injury. Although many
studies focused on low back pain or non specific musculoskeletal disorders, they
cannot be applied to all injury disability.
The literature search did not reveal any information specific to New Zealand and
therefore compensation schemes and methods of intervention may not be
consistent with the New Zealand context. There were no studies identified relevant
to Maori and the area of cultural appropriateness of different interventions may
need to be explored.
References
1. Lotters F, Franche RL, Hogg-Johnson S, Burdorf A, Pole JD. The prognostic value of
depressive symptoms, fear-avoidance, and self-efficacy for duration of lost-time
benefits in workers with musculoskeletal disorders.[see comment].
Occupational &
Environmental Medicine 2006;63(12):794-801.
2. Kool J, Bachmann S, Oesch P, Knuesel O, Ambergen T, de Bie R, et al. Function-
centered rehabilitation increases work days in patients with nonacute nonspecific
low back pain: 1-year results from a randomized controlled trial.
Archives of
Physical Medicine & Rehabilitation 2007;88(9):1089-94.
3. Kosny A, Franche R-L, Pole J, Krause N, Cote P, Mustard C. Early healthcare provider
communication with patients and their workplace following a lost-time claim for
an occupational musculoskeletal injury.
Journal of Occupational Rehabilitation
2006;16(1):27-39.
4. Rasmussen K, Andersen JH. Individual factors and GP approach as predictors for the
outcome of rehabilitation among long-term sick listed cases.
Journal of Occupational
Rehabilitation 2005;15(2):227-35.
5. Clayton M, Verow P. Advice given to patients about return to work and driving
following surgery.
Occupational Medicine (Oxford) 2007;57(7):488-91.
A c c i d e n t C o m p e n s a t i o n C o r p o r a t i o n
Page 10
6. Loisel P, Durand M-J, Baril R, Gervais J, Falardeau M. Interorganizational Collaboration
in Occupationa; Rehabilitation: Perceptions of an Interdisciplinary Rehabilitation
Team.
Journal of Occupational Rehabilitation 2005;15(4):581-590.
7. Risi G. [Low back pain--from work incapacity to disability].
Therapeutische Umschau
2007;64(8):409-13.
8. Ouellette V, Badii M, Lockhart K, Yassi A. Worker satisfaction with a workplace injury
prevention and return-to-work program in a large Canadian hospital: the
importance of an integrated approach.
Work 2007;28(2):175-81.
9. Schweigert MK, McNeil D, Doupe L. Treating physicians' perceptions of barriers to
return to work of their patients in Southern Ontario.
Occupational Medicine
(Oxford) 2004;54(6):425-9.
10. Kominski GF, Pourat N, Roby DH, Cameron ME. Return to work and degree of
recovery among injured workers in California's Workers' Compensation system.
Journal of Occupational & Environmental Medicine 2008;50(3):296-305.
11. Staal JB, Rainville J, Fritz J, van Mechelen W, Pransky G. Physical exercise
interventions to improve disability and return to work in low back pain: current
insights and opportunities for improvement.
Journal of Occupational Rehabilitation 2005;15(4):491-505.
12. Proctor TJ, Mayer TG, Gatchel RJ, McGeary DD. Unremitting health-care-utilization
outcomes of tertiary rehabilitation of patients with chronic musculoskeletal
disorders.
Journal of Bone & Joint Surgery - American Volume 2004;86-A(1):62-9.
13. Anema JR, Steenstra IA, Bongers PM, de Vet HCW, Knol DL, Loisel P, et al.
Multidisciplinary rehabilitation for subacute low back pain: graded activity or
workplace intervention or both? A randomized controlled trial.
Spine 2007;32(3):291-8; discussion 299-300.
14. Hlobil H, Staal JB, Spoelstra M, Ariens GAM, Smid T, van Mechelen W. Effectiveness of
a return-to-work intervention for subacute low-back pain.[see comment].
Scandinavian Journal of Work, Environment & Health 2005;31(4):249-57.
15. Hlobil H, Staal JB, Twisk J, Koke A, Ariens G, Smid T, et al. The effects of a graded
activity intervention for low back pain in occupational health on sick leave,
functional status and pain: 12-month results of a randomized controlled trial.
Journal of Occupational Rehabilitation 2005;15(4):569-80.
16. Hlobil H, Uegaki K, Staal JB, de Bruyne MC, Smid T, van Mechelen W. Substantial
sick-leave costs savings due to a graded activity intervention for workers with non-
specific sub-acute low back pain.
European Spine Journal 2007;16(7):919-24.
17. Johansson G, Lundberg O, Lundberg I. Return to work and adjustment latitude among
employees on long-term sickness absence.
Journal of Occupational Rehabilitation
2006;16(2):185-95.
18. van Duijn M, Burdorf A. Influence of modified work on recurrence of sick leave due to
musculoskeletal complaints.
Journal of Rehabilitation Medicine 2008;40(7):576-81.
19. MacEachen E, Clarke J, Franche R-L, Irvin E, Workplace-based Return to Work
Literature Review G. Systematic review of the qualitative literature on return to
work after injury.[see comment].
Scandinavian Journal of Work, Environment &
Health 2006;32(4):257-69.
20. Muenchberger H, Kendall E, Grimbeek P, Gee T. Clinical utility of predictors of
return-to-work outcome following work-related musculoskeletal injury.
Journal of
Occupational Rehabilitation 2008;18(2):190-206.
21. Shaw L, Domanski S, Freeman A, Hoffele C. An investigation of a workplace-based
return-to-work program for shoulder injuries.
Work 2008;30(3):267-76.
22. Ossmann J, Amick BC, 3rd, Habeck RV, Hunt A, Ramamurthy G, Soucie V, et al.
Management and employee agreement on reports of organizational policies and
practices important in return to work following carpal tunnel surgery.
Journal of
Occupational Rehabilitation 2005;15(1):17-26.
A c c i d e n t C o m p e n s a t i o n C o r p o r a t i o n
Page 11
23. Schultz IZ, Crook J, Meloche GR, Berkowitz J, Milner R, Zuberbier OA, et al.
Psychosocial factors predictive of occupational low back disability: towards
development of a return-to-work model.
Pain 2004;107(1-2):77-85.
24. Post M, Krol B, Groothoff JW. Work-related determinants of return to work of
employees on long-term sickness absence.
Disability & Rehabilitation 2005;27(9):481-8.
25. Skisak CM, Bhojani F, Tsai SP. Impact of a disability management program on
employee productivity in a petrochemical company.
Journal of Occupational &
Environmental Medicine 2006;48(5):497-504.
26. Soeker MS, Wegner L, Pretorius B. I'm going back to work: back injured clients'
perceptions and experiences of their worker roles.
Work 2008;30(2):161-70.
27. Lund T, Labriola M, Christensen KB, Bultmann U, Villadsen E. Return to work among
sickness-absent Danish employees: prospective results from the Danish Work
Environment Cohort Study/National Register on Social Transfer Payments.
International Journal of Rehabilitation Research 2006;29(3):229-35.
28. Bartley M, Sacker A, Clarke P. Employment status, employment conditions, and
limiting illness: prospective evidence from the British household panel survey
1991-2001.
Journal of Epidemiology & Community Health 2004;58(6):501-6.
29. Shaw WS, Huang Y-H. Concerns and expectations about returning to work with low
back pain: identifying themes from focus groups and semi-structured interviews.
Disability & Rehabilitation 2005;27(21):1269-81.
30. Fayad F, Lefevre-Colau MM, Poiraudeau S, Fermanian J, Rannou F, Wlodyka Demaille
S, et al. [Chronicity, recurrence, and return to work in low back pain: common
prognostic factors].
Annales de Readaptation et de Medecine Physique 2004;47(4):179-89.
31. Loisel P, Durand MJ, Berthelette D, Vezina N, Baril R, Gagnon D, et al. Disability
prevention - new paradigm for the mangement of occupational back pain.
Dis
Manage Health Outcomes 2001;9:351-360.
32. Franche R-L. Workplace-Based Return-to-Work Interventions: Optimiziing the Role of
Stakeholders in Implementation and Research.
Journal of Occupational
Rehabilitation 2005;15(4).
33. Loisel P, Buchbinder R, Hazard R, Keller R, Scheel I, van Tulder M, et al. Prevention of
work disability due to musculoskeletal disorders: the challenge of implementing
evidence.
Journal of Occupational Rehabilitation 2005;15(4):507-24.
34. Westmorland MG, Buys N. A comparison of disability management practices in
Australian and Canadian workplaces.
Work 2004;23(1):31-41.
35. Steenstra IA, Anema JR, van Tulder MW, Bongers PM, de Vet HCW, van Mechelen W.
Economic evaluation of a multi-stage return to work program for workers on sick-
leave due to low back pain.
Journal of Occupational Rehabilitation 2006;16(4):557-
78.
36. Streibelt M, Hansmeier T, Muller-Fahrnow W. [Effects of work-related medical
rehabilitation in patients with musculoskeletal disorders].
Rehabilitation
2006;45(3):161-71.
37. Streibelt M, Blume C, Thren K, Muller-Fahrnow W. [Economic evaluation of medically
occupationally orientated rehabilitation in patients with musculoskeletal disorders-
-a cost-benefit analysis from the perspective of the German statutory pension
insurance scheme].
Rehabilitation 2008;47(3):150-7.
38. Franche R-L, Cullen K, Clarke J, Irvin E, Sinclair S, Frank J, et al. Workplace-based
return-to-work interventions: a systematic review of the quantitative literature.
Journal of Occupational Rehabilitation 2005;15(4):607-31.
39. Bontoux L, Roquelaure Y, Billabert C, Dubus V, Sancho PO, Colin D, et al.
[Prospective study of the outcome at one year of patients with chronic low back
pain in a program of intensive functional restoration and ergonomic intervention.
A c c i d e n t C o m p e n s a t i o n C o r p o r a t i o n
Page 12
Factors predicting their return to work].
Annales de Readaptation et de Medecine
Physique 2004;47(8):563-72.
40. Mallon TM, Cloeren M, Firestone LM, Burch HC. Contract case managers prove cost
effective in federal workers' compensation programs.
Military Medicine
2008;173(3):253-8.
41. Lai H-S, Chan CCH. Implementing a pilot work injury management program in Hong
Kong.
Journal of Occupational Rehabilitation 2007;17(4):712-26.
42. Meijer EM, Sluiter JK, Frings-Dresen MHW. Evaluation of effective return-to-work
treatment programs for sick-listed patients with non-specific musculoskeletal
complaints: a systematic review.
International Archives of Occupational &
Environmental Health 2005;78(7):523-32.
43. Gross DP, Battie MC. Functional capacity evaluation performance does not predict
sustained return to work in claimants with chronic back pain.
Journal of
Occupational Rehabilitation 2005;15(3):285-94.
44. Gross DP, Battie MC. Does functional capacity evaluation predict recovery in workers'
compensation claimants with upper extremity disorders?
Occupational &
Environmental Medicine 2006;63(6):404-10.
45. Gross DP, Battie MC, Cassidy JD. The prognostic value of functional capacity
evaluation in patients with chronic low back pain: part 1: timely return to
work.[see comment].
Spine 2004;29(8):914-9.
46. Pransky G, Shaw W. Return to work-from research to practice.
Journal of Occupational
& Environmental Medicine 2007;49(3):249-51.
47. Iles RA, Davidson M, Taylor NF. Psychosocial predictors of failure to return to work in
non-chronic non-specific low back pain: a systematic review.
Occupational &
Environmental Medicine 2008;65(8):507-17.
48. Heijbel B, Josephson M, Jensen I, Stark S, Vingard E. Return to work expectation
predicts work in chronic musculoskeletal and behavioral health disorders:
prospective study with clinical implications.
Journal of Occupational Rehabilitation
2006;16(2):173-84.
49. Larsson A, Karlqvist L, Gard G. Effects of work ability and health promoting
interventions for women with musculoskeletal symptoms: a 9-month prospective
study.
BMC Musculoskeletal Disorders 2008;9:105.
50. van Weel C, Orbon K, van der Gulden J, Buijs P, Folgering H, Thoonen B, et al.
Occupational health and general practice: from opportunities lost to opportunities
capitalised?
Medicina del Lavoro 2006;97(2):288-94.
51. Millward LJ, Lutte A, Purvis RG. Depression and the perpetuation of an incapacitated
identity as an inhibitor of return to work.
Journal of Psychiatric & Mental Health
Nursing 2005;12(5):565-73.
52. Labriola M, Lund T, Christensen KB, Albertsen K, Bultmann U, Jensen JN, et al. Does
self-efficacy predict return-to-work after sickness absence? A prospective study
among 930 employees with sickness absence for three weeks or more.
Work
2007;29(3):233-8.
53. Bonde JP, Rasmussen MS, Hjollund H, Svendsen SW, Kolstad HA, Jensen LD, et al.
Occupational disorders and return to work: a randomized controlled study.
Journal
of Rehabilitation Medicine 2005;37(4):230-5.
54. Drews B, Nielsen CV, Rasmussen MS, Hjort J, Bonde JP. Improving motivation and
goal setting for return to work in a population on sick leave: a controlled study.
Scandinavian Journal of Public Health 2007;35(1):86-94.
55. Sullivan MJL, Feuerstein M, Gatchel RJ, Linton SJ, Pransky G. Integrating Psychosocial
and Behavioural Interventions to Achieve Optimal Rehabilitation Outcomes.
Journal of Occupational Rehabilitation 2005;15(4):475-489.
A c c i d e n t C o m p e n s a t i o n C o r p o r a t i o n
Page 13
56. Amaral RAd, Malbergiera A. [Evaluation of a screening test for alcohol-related
problems (CAGE) among employees of the Campus of the University of Sao
Paulo].
Revista Brasileira de Psiquiatria 2004;26(3):156-63.
57. Fernandez WG, Hartman R, Olshaker J. Brief interventions to reduce harmful alcohol
use among military personnel: lessons learned from the civilian experience.
Military Medicine 2006;171(6):538-43.
58. Mariotti O. [Drug addiction and working].
Giornale Italiano di Medicina del Lavoro Ed
Ergonomia 2004;26(3):247-50.
59. Halcomb E, Daly J, Davidson P, Elliott D, Griffiths R. Life beyond severe traumatic
injury: an integrative review of the literature.
Australian Critical Care 2005;18(1):17-8.
60. Barrett B, Byford S, Crawford MJ, Patton R, Drummond C, Henry JA, et al. Cost-
effectiveness of screening and referral to an alcohol health worker in alcohol
misusing patients attending an accident and emergency department: a decision-
making approach.
Drug & Alcohol Dependence 2006;81(1):47-54.
61. Drebing C, Van Ormer E, Krebs C, Rosenheck R, Rounsaville B, Herz L, et al. The
impact of enhanced incentives on vocational rehabilitation outcomes for dually
diagnosed veterans.
Journal of applied behavior analysis. 2005;38(3):359-72.
62. Miller TR, Zaloshnja E, Spicer RS. Effectiveness and benefit-cost of peer-based
workplace substance abuse prevention coupled with random testing.
Accident
Analysis & Prevention 2007;39(3):565-73.
63. Spicer RS, Miller TR. Impact of a workplace peer-focused substance abuse prevention
and early intervention program.
Alcoholism: Clinical & Experimental Research
2005;29(4):609-11.
64. Vungkhanching M, Heinemann AW, Langley MJ, Ridgely M, Kramer KM. Feasibility of
a skills-based substance abuse prevention program following traumatic brain
injury.
Journal of Head Trauma Rehabilitation 2007;22(3):167-76.
A c c i d e n t C o m p e n s a t i o n C o r p o r a t i o n
Page 14
Document Outline